
Abstract
Microtubules (MTs) are intracellular polymers that provide structure to the cell, serve as railways for intracellular transport, and regulate many cellular activities, including cell migration. The dynamicity and function of the MT cytoskeleton are determined in large part by its regulatory proteins, including the recently discovered MT severing enzyme Fidgetin-like 2 (FL2). Downregulation of FL2 expression with small interfering RNA (siRNA) results in a more than twofold increase in cell migration rate in vitro as well as translates into improved wound-healing outcomes in in vivo mouse models. Here we utilized a commercially available surfactant polymer dressing (SPD) as a vehicle to deliver FL2 siRNA. To this end we incorporated collagen microparticles containing FL2 siRNA into SPD (SPD-FL2-siRNA) for direct application to the injury site. Topical application of SPD-FL2 siRNA to murine models of full-thickness excision wounds and full-thickness burn wounds resulted in significant improvements in the rate and quality of wound healing, as measured clinically and histologically, compared with controls. Wound healing occurred more rapidly and with high fidelity, resulting in properly organized collagen substructure. Taken together, these findings indicate that the incorporation of FL2 siRNA into existing treatment options is a promising avenue to improve wound outcomes.

Introduction
W
Our previous work that involved screening of biological agents for cell migration phenotypes identified a novel regulator of the microtubule (MT) cytoskeleton, termed Fidgetin-like 2 (FL2), as an important negative regulator of cell migration. 12 siRNA-mediated depletion of FL2 results in a significant increase in the velocity and directionality of keratinocyte and fibroblast motility in vitro. 12 Moreover, we found that in vivo depletion of FL2 strongly promoted wound closure and repair. Of note, FL2 depletion enhanced healing by inducing a targeted, transient disruption of cortical MT within the leading edge of fibroblasts and keratinocytes. 12 This localized alteration bypasses the manipulation of larger signaling cascades, which have been shown to induce numerous unintended side effects. 3,5,13 Having identified FL2 as a promising therapeutic target we began development of an SPD containing FL2 siRNA.
As poloxamer technology has matured, commercially available SPDs are more widely used. We identified one biocompatible and nonionic SPD containing poloxamer 188 as a candidate for siRNA incorporation. 14 This SPD has previously been shown to improve wound-healing outcomes (improved wound closure rates, reduction of inflammation, pain, and odor) in nonhealing wounds and is now in a U.S.-based clinical trial to determine its efficacy in the treatment of wounds of mixed etiologies. 15,16 Looking to utilize the complimentary healing mechanisms of FL2 siRNA and SPD, we synthesized collagen microparticles containing FL2 siRNA and incorporated these into the SPD for topical application in two in vivo wound-healing models.
Here, we demonstrate that the incorporation of FL2 siRNA collagen microparticles into SPD (SPD-FL2-siRNA) significantly enhances healing outcomes compared with controls (SPD without microparticles and SPD-Control-siRNA), as measured clinically and histologically in two murine wound-healing models, namely full-thickness excision and full-thickness burn. Following SPD-FL2-siRNA treatment, there was a decrease in inflammation and an increase in revascularization at the wound site, while cell proliferation was unaffected. Wound healing occurred more rapidly and with high fidelity, resulting in properly organized collagen substructure. Taken together, these findings indicate that the incorporation of FL2 siRNA into existing treatment options is a promising avenue to improve wound management.
Clinical Problem Addressed
Slow healing and open wounds are a serious medical problem faced by patients worldwide. Without proper re-epithelialization, these wounds are at risk of infection, increasing the risk of amputation or mortality. Slow-healing wounds also bring the risk of scarring and skin deformation. 17 A therapeutic that can more quickly close wounds would directly address these issues.
Materials and Methods
Surfactant polymer dressing
A nonionic SPD (PluroGel®; Medline Industries, Inc.) was used for siRNA delivery.
siRNA
Sequences targeting mouse FL2 messenger RNA (mRNA) (SASI_Mm02_00354635; Sigma-Aldrich) or a nontargeting negative control siRNA (SIC001; Sigma-Aldrich) were used.
Collagen microparticle and SPD incorporation
Ten grams of sodium bis(2-ethylhexyl) sulfosuccinate (AOT; Sigma-Aldrich) was dissolved in 34 mL n-hexane, and 2 mL 5% collagen-I dissolved in acetic acid was added. The resulting microemulsion was stirred for 45 min until it became clear. This solution was then evaporated to remove hexane. The residue was washed and then suspended in nuclease-free water and lyophilized. Then 100 mg of lyophilized powder was then treated with 1,000 μL of 25 μM siRNA solution and relyophilized. This material was then suspended in 1.25 mL SPD, at 4°C for 2 h, and then lyophilized. The lyophilized powder was then added with 1.25 mL nuclease-free water and 1.25 mL SPD.
In vivo studies
Animal experiments were performed according to the guidelines published by the Institute of Laboratory Animal Resources of National Research Council, and animal care for this study was approved by the Institutional Animal Care and Use Committee of the Albert Einstein College of Medicine.
