
Abstract
Introduction:
Inability to achieve social continence because of constipation or fecal incontinence affects up to 25% of patients with anorectal malformations (ARMs). 1 These patients require a scheduled bowel regimen, and independence in achieving fecal continence can be obtained with a Malone antegrade continence enema (MACE). 2 However, use of an MACE can be associated with complications, some of which require surgical intervention to correct. 3 We present the case of a 14-year-old boy who presented with MACE incontinence.
Methods/Case Presentation:
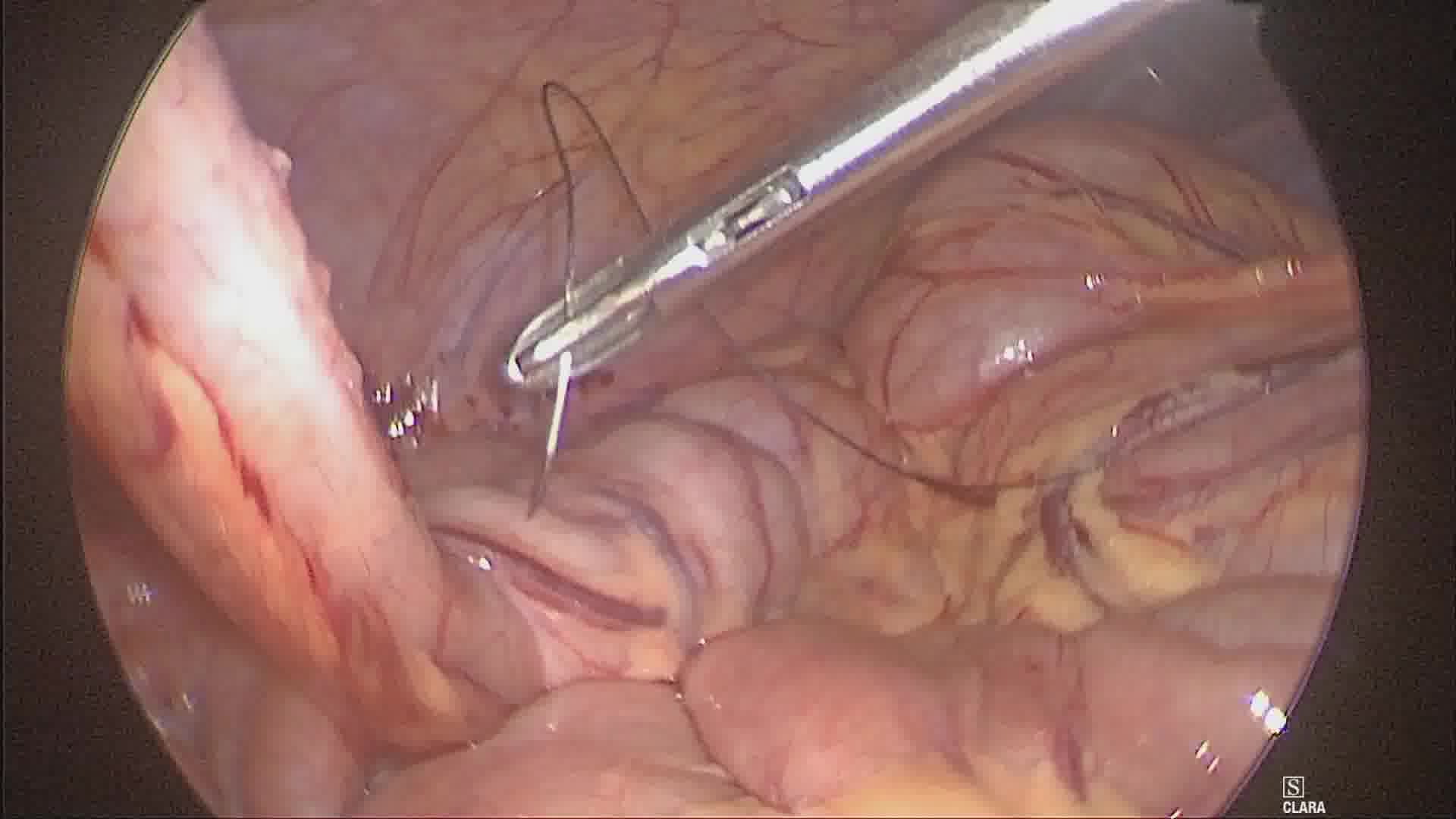
The authors have received and archived patient consent for video recording/publication. Our patient is a 14-year-old boy with a history of ARM, who previously had undergone posterior sagittal anorectoplasty with subsequent MACE placement at the age of 5 years to assist with fecal continence. The appendix was the conduit used; the channel was not plicated with a cecal wrap. Although the child denied any streaking or accidents with use of flushes, leakage of both saline and stool was noted from the MACE site. Work-up included anorectal examination under anesthesia, revealing a patent anus located within the sphincter muscle complex. A contrast study through the MACE revealed passage of contrast into the cecum but also reflux through the umbilicus. A 5-mm incision was made in the left upper quadrant as the MACE was situated in the umbilicus; 5 mm ports were then placed in the left lower and right upper quadrants. Mobilization of the cecum and terminal ileum was performed until the cecum could be wrapped around the base of the appendix without undue tension to create a valve mechanism. The 360° wrap was then created using 4-0 silk sutures, incorporating part of the cecum, the appendiceal wall, and then the cecum on the opposite side. After the first stitch was placed, a 10F Coude catheter was passed down the MACE and through the area of the wrap to ensure patency. Two further 4-0 silk sutures were placed in a similar manner. The patient was discharged on postoperative day 1 after tolerating a full flush. At 1-year follow-up, he is still able to perform his flushes without leakage from the channel and remains socially continent.
Results:
This patient benefitted from the creation of a laparoscopic fundoplication around the appendicostomy based on work-up and history. For primary MACE placement, we perform a fundoplication at the time of MACE placement. However, for children with persistent leakage of stool from the MACE channel, we perform investigations, like this case. 3 We have since performed 40 MACE procedures, all with formation of a fundoplication of the appendix/neoappendix at the time of operation. Two patients were referred for work-up and found to require laparoscopic cecal plications as the wrap was found to be disrupted or missing.
Conclusion:
Performance of a fundoplication around the MACE using proximal cecum is created to prevent reflux of flush and stool. For patients who present with leakage of stool from their MACE, such as in this case, a laparoscopic cecal plication can be created to prevent reflux.
Patient Consent Statement:
The authors have received and archived patient consent for video recording/publication in advance of video recording of the procedure.
The authors have no competing interests (either financially or personally) that could create a conflict of interest in connection with the video. The authors have no personal financial interests associated with the video; no funding was received for the creation of this video.
Runtime of video: 4 mins 47 secs
This video was presented as an oral presentation at the 2021 International Pediatric Endosurgery Group (IPEG) annual meeting in June 2021.


Keywords
Get full access to this article
View all access options for this article.