
Abstract
Objective
To evaluate the feasibility, safety, and short-term outcomes of middle rectal resection followed by transanal specimen extraction.
Methods
Forty-four patients with small mid-rectal tumors underwent laparoscopic rectal resection followed by transanal specimen extraction.
Results
The procedure was successful in all patients without intraoperative conversion or additional access. The mean operation time was 182.7 minutes (range, 130–255 minutes), the mean blood loss was 26.5 mL (range, 5–120 mL), the mean postoperative exhaust time was 31.3 hours (range, 16–60 hours), and the mean length of hospital stay was 9.5 days (range, 8–19 days). One patient developed anastomotic leakage, which was treated by intravenous antibiotics and daily pelvic cavity flushes through the abdominal drainage tube. No infection-related complications or anal incontinence were observed. The mean tumor size was 2.1 cm (range, 1.6–3.2 cm), the mean number of harvested lymph nodes was 16.5 (range, 6–31), and the mean follow-up time was 8.5 months (range, 2–16 months). By the last follow-up, no signs of recurrence had been found in any patient.
Conclusion
The combination of standard laparoscopic proctectomy and transanal specimen extraction could become a well-established strategy for selected patients.
Keywords
Introduction
Laparoscopic surgery has been widely practiced for benign and malignant colorectal diseases since laparoscopic-assisted colorectal surgery was first performed in 1991. Accumulated evidence suggests that laparoscopic-assisted surgery for colorectal cancer has gradually become an acceptable alternative to open surgery in terms of faster postoperative recovery and long-term outcomes.1–4 However, this technique typically requires an abdominal incision to extract the specimen, resulting in postoperative pain and other abdominal wound-related complications. In one study, the incidence rates of incisional hernia in patients undergoing laparoscopic versus open colorectal cancer surgery were 12.3% versus 13.8%, respectively. 5 In addition, because the length of the abdominal incision is directly related to the incisional hernia rate, avoiding laparotomy might influence the rate of postoperative wound complications. 6
The development of natural orifice transluminal endoscopic surgery (NOTES) has provided the notable advantages of completely avoiding surgical wounds and wound-related postoperative complications. 7 However, many challenging technical problems of NOTES remain to be solved, such as the need for complex surgical procedures, selection of proper operative approaches, lack of suitable instruments and devices, unclear exposure to the surgical field, and closure of the natural orifice incision.
The combination of a laparoscopic technique and specimen extraction through a natural orifice (i.e., laparoscopic natural orifice specimen extraction (laparoscopic NOSE)) preserves the advantages of both laparoscopic surgery and NOTES.8–11 In addition, laparoscopic NOSE represents a considerable technical advancement over open surgery, laparoscopic surgery, and NOTES while avoiding an abdominal specimen extraction wound and wound-related complications.
Currently, laparoscopic NOSE is mainly applied for colonic resection. Selected low-risk patients with rectal carcinoma can undergo transanal rectal resection followed by transanal specimen extraction when performed by an experienced colorectal team.12,13 However, very few studies related to rectal resection are available. Wolthuis et al. 14 reported the technical possibilities and shortcomings of laparoscopic NOSE–colectomy, describing the various techniques to further minimize trauma and exploring new surgical strategies in bridging conventional laparoscopic surgery (CLAPS) with pure NOTES.
The present retrospective study focused on the novel procedure of laparoscopic total mesorectal excision (TME) for mid-rectal cancer with transanal specimen extraction. We also herein discuss the feasibility, safety, technical aspects, and short-term outcomes of this minimally invasive surgical technique.
Materials and methods
Patient selection
This study involved 44 consecutive patients who underwent treatment of rectal tumors from September 2015 to March 2019. The inclusion criteria for this technical procedure were as follows. (1) The primary tumor was located at the middle rectum, histopathologic examination confirmed rectal cancer, and the distance between the lower edge of the tumor and the dentate line was 5 to 10 cm. (2) The depth of tumor invasion was clinically within T3. (3) Preoperative imaging examination (computed tomography and magnetic resonance imaging) suggested that the circumferential diameter of the tumor was ≤3 cm. (4) The body mass index (BMI) was ≤30 kg/m2. (5) Informed consent was obtained from the patients. The exclusion criteria were advanced T3 tumors and performance of preoperative radiotherapy or chemotherapy.