Punch biopsy excision
Before procedures, mice were anesthetized with a ketamine–xylazine cocktail. Female Balb/c mice (6–8 weeks; National Cancer Institute, Frederick, MD) were shaved and then wounded uniformly on their dorsa using a 5 mm punch biopsy tool. 12 To counteract wound contraction typically seen in mice, we used an established silicone splinting method to encourage the formation of granulation tissue and re-epithelialization. 18 Splints were checked multiple times a day during the study and replaced as needed. Wounds were treated with 10 μL of SPD, SPD-Control-siRNA, or SPD-FL2-siRNA on days 0, 2, and 4.
Burn protocol
Before procedures, mice were anesthetized with a ketamine–xylazine cocktail. Female Balb/c mice (6–8 weeks; National Cancer Institute, Frederick, MD) were shaved and then burned uniformly on their dorsa using a 5 mm brass probe heated to 100°C. 12,19 Mice were provided buprenorphine as needed following injury. Wounds were treated with 10 μL of SPD, SPD-Control-siRNA, or SPD-FL2-siRNA on days 0, 2, and 4.
Wound measurements
Wounds were measured by investigators blinded to the treatment groups using surgical calipers. Measurements were made in four planes (N-S, W-E, NE-SW, NW-SE), tabulated, and compared with day 0. 18 Histologically, wound edges were defined by the distance between the first hair follicle encountered at each end of the wound.
Histochemistry
Wound sites were harvested, fixed overnight in HistoChoice, bisected through the center of the wound, and embedded in paraffin blocks. Seven-micrometer sections were cut and slides were deparaffinized, washed in phosphate buffered saline (PBS)-0.01% TritonX100, unmasked with antigen retrieval buffer tris(hydroxymethyl)aminomethane/ethylenediaminetetraacetic acid pH 9.0, and blocked with 5% normal goat serum in PBS. Sections were stained overnight with their respective antibody and visualized using a 3,3′-diaminobenzidine (DAB) kit (Vector Labs).
Microscopy
Whole wound sections were imaged with a P250 High Capacity Slide Scanner (3D Histech) using brightfield with a 20 × air objective, numerical aperture 0.8, and complementary metal–oxide semiconductor (CMOS) color camera (VCC-FC60FR19CL; CIS Corp.). Measurements of wound sizes were made using the CaseViewer analysis software (3D Histech). The size of wounds was determined by measuring the maximum length between wound edges. Quantifications of proliferating cell nuclear antigen (PCNA), cluster of differentiation 45 (CD45), and platelet endothelial cell adhesion molecule-1 (PECAM1) were conducted as described elsewhere. 20,21 Herovici analysis was conducted following a previously described approach. 22,23
Statistical analysis
Data are expressed as mean ± standard error of the mean. Differences between treatment groups were calculated using unpaired Student's, Mann–Whitney nonparametric t-tests, or two-way analysis of variances. Significance was set at p < 0.05.
Commercial antibodies and stains
Commercially produced antibodies used in immunohistochemistry included PECAM-1 (1:50; ab28364; Abcam), CD45 (1:200; ab10558; Abcam), PCNA (1:1,000; ab152112; Abcam), and Keratin 14 (1:500; 906004; BioLegend). Alternatively, sections were stained with hematoxylin (#3530-32; Ricca Chemical Company) and eosin (#17372-87-1; Acros Organics) or Herovici (#KTHER; American MasterTech) following the manufacturer's suggested protocol.
Quantitative PCR
Skin of SPD, SPD-Control-siRNA, and SPD-FL2-siRNA–treated mice was excised at set time points after wounding. The Next Advance Bullet Blender was used to pulverize the tissue, and RNA was extracted with Trizol reagent (15596-026; Invitrogen). Complementary DNA was synthesized the same day using the SuperScript IV First-strand synthesis system (18091050; Invitrogen). Quantitative PCR (qPCR) was performed using Life Technologies Universal Master Mix II (4440040) with FIGNL2 primers (Mm.PT.58.21940655; IDT Technologies). ActB (actin) served as the reference gene (Mm.PT.58.33540333; IDT Technologies). Resulting data were quantified using the comparative 2–ΔΔCt method. The average of control skin wounds was normalized to 1 and used for relative quantification.
Results
SPD-FL2-siRNA knocks down FL2 messenger RNA abundance
Delivery of FL2-targeting siRNA to the cells within the wound zone was achieved by direct topical application of our therapeutic surfactant polymer containing siRNA microparticles (Fig. 1A). Reduction of FL2 levels was confirmed by qPCR analysis on injured skin 3 days post initial treatment (Fig. 1B). Wounds that received FL2 siRNA had a 51% reduction in FL2 mRNA levels compared with their control counterpart (SPD with collagen microparticles containing nontargeting siRNA). These data indicate that FL2 siRNA was effectively being delivered and was causing degradation of FL2 mRNA transcripts at the site of application.
