
Abstract
Introduction:
Meckel's diverticulum, a congenital anomaly resulting from incomplete obliteration of the omphalomesenteric duct, is the most common gastrointestinal tract malformation (2%–4% incidence). 1 Although painless hematochezia is the most common presentation of a Meckel's diverticulum in younger children (<10 years of age), older children and adults rarely develop complications that include obstruction, intussusception, diverticulitis, hemorrhage, and neoplasm. According to one study, 2 risk factors for development of a symptomatic Meckel's diverticulum in adulthood include age <50 years (odds ratio [OR] 3.5, confidence interval [95% CI] 2.6–4.8), male gender (OR 1.8, 95% CI 1.3–2.4), diverticulum length <2 cm (OR 2.2, 95% CI 1.1–4.4), and histologically ectopic tissue (OR 13.9, 95% CI 9.9–19.6). 1 –9 Historically, open small bowel resection or diverticulectomy was the standard operative interventions utilized for Meckel's pathology. A growing body of literature suggests that minimally invasive (laparoscopic/robot-assisted laparoscopic) diverticulectomy or bowel resection for Meckel's diverticular disease is similarly safe and effective. This video describes the case of a 30-year-old man who presented with a 24-hour history of periumbilical abdominal pain that migrated to the right lower quadrant and was associated with fevers, nausea, and vomiting. He was found to have a leukocytosis and evidence of acute Meckel's diverticulitis on CT imaging.
Methods:
The patient was taken to the operating room and underwent diagnostic laparoscopy, incidental appendectomy, and laparoscopic small bowel resection with intracorporeal anastomosis. The common channel of the small bowel anastomosis was stapled, and the enterotomy was closed in two layers with running Vicryl and interrupted silk sutures. The mesenteric defect was closed with running barbed absorbable suture. Total operative time was 135 minutes.
Results:
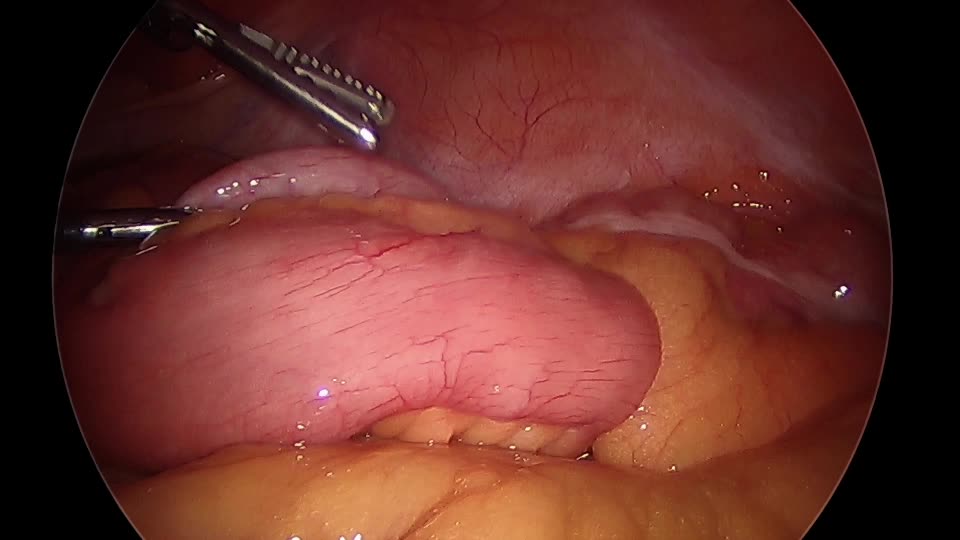
Meckel's diverticulum measured 7 cm in length and 3.5–4 cm in width. Pathology report revealed a histologically normal appendix and evidence of Meckel's diverticulitis without evidence of ectopic tissue or neoplasia. Our patient had an uneventful postoperative course and was discharged home on postoperative day 3. He was doing well at his hospital follow-up visit; he was completely asymptomatic and had returned to work 1 week after surgery.
Conclusions:
This case demonstrates an uncommon case of Meckel's diverticulitis in an adult patient who underwent effective laparoscopic segmental small bowel resection. Our result along with recent literature suggests that minimally invasive surgery is a viable option for the treatment of Meckel's diverticulitis when necessary.
No competing financial interests exist.
Runtime of video: 9 mins 58 secs


Get full access to this article
View all access options for this article.