
Abstract
Background & Aims:
Although incisional hernia repair in women of childbearing age is not rare, hernia disease in this group of patients is sparsely documented. The aim of this study was to examine long-term clinical results after incisional hernia repair in women of childbearing age.
Material and methods:
This nationwide cohort study examined incisional hernia repair from 2007 to 2013 in women of childbearing age, registered prospectively in the Danish Ventral Hernia Database. All women with a subsequent pregnancy were included, and a 1:3 propensity-score matched group of women with an incisional hernia repair without a subsequent pregnancy. A prospective follow-up was conducted, including a validated questionnaire. The primary outcome was recurrence, and the secondary outcome was chronic pain from the operated site.
Results:
In total, 124 (70.5%) women responded, 47 and 77 women with and without a subsequent pregnancy, respectively. The 5-year cumulative incidence of recurrence was 41.0% (95% confidence interval 32.0%–49.9%). After adjustment for potential confounders, subsequent pregnancy was independently associated with recurrence (hazard ratio 1.83, 95% confidence interval 1.02–3.29, p = 0.044). Twenty-six (21.0%) women reported chronic pain (moderate, n = 21; severe, n = 5) with no difference between women with and without a subsequent pregnancy. Hernia recurrence, higher body mass index, and smoking were associated with chronic pain.
Conclusion:
Pregnancy following incisional hernia repair was associated with an increased risk of recurrence, but not with chronic pain.
Keywords
Introduction
Incisional hernia is reported in 12%–22% of patients following abdominal surgery (1). Consequently, incisional hernia repair is a common procedure with about 350,000 repairs performed annually in the United States (2). Approximately every tenth patient undergoing incisional hernia repair is a woman of childbearing age (3). However, there is only sparse evidence on the risk of recurrence and chronic pain in women with an incisional hernia repair and a subsequent pregnancy (3). Both recurrence and chronic pain have previously been associated with decreased patient satisfaction and quality of life following incisional hernia repair (4, 5).
The abdominal wall is strained during pregnancy, and two previous studies have reported that a pregnancy following ventral hernia repair was associated with recurrence (6, 7). However, both of these studies were based on registration of recurrence from administrative data, whereas a validated questionnaire was used for follow-up in the present study. Other outcomes, such as chronic pain, have only been documented in case reports or smaller case-series (8).
The aim of this nationwide prospective cohort study was to examine long-term clinical results after incisional hernia repair in women of childbearing age and compare women with and without a subsequent pregnancy. The primary outcome was recurrence, and the secondary outcome was chronic pain from the operated site.
Material and Methods
This was a prospective cohort study reported according to the STROBE checklist (9). The Danish Ventral Hernia Database was queried for incisional hernia repairs (index repairs) on women aged 15–45 years old between 1 January 2007 and 31 December 2013. In the present study, an incisional hernia was defined as a first-time incisional hernia (including trocar-site hernias) and any recurrent ventral hernia, in accordance with the European Hernia Society classification (10). Parastomal hernia repairs were excluded. The data were merged with the Danish Medical Birth Registry (DMBR) to identify childbirths following the index repair within the study inclusion period (i.e. until 31 December 2013). All childbirths, including home births are registered in the DMBR (11). A study on registry-based outcomes on this cohort has previously been published (7). In Denmark, all residents are given a unique personal identification number at birth or time of immigration, which is used throughout the health care sector. This system enables reliable cross-linking between medical registries and databases at an individual level. The final study cohort consisted of all women who had given birth subsequently, and a 3:1 matched group of women who had not been pregnant subsequently. The women were sent a mailed questionnaire in January 2018. The questionnaire was resent twice to non-responders, followed by up to three telephone contact attempts. The questionnaire has previously been validated to identify recurrence following ventral hernia repair (sensitivity and specificity of 0.86 and 0.78, respectively) (12). Doubt of recurrence was resolved by a previously published standardized telephone interview protocol (sensitivity and specificity of 1.00 and 0.86, respectively) (13). Furthermore, the questionnaire included questions on smoking habits at time of index repair, current height and weight, and chronic pain (none, mild, moderate, or severe pain from the operated site during the last week). The matched control group of women who had not been pregnant after the index repair were asked for date of any childbirth, to identify pregnancies after 31 December 2013. Women who reported a subsequent childbirth during follow-up were reassigned to the pregnancy-exposed group. Women who reported both recurrence and a subsequent pregnancy were asked about the timely relation of these events, in order to ensure correct exposure classification.