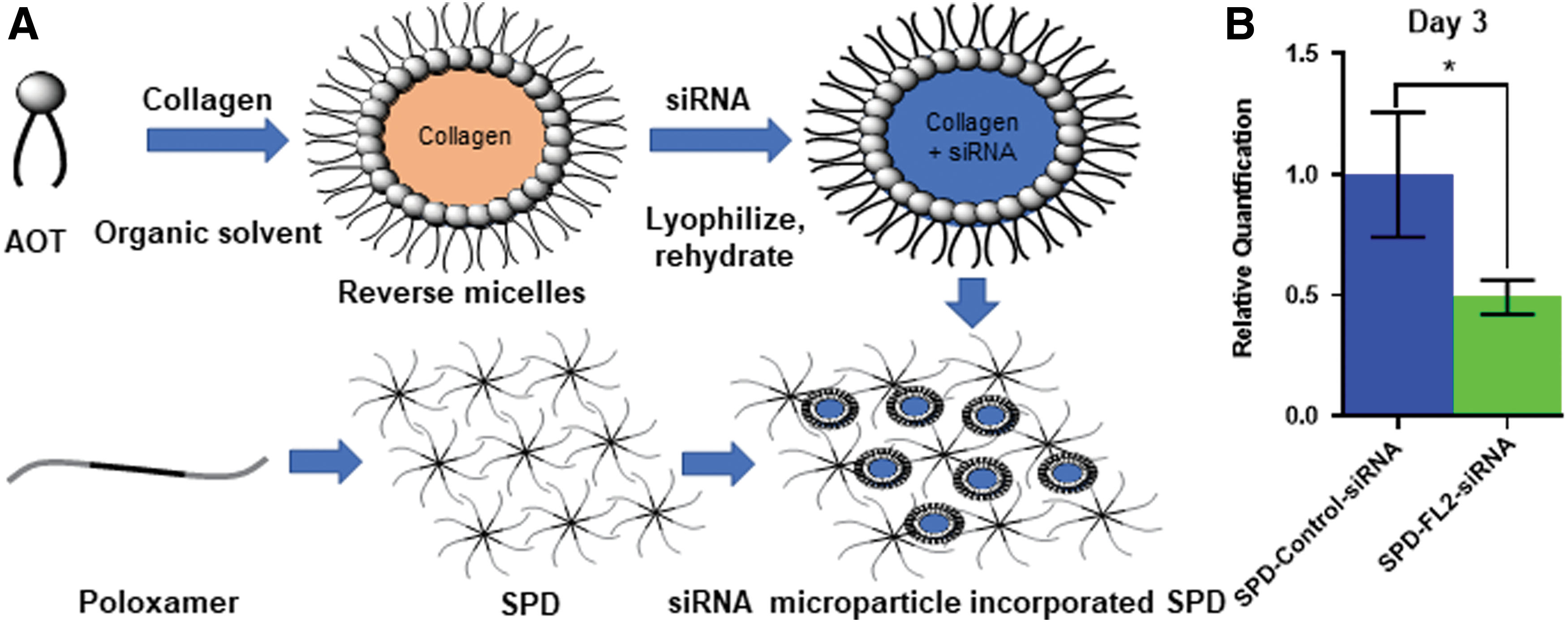
FL2 levels are reduced in injured skin treated with SPD-FL2-siRNA.
SPD-FL2-siRNA expedites excisional wound re-epithelialization
Following full-thickness excision, significant improvements in wound size were first noted in SPD-FL2-siRNA–treated wounds 3 days post wounding (Fig. 2A, B). On day 4, open wound areas of SPD alone and SPD-Control-siRNA–treated mice (21.8% and 23.7% open, respectively) were nearly twice the size of SPD-FL2-siRNA–treated wounds (11.04% open; n = 22 wounds per group; Fig. 2C). Treatments continued through day 6 at which point wounds became too small to measure.
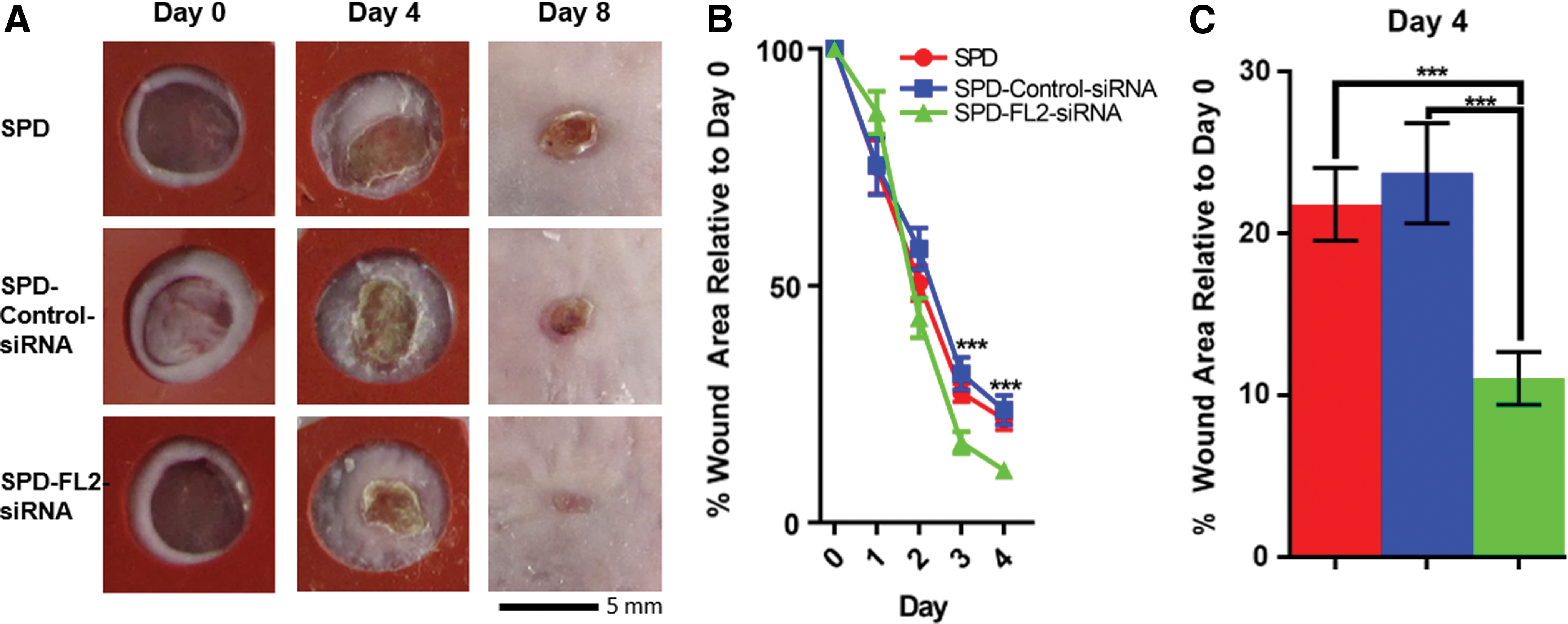
SPD-FL2-siRNA treatment stimulates healing in a mouse full-thickness excision model.