The exhaust time was defined as the time to first passage of flatus or first bowel movement following surgery. Postoperative pain was measured using a visual analogue scale, which graded the pain intensity from 0 (no pain) to 10 (maximal pain ever experienced). Because this was a retrospective study, the requirement for ethics review was waived. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). All surgeries were conducted by the same team of surgeons (Xishan Wang, MD, PhD). Written informed consent was obtained from the patients for publication of this study. The reporting of this study conforms to the STROBE guidelines. 15
Preoperative preparation and anesthesia
All patients were given preoperative oral laxatives for bowel preparation the evening before the surgery, and an enema was given 3 hours before the surgery. During anesthetic induction, a single dose of a second-generation cephalosporin or levofloxacin was routinely given by intravenous infusion. The same dose was repeated if the operative time exceeded 3 hours. All patients were given general anesthesia.
Operative technique
Once anesthetized, the patients were placed supine in the modified lithotomy position for better anal access. A five-trocar laparoscopic approach was applied during the procedure. A 10-mm supraumbilical trocar was inserted for the laparoscopic camera. Another 12-mm trocar was inserted through the right lower quadrant for the surgeon’s operation. Three additional 5-mm ports were placed in the left lower quadrant, right middle abdomen, and left middle abdomen, respectively.
The medial-to-lateral approach was applied to mobilize the distal part of the descending colon and the sigmoid colon. The left gonadal vessels, left ureter, and inferior mesenteric nerve plexus were identified and preserved during this procedure. The inferior mesenteric artery was dissected and transected at the point of origin from the aorta following the application