Variables and Outcomes
All Danish surgeons are obliged to prospectively register ventral hernia repairs in the Danish Ventral Hernia Database (14). The following data were retrieved from the database: date of index repair, age, hernia type, fascial defect size, open or laparoscopic approach, emergent or elective repair, and mesh or suture repair. Parity (nulliparous versus parous) prior to the index repair was retrieved from the DMBR. Matching was performed on all abovementioned variables. The women were followed from the index repair until date of reoperation for recurrence or date of questionnaire response. Hence, only one recurrence was considered for each included woman. Furthermore, only the first subsequent pregnancy was taken into account in the present study, as retrieved from the DMBR or the questionnaire.
The primary outcome of the study was hernia recurrence, defined as self-reported clinical recurrence or reoperation for recurrence. The secondary outcome was chronic pain, defined as moderate or severe pain from the site of the repair during the last week, as opposed to none or mild pain.
Statistics
Comparison of baseline characteristics was performed with Student’s t-test and Mann Whitney U for normally and non-normally distributed continuous variables, respectively. Categorical data were compared with χ2 or Fisher exact test, as appropriate. Matching was performed in a 1:3 ratio (subsequent pregnancy and no subsequent pregnancy) with a propensity-score based on a logistic regression model with a caliper width of 0.2 and the nearest neighbor method without replacement (15). The reverse Kaplan Meier estimator was used to calculate median follow-up (16). The risk of recurrence was analyzed with extended Cox regression analysis and graphically presented as cumulative incidence. The Cox model included previously identified risk factors for hernia recurrence which were reported with hazard ratios (HRs) and 95% confidence intervals (CIs). In the model, a subsequent pregnancy was included as a time-dependent variable to address the risk of immortal time bias, due to the inherent design mandating that women with a subsequent pregnancy must be recurrence-free during the interval from index repair to the pregnancy (17). Pregnancy conception was defined as the date preceding 267 days from the date of childbirth (18). The risk of chronic pain was analyzed with logistic regression analysis and reported as odds ratios (ORs) with 95% CI. A p-value < 0.05 was considered significant. Analyses were performed with R, version 3.5.2 (The R Foundation for Statistical Computing, Vienna, Austria). The study was approved by the regional Ethics Committee (H-17002135) and the Danish Data Protection Agency (BFH-2017-025).
Results
In total, 46 women underwent incisional hernia repair and subsequently gave birth during the inclusion period from 1 January 2007 to 31 December 2013. These women were matched with 138 women who had not given birth after the index repair. Eight women subsequently died or emigrated, and hence, a questionnaire was sent to 176 women (Fig. 1). In total, 124 (70.5%) women responded. There were no significant differences between responders and non-responders, apart from age (mean age responders 31.3 years versus non-responders 28.8 years, p = 0.005). Fifteen of the women in the control group reported a pregnancy after 1 January 2014 and were relocated to the pregnancy-exposed group. Thus, 47 and 77 women with and without a subsequent pregnancy, respectively, were included in the analyses. There were no significant differences between the two groups in comparison of baseline characteristics (Table 1). The median follow-up was 9.1 years (interquartile range 7.1–10.7 years). The median interval from the index repair to a subsequent pregnancy was 1.4 years (interquartile range 0.8–2.8 years).