Histological analysis of wounds confirmed a significant reduction in wound size following SPD-FL2-siRNA treatment; SPD-FL2-siRNA wounds were reduced to about half the length of controls (average wound length of 2.5 ± 0.2 mm for SPD, 2.4 ± 0.3 mm for SPD-Control-siRNA, and 1.2 ± 0.3 mm for SPD-FL2-siRNA treatments, respectively; Fig. 3A, B). Furthermore, we noted that in a few cases (2 out of 7), SPD-FL2-siRNA–treated wounds had hair follicles present within the wound zone, as confirmed by keratin 14 staining (Fig. 3A inset). No such structures were observed in controls. These clinical and histological assessments indicate that SPD-FL2-siRNA was more effectively stimulating re-epithelialization and regeneration following full-thickness excision compared with controls.
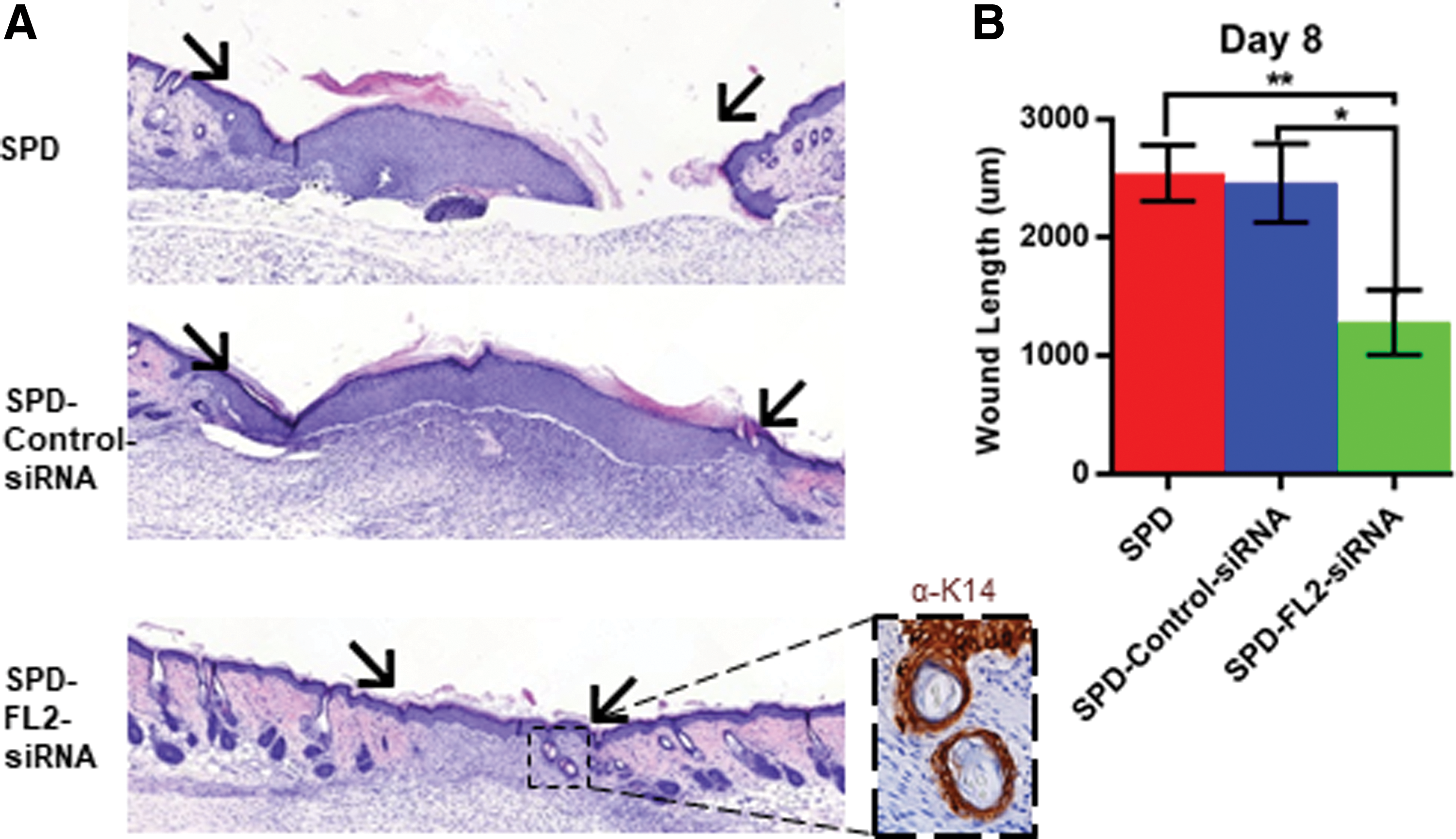
SPD-FL2-siRNA treatment reduces wound size in mouse full-thickness excision model.