of Hem-o-Lok clips (Teleflex Inc., Wayne, PA, USA). Regional lymph node dissection was performed at the root of the inferior mesenteric vessels. The right and left lateral attachments of the sigmoid colon were incised cephalically toward the distal part of the descending colon and caudally toward the colorectal junction. The splenic flexure was selectively released to ensure adequate length for a tension-free anastomosis. The mesorectum was circumferentially dissected caudally as far as 3 to 5 cm below the lower margin of the rectal tumor. The whole procedure of rectal resection strictly complied with the TME technique. The rectum was irrigated with 1% povidone-iodine solution (Betadine; Avrio Health, Stamford, CT, USA). An assistant surgeon gently distended the anal orifice until four fingers could be accommodated, and 2 L of diluted 1% povidone-iodine solution was then used to irrigate the sigmoid colon and rectum.
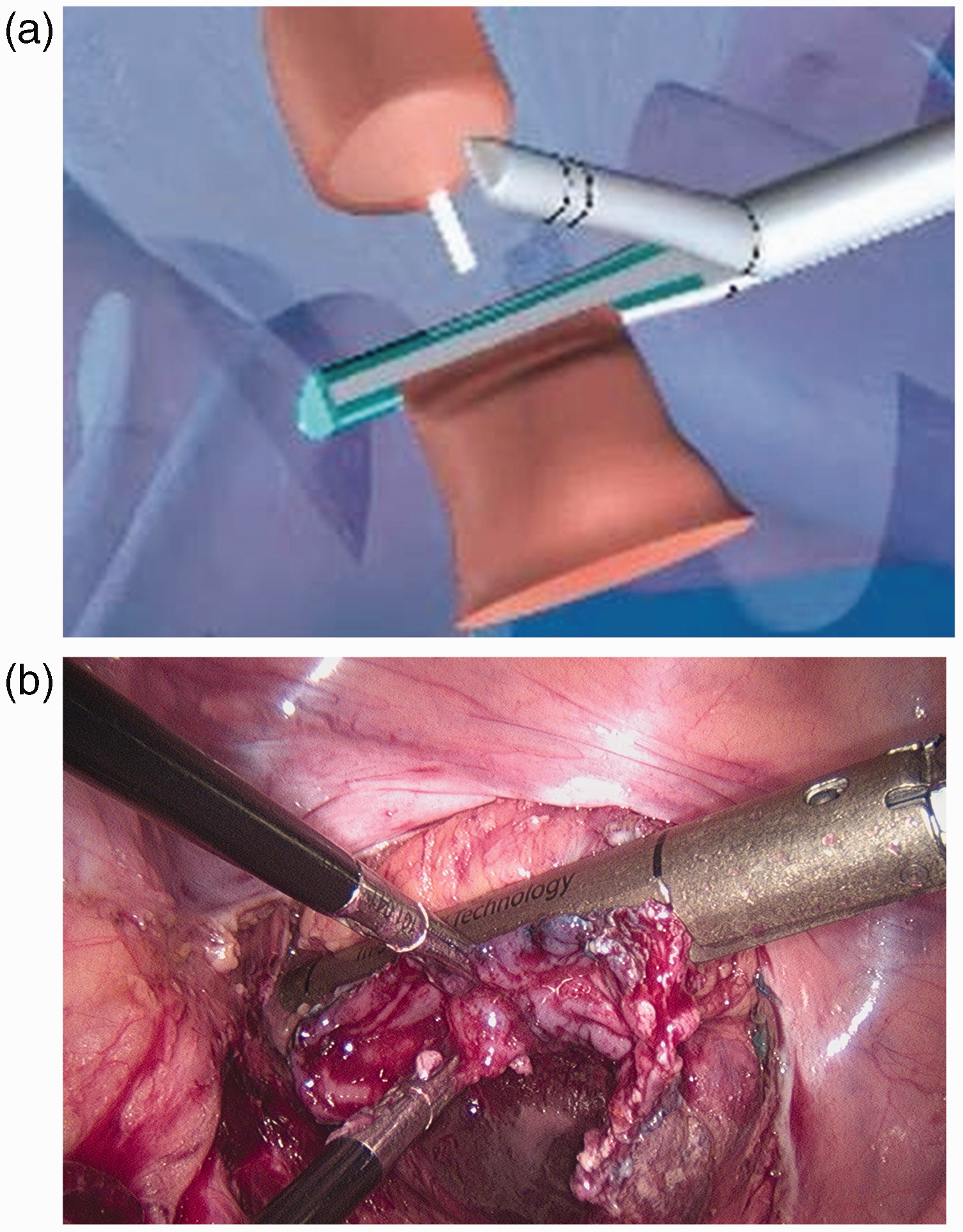
A linear stapler (Echelon 60; Ethicon Endo-Surgery, Cincinnati, OH, USA) was used to transect and close the rectum as far as 2 to 3 cm below the lower edge of the tumor. After perineal re-disinfection, the distal rectum was thoroughly irrigated with a diluted povidone-iodine solution. Next, the stump of the distal rectum was incised under laparoscopic vision after reassessing the feasibility of transanal specimen extraction. A sterile protective sleeve was transanally inserted into the abdominal cavity through the opened distal rectal stump for smooth extraction of the specimen and to avoid tumor deposition at the opened rectal stump. The previously resected proximal rectum was then grasped by sponge forceps gently inserted through the sterile protective sleeve and gradually exteriorized until the tumor site segment was available for extracorporeal transection (Figure 1). The rectal specimen was extracorporeally resected at the colorectal junction. The specimen was