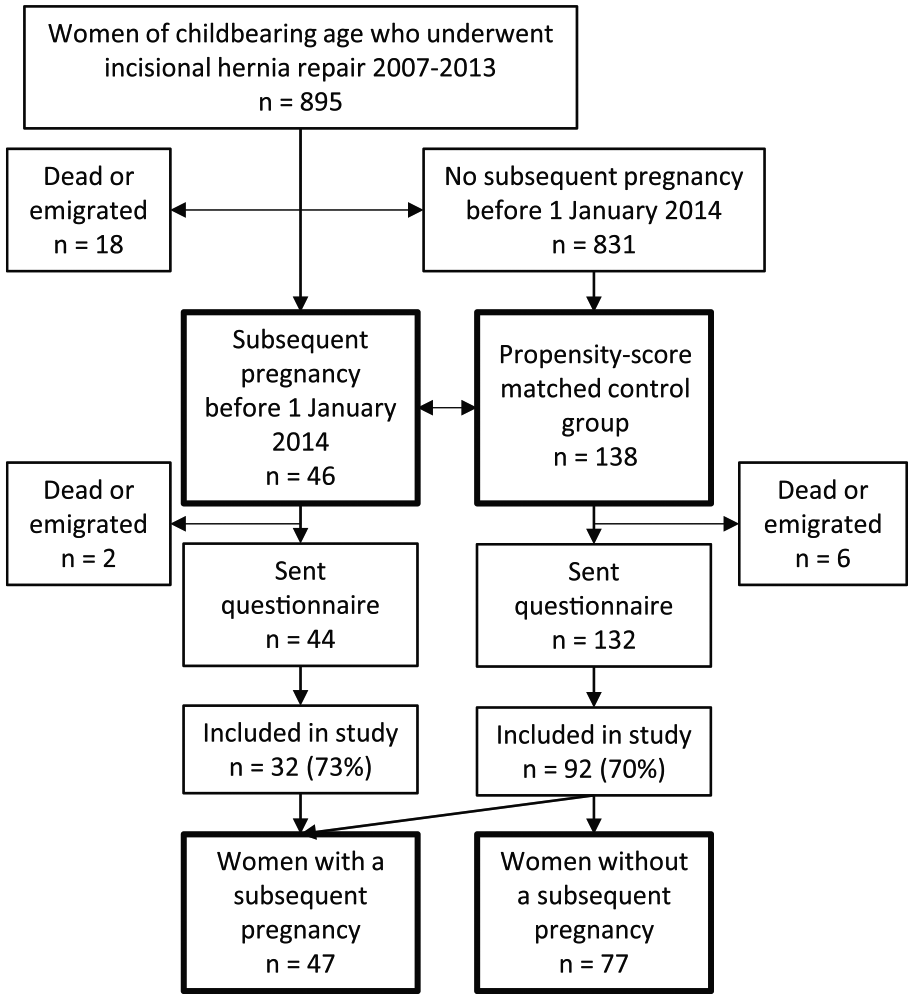
Study profile.
Baseline characteristics of women who underwent incisional hernia repair with and without a subsequent pregnancy.
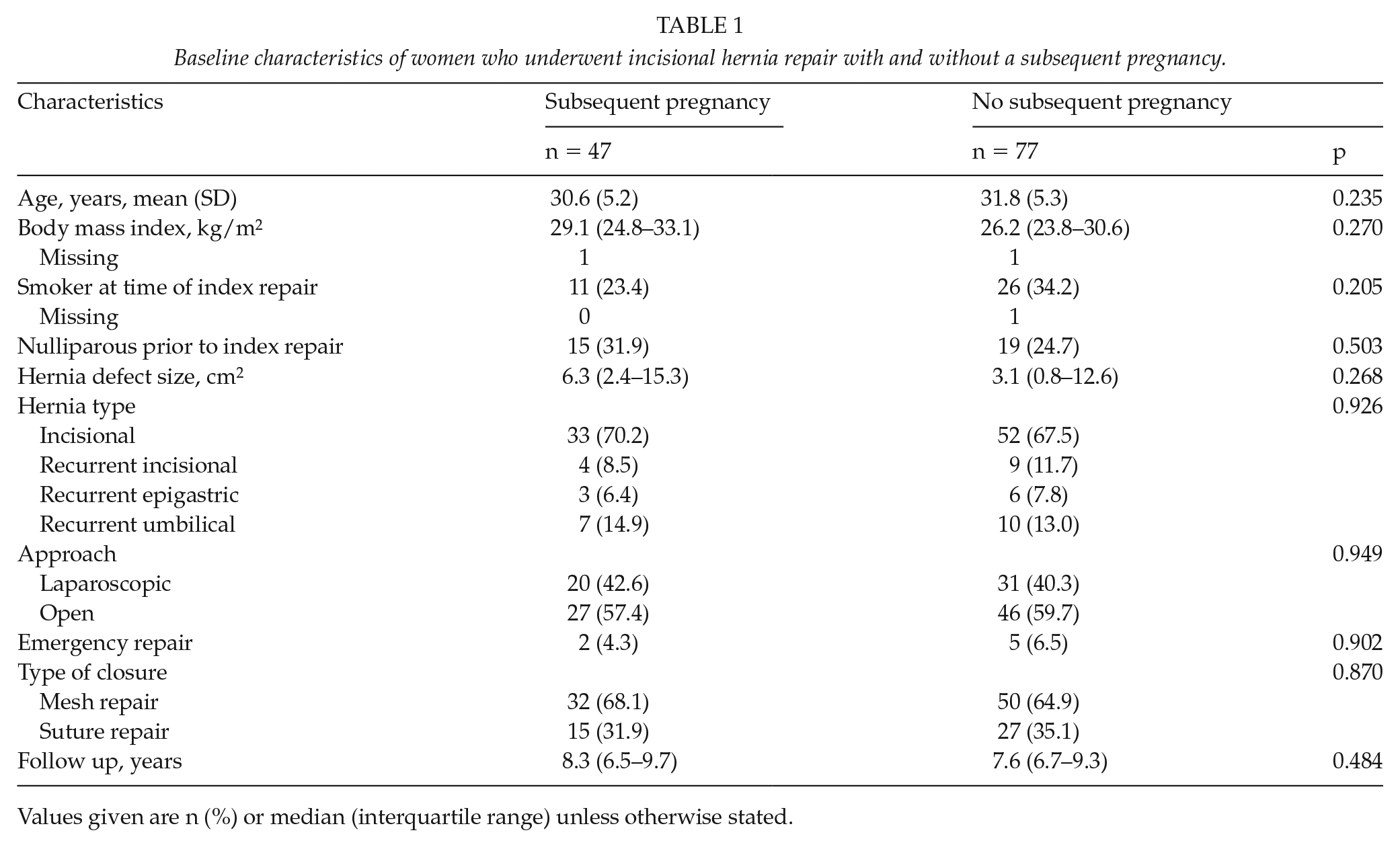
Values given are n (%) or median (interquartile range) unless otherwise stated.
Hernia recurrence
Fifty-two (41.9%) women reported hernia recurrence (clinical recurrence, n = 25 (20.2%), reoperation for recurrence, n = 27 (21.8%)). The 5-year cumulative incidence of recurrence was 41.0% (95% CI: 32.0%–49.9%). In the group of women with a subsequent pregnancy, the 5-year cumulative incidence of recurrence was 47.7% (95% CI: 31.8%–63.5%) from the time of pregnancy conception. In the group of women without a subsequent pregnancy, the 5-year cumulative incidence of recurrence from the time of index repair was 37.7% (95% CI: 26.9%–48.6%) (Fig. 2). In the extended Cox regression analysis, a subsequent pregnancy was significantly associated with recurrence, in both an unadjusted (HR: 1.87, 95% CI: 1.05–3.33, p = 0.033) and adjusted model (HR: 1.83, 95% CI: 1.02–3.29, p = 0.044) (Table 2). There were no other factors significantly associated with recurrence. A subsequent pregnancy remained associated with recurrence in a multivariable sensitivity analysis restricted to mesh repairs (n = 82) only (HR: 2.74, 95% CI: 1.30–5.75, p = 0.008). Increasing body mass index was also associated with recurrence, in this latter analysis (HR per 1 kg/m2 increase 1.05, 95% CI: 1.00–1.10, p = 0.042).