SPD-FL2-siRNA improves burn wound healing
The effect of SPD-FL2-siRNA on wound healing was further tested in a full-thickness burn model. Burns were measured by two investigators blinded to the treatment groups using surgical calipers every day and tracked until closure (Fig. 4A, B). The wound sites enlarged in size for 4 days post injury, increasing up to 215% the size of the original burn area in control groups. SPD-FL2-siRNA–treated burns, however, did not enlarge as dramatically, reaching a maximum of 160% the size of the original burn area. The reduced burn expansion was followed by significantly improved healing from day 4 to 9 compared with SPD and SPD-Control-siRNA–treated burns (Fig. 4B, C). Due to scabbing, burns became too difficult to measure using surgical calipers following day 9.
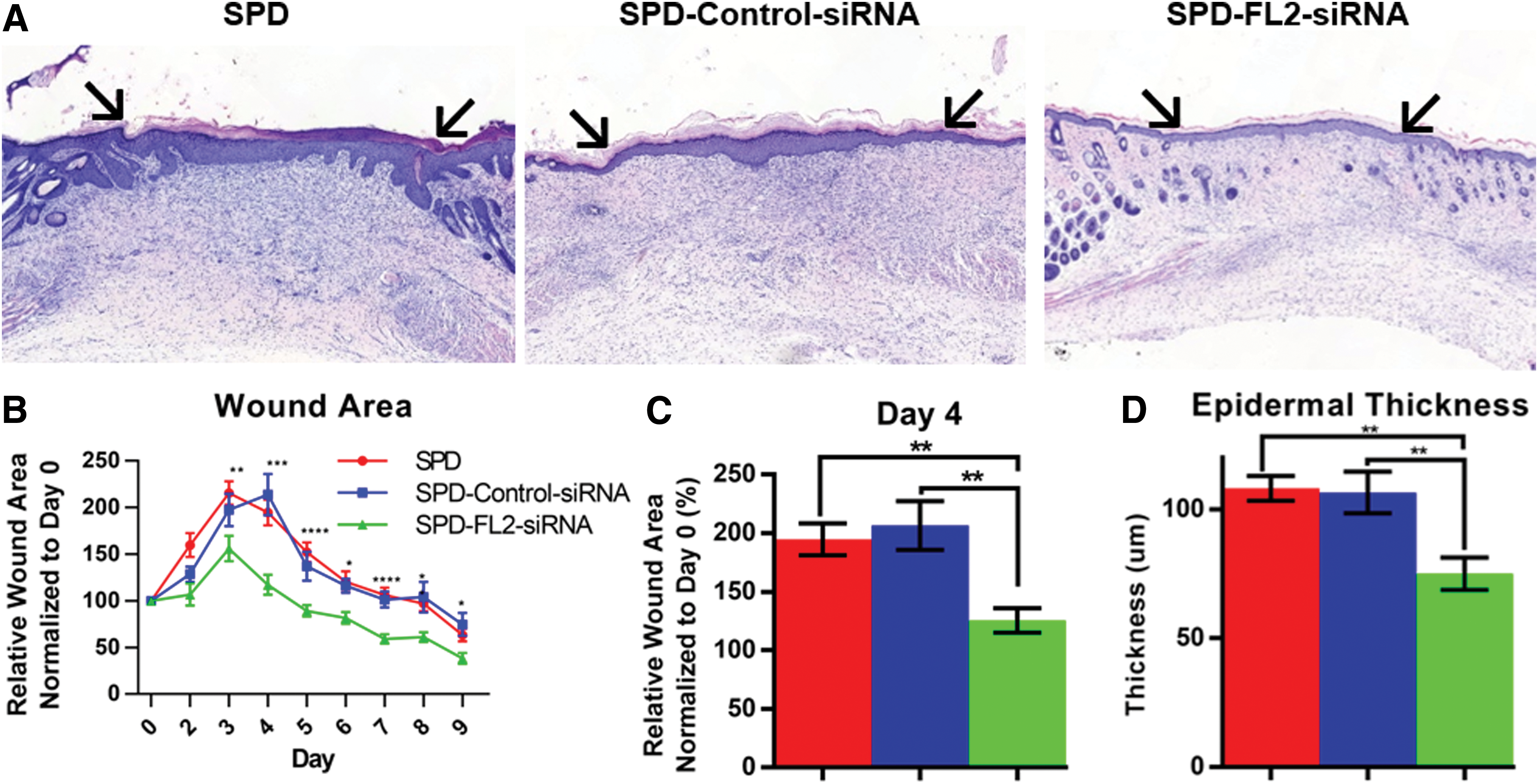
SPD-FL2-siRNA treatment stimulates healing in mouse full-thickness burn model.
