
Abstract
Background:
Traditional management of an acute sigmoid volvulus (SV) includes adequate resuscitation and colonoscopic decompression to detorse the volvulized colon. Owing to the high recurrence rate, an elective sigmoid resection is recommended. A laparoscopic sigmoidectomy is a well-accepted option secondary to decreased pain, faster recovery, and lower morbidity rates.1–4 Recently, natural orifice specimen extraction (NOSE) has been adopted to maximize the benefits of laparoscopic surgery.5 This video details a laparoscopic procedure and the steps of transrectal specimen extraction to demonstrate the utility of NOSE for patients with SV.
Methods:
An SV was diagnosed in a 45-year-old woman. She was treated nonoperatively and an elective sigmoid colectomy with NOSE was performed. In brief, the patient was placed in the Trendelenburg position under general anesthesia, and four trocars were placed after creating a pneumoperitoneum. The sigmoid colon with its mesocolon was mobilized in a medial to lateral direction using a tissue-sealing device (ENSEAL, Ethicon Endo-Surgery; Johnson & Johnson). The elongated sigmoid colon was then completely divided and the resected colon was subsequently extracted through the rectum and delivered transanally through a rectoscope (TEO, Karl Storz, Tuttlingen, Germany). Finally, the anastomosis was made with a circular stapling device (CDH 29; Ethicon Endo-Surgery, Cincinnati, OH). No drain was placed in the pelvis, and the 10- to 12-mm ports were closed with a Vicryl suture meticulously to reduce the risk of port site herniation.
Results:
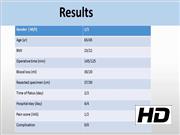
Two patients with recurrent SV were treated by this technique. The average length of the resected colon was 33.5 cm. The mean operative time was 130 minutes and mean blood loss was 25 mL. During the postoperative period no analgesic agents were given and the hospital stay was 4 days. Both patients passed flatus and were started on a liquid diet on day 2. There were no postoperative complications and they remained well at 2 years follow-up without recurrent SV.
Conclusions:
Clinical data and our experience suggest that either transvaginal or transanal NOSE does not prolong operative times for laparoscopic colorectal surgery.6 To avoid potential intraperitoneal contamination, a regular preoperative bowel preparation is strongly recommended. An elective laparoscopic NOSE colectomy for SV is feasible and safe in terms of a fast recovery, minimal postoperative pain, and a low risk of wound comorbidities. In properly selected cases, this technique can be considered as an alternative for both benign and malignant colorectal diseases. Because of the limited diameter of the rectoscope, this approach may not be appropriate for patients with a high BMI, a bulky mesocolon, or large tumors.
No competing financial interests exist.
Runtime of video: 6 mins 59 secs


Get full access to this article
View all access options for this article.