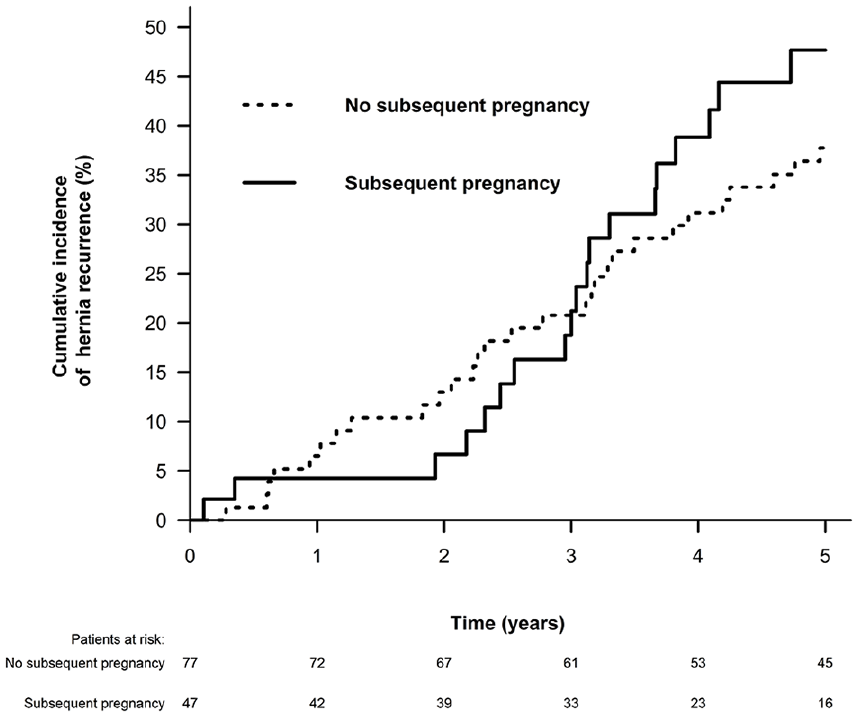
Cumulative incidence of hernia recurrence after incisional hernia repair in women of childbearing age. Time point 0 denotes day of index repair for women without a subsequent pregnancy. Time point 0 denotes day of estimated conception for women with a subsequent pregnancy, as these women were mandatory recurrence-free until this day. Please see “Methods” section for further details.
Multivariable extended Cox regression analysis for risk of recurrence (n = 52) after incisional hernia repair in women of childbearing age (n = 124).
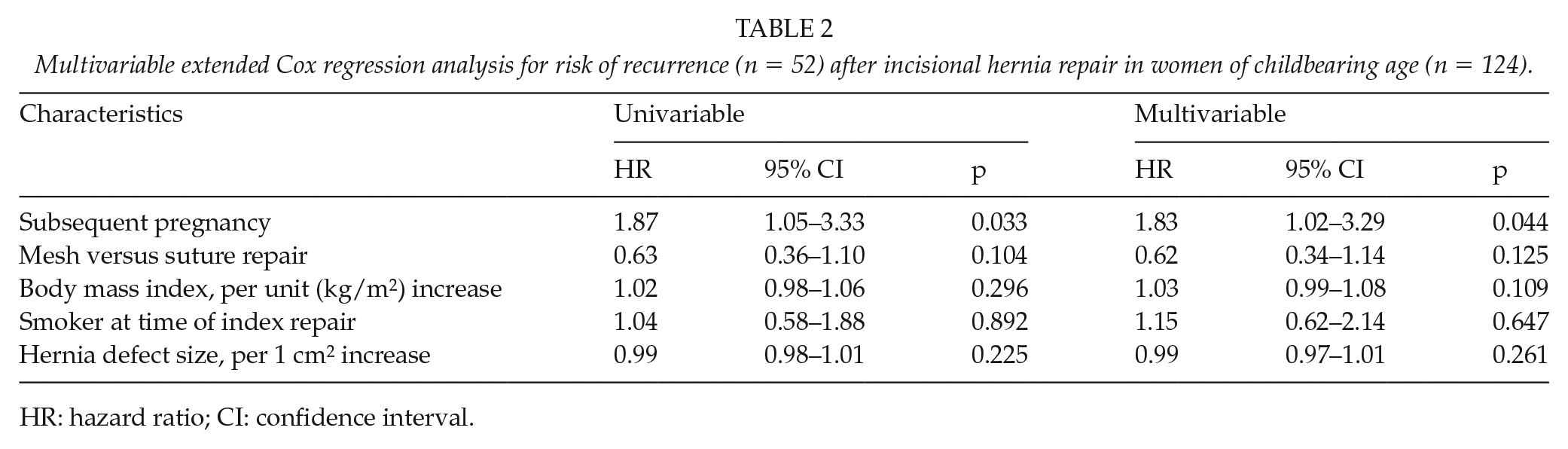
HR: hazard ratio; CI: confidence interval.