Histological analysis of wound tissue 14 days post injury showed that SPD-FL2-siRNA–treated burns underwent a significant reduction in burn wound area (SPD and SPD-Control-siRNA were 35.5% and 39.3% larger, respectively; data not shown). All SPD-FL2-siRNA–treated burns had closed completely at day 14, whereas 25% and 30% of SPD and SPD-Control-siRNA–treated wounds, respectively, remained unhealed (data not shown). Furthermore, SPD-FL2-siRNA–treated burns had a significant reduction in epidermal thickness compared with controls, more closely resembling normal skin (Fig. 4D). These clinical and histological assessments indicate that SPD-FL2-siRNA promotes re-epithelialization and regeneration of wound tissue following full-thickness burns.
SPD-FL2-siRNA improves regeneration of the skin
We next characterized the quality of regenerated tissue through immunohistochemical staining.
First we looked to define FL2's role in cell proliferation as an increase in cell proliferation could potentially account for the shortened re-epithelialization time. PCNA staining of burn wound sections revealed that there was no significant difference in the percentage of PCNA-positive cells between the three treatment groups (Fig. 5A, B). These data indicate that FL2 knockdown does not affect cell proliferation during healing and suggests that cell migration is the likely driver of hastened re-epithelialization compared with controls.
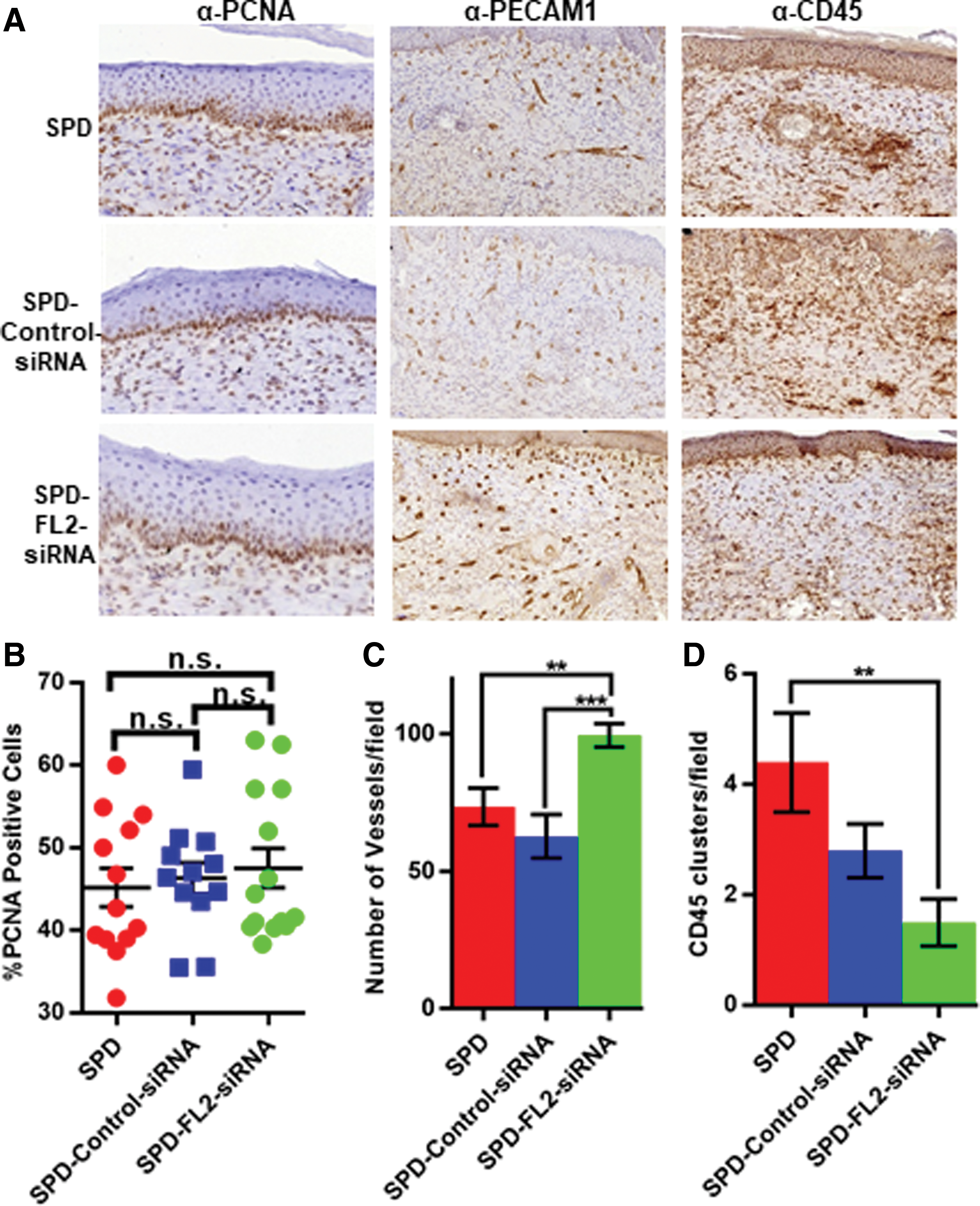
FL2 knockdown enhances revascularization and reduces inflammation without affecting cell proliferation.