carefully inspected to ensure an adequate distal margin. The anvil of the circular end-to-end anastomosis stapler (CDH29; Ethicon Endo-Surgery) was then inserted through the opened proximal sigmoid colon stump, and a purse-string suture was simultaneously applied using 2-0 Prolene (Figure 2). The proximal colon stump was gently returned to the pelvis through the anus.
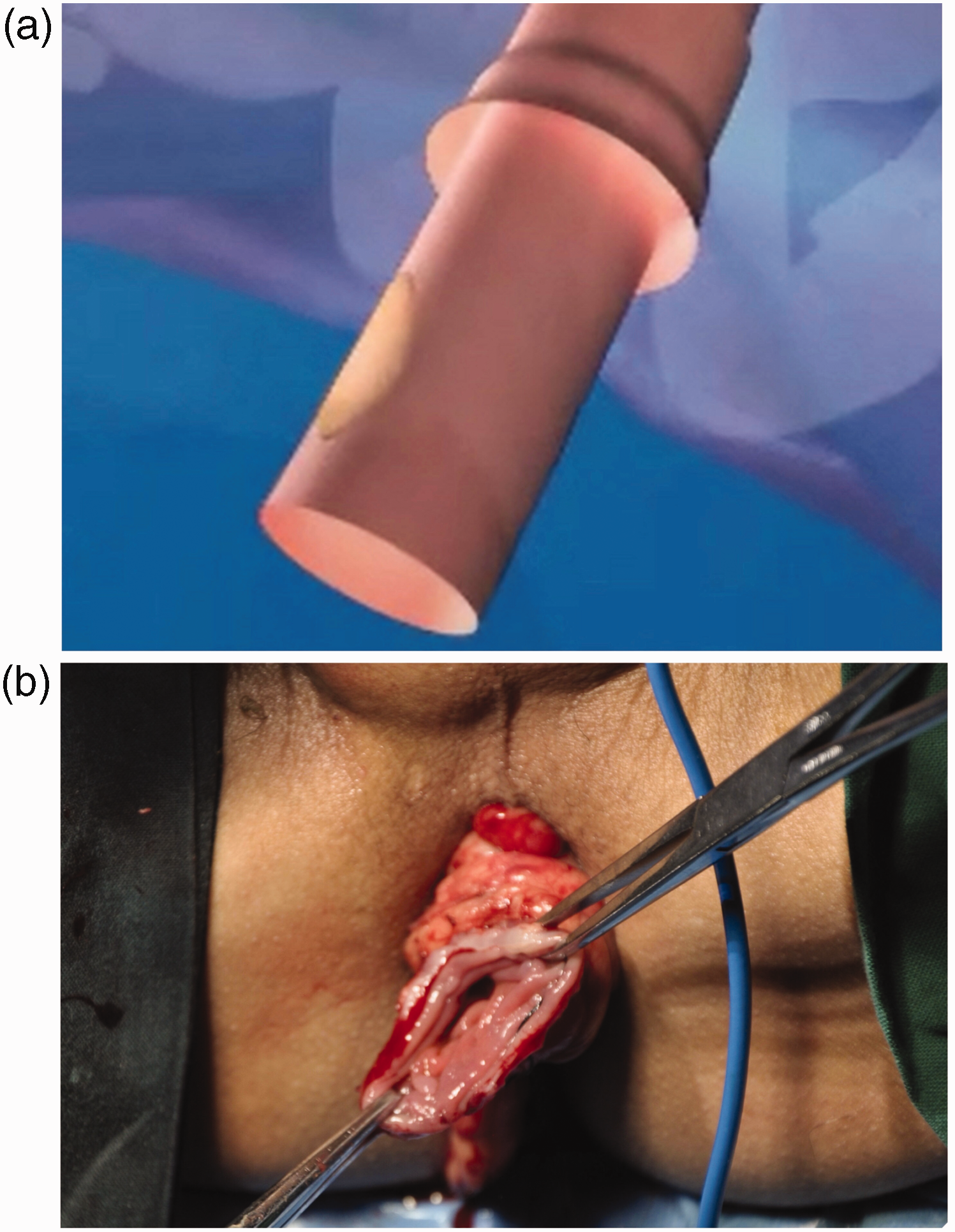
The specimen is pulled out through the anus. (a) Schematic presentation and (b) Intraoperative photograph.

The anvil is inserted into the opened proximal sigmoid colon stump. (a) Schematic presentation and (b) Intraoperative photograph.
The open rectal stump was transabdominally closed with a linear stapler (Endo-GIA AST45; Medtronic, Minneapolis, MN, USA) (Figure 3), and the resected cuff was placed in a specimen retrieval bag and then extracted through the 12-mm trocar. The head of the circular stapler was passed through the anal orifice. Next, the anvil and the central rod of the stapler were connected, the stapler was fired, and an end-to-end double-stapled anastomosis was performed intracorporeally with laparoscopic guidance (Figure 4). The doughnuts were scrutinized, and a routine air leak test was performed. Finally, a soft peritoneal drainage tube was placed following pelvic wash-out to the anastomosis through a 5-mm trocar site in the right lower quadrant.
The open rectal stump is closed. (a) Schematic presentation and (b) Intraoperative photograph.

An end-to-end stapled anastomosis is performed. (a) Schematic presentation and (b) Intraoperative photograph.
Results
Forty-four consecutive patients with rectal tumors were documented from September 2015 to March 2019. All patients underwent laparoscopic TME for mid-rectal cancer followed by transanal specimen extraction at the Second Affiliated Hospital of Harbin Medical University, Harbin, China (Table 1).
Patients’ characteristics and short-term outcomes.