Chronic pain
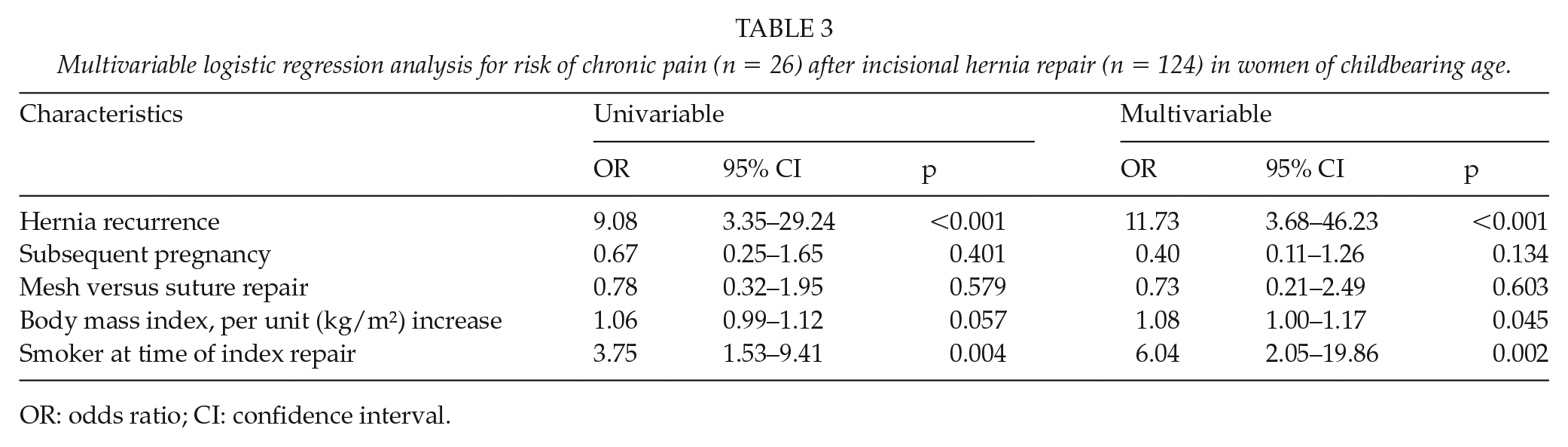
Twenty-six (21.0%) women reported chronic pain (moderate, n = 21; severe, n = 5); eight (17%) women in the group with a subsequent pregnancy, and 18 (23%) women in the group without a subsequent pregnancy. Hernia recurrence was associated with chronic pain, in a multivariable logistic regression analysis (OR: 11.73, 95% CI: 3.68–46.23, p < 0.001, Table 3). Furthermore, increasing body mass index and smoking were also independently associated with chronic pain. A subsequent pregnancy was not associated with chronic pain from the operated hernia site. A multivariable sensitivity analysis restricted to mesh repairs only (n = 82) revealed similar results (OR hernia recurrence 5.92, 95% CI: 1.79–22.63, p = 0.005).
Multivariable logistic regression analysis for risk of chronic pain (n = 26) after incisional hernia repair (n = 124) in women of childbearing age.
OR: odds ratio; CI: confidence interval.
Discussion
In this study, we found that a pregnancy following incisional hernia repair was associated with an increased risk of recurrence, whereas there was no difference in the risk of chronic pain comparing women with and without a subsequent pregnancy.