Managing inflammation is an essential process for effective wound healing. To assess the impact of FL2 knockdown on inflammatory cell presence at day 14, sections were stained for CD45, a marker of leukocytes and other immune cells. CD45 staining was present in all three treatment groups. However, we observed that SPD-FL2-siRNA–treated wounds contained fewer distinct clusters of CD45-positive cells within the burn zone than SPD and SPD-Control-siRNA groups (Fig. 5A, C). After day 7, reduction of CD45-positive cells was indicative of a return to baseline conditions. 21
Revascularization of the burn zone was quantified by PECAM1 staining. Significantly more vessels per field were present in SPD-FL2-siRNA–treated wounds (99.5 ± 4.3 vessels per field) than SPD and SPD-Control-siRNA treatments (73.5 ± 6.8 and 62.7 ± 7.9 vessels per field, respectively; Fig. 5A, D). This data suggest that FL2 knockdown may enhance angiogenesis in wounded skin to provide oxygen and nutrients to the wound site for use in the rapidly regenerating wound zone.
SPD-FL2-siRNA affects collagen III to collagen I ratios in burn scars
In the early stages of wound healing, myofibroblasts deposit collagen III in the wound zone, increasing the ratio of collagen III to collagen I. Collagen III accounts for up to 50% of total collagen in the early stages of wound healing, up from levels in uninjured skin by about 20%. 24 As the scar matures, the ratio of collagen III to collagen I decreases to approximate normal levels.
To determine whether FL2 knockdown influences the ratio of collagen III to collagen I during burn healing, burns were analyzed using Herovici stains. Herovici is routinely used to quantify the ratio of collagen I (which stains red) and III (which stains blue) through multispectral imaging. Our results indicate that there were increased levels of mature collagen (reduction in collagen III to collagen I ratio) in SPD-FL2-siRNA–treated burn tissues, which further supports our hypothesis that FL2 knockdown accelerates wound healing.
Discussion
Treating wounds with a SPD provides significant hydration to the wound site and increases antimicrobial efficacy, improving healing outcomes. The data shown here support our hypothesis that the incorporation of FL2 siRNA, a therapeutic with a complimentary healing mechanism, into an SPD further improves wound-healing outcomes. Further development of alternative SPD formulations and optimization of dosing regimens is an area ripe for future investigation. 25
Improving current therapeutic options with FL2-targeting siRNA
Several wound-healing models, including dermal (excisional and burns), ocular (abrasions and burns), and 3D co-cultures of keratinocytes and fibroblasts, have underscored the importance of rapid re-epithelialization as a key determinant of effective healing outcomes. 26 –32 The clinical and histological characterization of treated wounds presented above indicate that SPD-FL2-siRNA stimulates more efficient re-epithelialization and progresses wounds into subsequent stages of healing (resolution of inflammation) and regeneration (collagen maturation, angiogenesis) more quickly than controls.
The extent of inflammatory response following injury is a first indicator of potential wound outcome. 33 It is noteworthy that SPD-FL2-siRNA–treated wounds show an expedited resolution of inflammation at earlier time points (Fig. 4B) and reduced CD45+ staining at later points (Fig. 5A); there is now evidence that more effective re-epithelialization is correlated with shortened periods of inflammation and that reduced CD45+ levels 7 days post injury is indicative of further progressed wounds. 21,34,35 Next, as re-epithelialization continues, leading edge cells generate a “healing” scaffold into the wound zone. This structure creates a path for cells to efficiently migrate to the center of the wound and begin remodeling the extracellular matrix. 36 Our findings here show that FL2 knockdown influences collagen organization within the wound zone, reducing the ratio of collagen III to collagen I in treated wounds (Fig. 6). While increased deposition of collagen III is known to reduce the density of blood vessels within the wound, 37 collagen I is an optimal substrate for endothelial cells, and this may explain the increase in angiogenesis seen in SPD-FL2-siRNA–treated wounds (Fig. 5). 38,39 Additional cell types such as epidermal stem cells also utilize this newly formed scaffold to migrate into the wound zone. 36 We found that only FL2 siRNA–treated wounds showed stem cell–derived hair follicles within the wound zone, suggesting that these wounds were further progressed in the regeneration process (Fig. 3). Re-epithelialization also impacts local cellular signaling within the wound zone. Increasingly abundant keratinocytes release VEGF, recruiting endothelial cells into the wound zone, and may provide an alternative explanation for the increased angiogenesis seen in SPD-FL2-siRNA–treated wounds. 40 Additional studies will be needed to define these processes more completely.
