
Abstract
Background:
Laparoscopic hepaticojejunostomy for the treatment of choledochal cysts in children is one of the most technically challenging operative procedures. 1,2 Recent advances in high-definition imaging modalities have brought better intraperitoneal visibility, and have extended the indication to meticulous anastomosis for the small hepatic duct. 3 We herein describe secure laparoscopic hepaticojejunostomy of the small hepatic duct using simple duct plasty and two stay suture techniques. 4
Duct Plasty and Hepaticojejunostomy Using Two Stay Sutures:
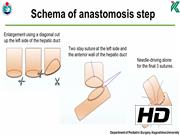
A 3-year-old boy was diagnosed with choledochal cyst caused by cholangitis. Pancreaticobiliary maljunction was found based on magnetic resonance image before the operation. Under general anesthesia, the patient was placed in a broad base position, and a 10-mm 30° laparoscope was inserted through an umbilical incision using the open 12-mm Hasson trocar method. Three additional trocars were inserted in the right upper abdomen (3-mm: operator's left hand), right side of the umbilicus (5-mm: operator's right hand), and the left lateral abdomen (3-mm: assistant's left hand) and a needle grasper (2.4-mm: assistant's right hand) was also inserted. After excision of the nondilated choledochal cyst and preparation of the jejunal limb and performing Roux-en-Y anastomosis outside the umbilicus, hepaticojejunostomy was performed. The small hepatic duct was enlarged using a diagonal cut up the left side of the hepatic duct (in the 3 o'clock direction). For the cutting device, we used fine scissors (Mini Endocut; Microline Surgical, Beverly, MA). At the start of hepaticojejunostomy, we usually place a stay suture at the left side of the hepatic duct (in the 3 o'clock direction). After placing a stay suture using 5-0 monofilament (PDS® Plus; Johnson & Johnson, New Brunswick, NJ), intracorporeal knot tying was performed on the left side of the hepatic duct, the long tail of the suture is suspended by the needle device (LAPA-HER-CLOSURE; Hakko, Co., Ltd., Tokyo, Japan) inserted in the left upper abdomen. To obtain stable observation and perform secure membrane-to-membrane anastomosis, the anterior wall of the hepatic duct was also suspended using 5-0 PDS from outside the body. After finishing posterior wall anastomosis, the anterior wall is sutured in the same manner by intracorporeal knot tying using 6-0 PDS. The suspending sutures are removed after anastomosis of half of the anterior wall is completed. Before finishing anastomosis of the anterior wall, needle-driving alone is performed for the final three sutures. Then, knot tying is performed to finish the hepaticojejunostomy. This technique helps avoid the risk of the involvement of posterior wall by needle-driving during anterior wall anastomosis because the lumen of the hepatic duct and mucosal layer of the anastomotic hole of the jejunum are confirmed. Anastomosis is completed without stent insertion.
Conclusion:
Duct plasty and confirmation of the lumen for anastomosis are important points associated with pitfalls in hepaticojejunostomy of the small hepatic duct. During anastomosis, the placement of two stay sutures, including a suspension technique for the anterior wall of the hepatic duct is useful for confirming the lumen of the hepatic duct. However, pediatric surgeons must endeavor to perform needle-driving precisely and to apply stable knot-tying techniques.
Acknowledgments:
We thank Brian Quinn for his comments and help with the article. This study was supported by Grants-in-Aid for Scientific Research from the Japan Society for the Promotion of Science (JSPS, Nos. 16K11350, 19K09150), research grant from JFE (The Japanese Foundation for Research and Promotion of Endoscopy), research grant from J-CASE (Japanese Consortium of Advanced Surgical Endoscopy), research grant from Kyushu Society of Endoscopic and Robotic Surgery, research grant of Karl Storz Award from Japan Society for Endoscopic Surgery, research grant from The Mother and Child Health Foundation and research grant from the Kawano Masanori Memorial Public Interest Incorporated Foundation for Promotion of Pediatrics.
No competing financial interests exist.
Runtime of video: 5 mins 54 secs


Get full access to this article
View all access options for this article.