There is documented benefit of optimization of modifiable risk factors prior to ventral hernia repair (19). For primary ventral hernias, it is suggested that repair is postponed during the childbearing period to reduce the risk of recurrence (20, 21). However, the risk of delaying repair until after last pregnancy is not clear for incisional hernias (3). In the general adult population, it has been reported that watchful waiting for incisional hernias appears safe, while another study reported high crossover rates with increased morbidity and mortality compared with initial elective repair (22, 23). These studies did not consider and analyze the impact of a subsequent pregnancy. Hypothetically, incisional hernias may have a higher risk of enlarging and become increasingly symptomatic during a subsequent pregnancy compared with the typically smaller primary ventral hernias. Based on this study, considering potential pregnancies seems important in incisional hernia management. However, more studies are needed on the risks of watchful waiting versus surgical repair to define the optimal timing of hernia repair in women of childbearing age. In this study, the recurrence rate was also discouragingly high for women who did not have a subsequent pregnancy. Ideally, surgical repair should lead to complete restoration of the abdominal wall with a positive impact on quality of life (24). Recurrence and chronic pain have previously been associated with a decrease in both patient satisfaction and quality of life (4, 5).
High rates of recurrence and chronic pain were identified in the present study. A previous Danish study, which used an identical questionnaire, reported a 30% recurrence rate after incisional hernia repair in the general adult population (12). In that study, the reoperation for recurrence rate underestimated the total recurrence rate (reoperation for recurrence + clinical recurrence) fivefold, which is in contrast to the only twofold underestimation in the present study (52/27 = 1.9). It is hypothesized that surgeons are more willing to offer re-repair in case of recurrence in this subgroup. Younger age and female sex have previously been reported as associated risk factors for postoperative chronic pain (25), which could also partly explain the high rate in the present study. Furthermore, recurrence was a strongly associated predictor for chronic pain, as reported elsewhere (26). It has also been shown that preoperative pain is a predictor for postoperative pain (27), but unfortunately, a preoperative assessment was not available for the present study. There was no difference in the risk of chronic pain comparing mesh and suture repair. However, there are reports of aggravated pain during the course of the pregnancy following incisional hernia repair with mesh (28). Nonetheless, a mesh repair seems warranted to reduce the risk of recurrence, as for incisional hernia repair in the general adult population (24). In this study, a mesh repair was associated with a 38% decreased risk of recurrence (p = 0.125). The lack of statistical significance was likely due to a type II error due to the small study population. We had no data on pain during the pregnancies, but the findings of this study indicate that a subsequent pregnancy does not increase the risk of sustained chronic pain post partum. The study population size did not allow for subgroup analyses on operative details, such as mesh (type, placement, and fixation) and suture technique. The chronic pain questionnaire has not been validated.
Considering the association between hernia recurrence and pregnancy, this study confirms the findings from two previous registry-based cohort studies (6, 7). Both studies likely underestimated the recurrence rates, as recurrence was based on registration of hospital administrative data; thus missing recurrences managed elsewhere. Moreover, the study from Lappen et al. (6) was limited by a lack of data on hernia size and use of mesh. An additional limitation of the previous study from our group was the pooled data on both primary ventral and incisional hernias, which may have biased the results (29). However, it seems that the magnitude of the increased risk of recurrence imposed by pregnancy is similar for these hernia types (21).
This study has several limitations. There was a risk of selection bias due to the observational study design. We had no data on diabetes or wound complications, which have previously been associated with recurrence (30). There was a risk of recall bias, especially considering the chronological order of events for women who reported both a subsequent pregnancy and recurrence, and body mass index might have changed during follow-up. Finally, response bias might be present, although there were no differences in baseline characteristics between responders and non-responders. Strengths of the study included the long-term follow-up on a nationwide cohort, reflecting daily clinical practice. Furthermore, this is the first study to report patient-reported outcomes after incisional hernia repair in women of childbearing age (3).
In conclusion, poor outcomes following incisional hernia repair in women of childbearing age were found. A subsequent pregnancy was independently associated with an almost twofold increased risk of recurrence. However, a high risk of recurrence was also noted for women who did not become pregnant subsequently. A subsequent pregnancy did not seem to alter the risk of postoperative chronic pain.
Footnotes
Authors Contributions
Study conception and design was done by all authors. Acquisition and analysis of data was done by Oma. Interpretation of data was by all authors. Drafting of article was by Oma. Critical revision of article for important intellectual content was done by all authors.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Oma has received a grant from Lundbeckfonden. The foundation was not involved in study design, data collection, data analysis, article preparation, or publication decisions.