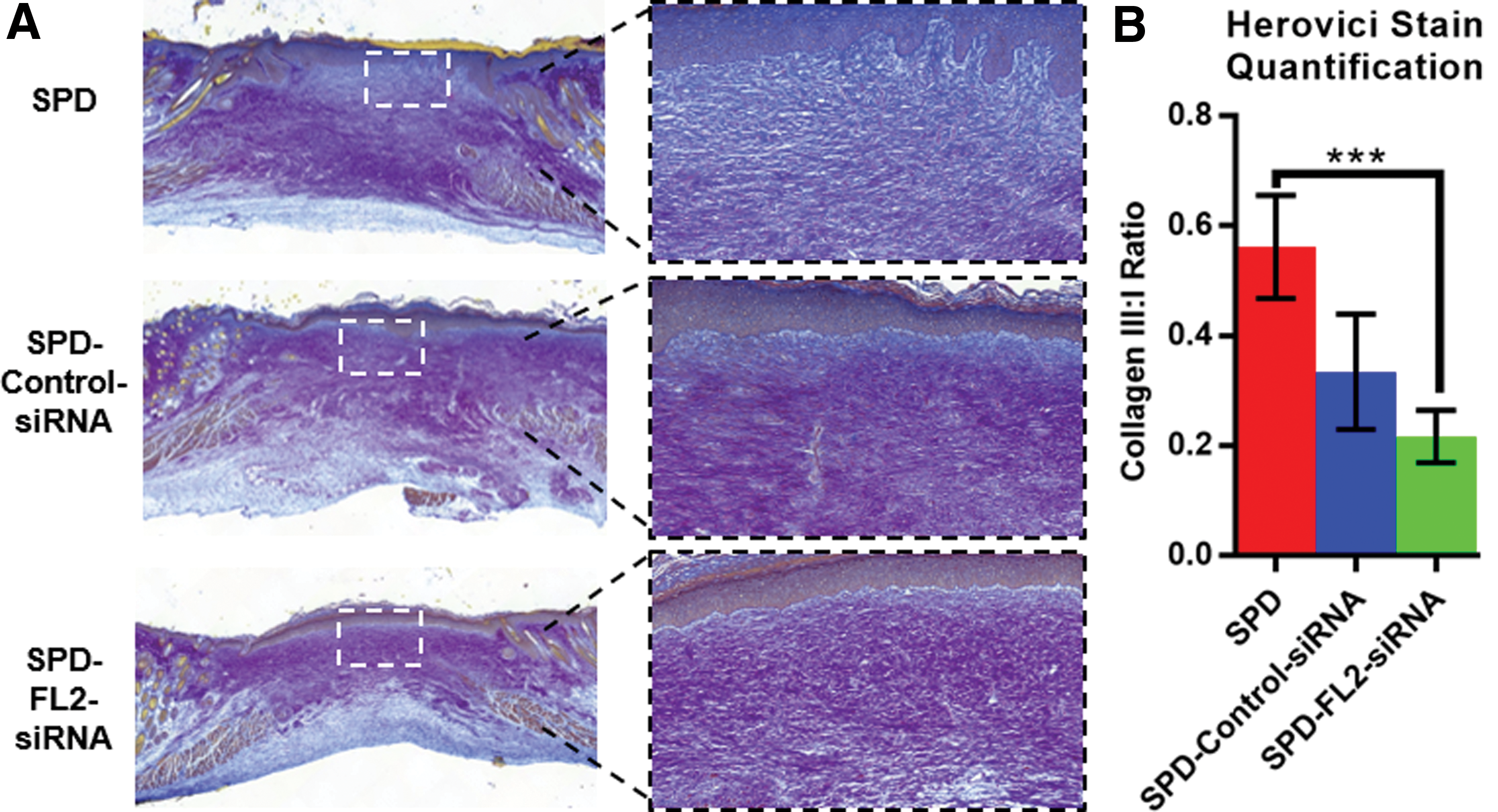
SPD-FL2-siRNA treatment enhances collagen remodeling in mouse full-thickness burn model.
In conclusion, we present a new SPD-siRNA platform that can be applied topically and used to treat excision wounds and burns. Treatment with SPD-FL2-siRNA depletes FL2 levels, which expedites re-epithelialization and ultimately improves dermal structure compared with treatment with SPD alone. Due to its favorable chemical composition and ease of application, an SPD-FL2-siRNA product could improve the lives of patients suffering from a variety of dermal injuries.
Innovation
Here we incorporated siRNA into SPD for use on cutaneous burns and excisions. To our knowledge this is the first time siRNA in collagen microparticles has been incorporated into SPD. While previous formulations of particles have been used to encapsulate siRNA, the platform presented herein has several advantages. SPD is biocompatible, nonionic, hydrating, and able to remain at the site of application. SPD also has noted anti-biofilm properties, helping to ward off infection and allowing wounds to heal. Combining SPD with the synergistic FL2 siRNA allows for the therapeutic use of both healing mechanisms.
FL2 siRNA can be incorporated into current treatment options to further improve healing outcomes.
The use of SPD improves the ease of application of FL2-siRNA.
Collagen microparticles in SPD is a viable platform for testing alternative therapeutic siRNAs in wound-healing contexts.
Footnotes
Acknowledgments and Funding Sources
This work was supported in part by a grant from the Wound Healing Foundation. We would also like to acknowledge Einstein Analytical Imaging Facility (AIF) for expert advice/assistance in microscopy. The AIF is funded by the NCI Cancer Grant P30CA013330. Imaging was conducted using the 3DHistec Pannoramic 250 Flash II slide scanner, which was funded by the NIH 1S10OD019961-01. A.H.K. is partially supported by the National Research Foundation of South Africa.
Author Disclosure and Ghostwriting
B.O.R. is an employee of MicroCures, Inc. J.N. is a scientific advisor for MicroCures, Inc. D.J.S. is the founder and Chief Science Officer of MicroCures, Inc. D.J.S. is the owner of U.S. Patent #20130022667 entitled “Fidgetin-like 2 as a target to enhance wound healing,” which has been licensed by MicroCures. No other author has a conflict of interest. No ghostwriters were used to write this article.
About the Authors