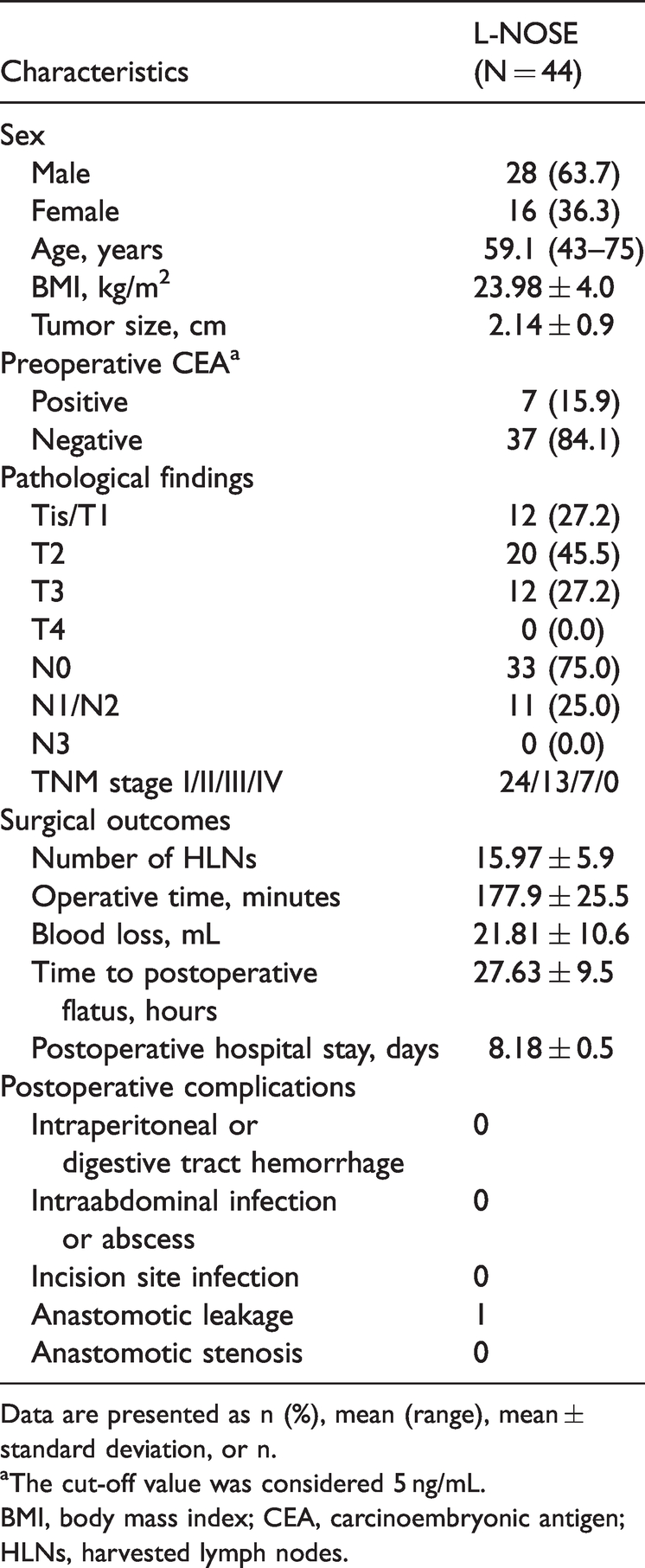
Data are presented as n (%), mean (range), mean ± standard deviation, or n.
aThe cut-off value was considered 5 ng/mL.
BMI, body mass index; CEA, carcinoembryonic antigen; HLNs, harvested lymph nodes.
The procedure was successfully performed in all 44 patients in this retrospective study. In general, all patients underwent laparoscopic TME and regional lymphadenectomy followed by transanal specimen extraction. None of the patients required conversion to open surgery, and there were no intraoperative complications or other abdominal-related complications, including postoperative complications. One patient underwent simultaneous hysteromyomectomy, and the specimen was also extracted transanally. No rectal or anal injuries were observed during and after the specimen extraction.
Of the 44 patients, 28 were male and 16 were female. The patients’ mean age was 59.1 years (range, 41–75 years). Their mean BMI was 23.9 kg/m2 (range, 17.4–30 kg/m2), mean operative time was 177.9 minutes (range, 130–255 minutes), mean blood loss was 21.8 mL (range, 5–120 mL), mean postoperative exhaust time was 27.6 hours (range, 10–60 hours), and mean length of hospital stay was 8.1 days (range, 5–19 days). On the fifth postoperative day, one patient was diagnosed with anastomotic leakage as confirmed by fecal spillage from the drainage tube. We performed a computed tomography scan to assess the severity of the leakage; however, we did not consider performing an ileostomy. Based on the International Multispecialty Anastomotic Leak Global Improvement Exchange (IMAGInE) definition of anastomotic leakage, the case was recognized as low-severity leakage (Grade A) 16 and was managed with an antibiotic course and daily pelvic cavity flush through the abdominal drainage tube. The patient was discharged on postoperative day 19. No patient required a blood transfusion. None had a positive result on the air leak test after anastomosis. The patients’ characteristics and short-term outcomes are summarized in Table 1.
The mean tumor size was 2.1 cm (range, 1.5–3.2 cm). Twenty of the patients (45.4%) had a stage T2 tumor, 12 (27.2%) had a stage T3 tumor, and 12 were diagnosed with a stage T1 tumor or adenoma both preoperatively and postoperatively. In the 12 patients with stage T3 tumors, tumor resection was considered challenging by transanal endoscopic microsurgery because these tumors were more extensive. The mean number of harvested lymph nodes was 15.9 (range, 6–25). The mean postoperative pain score was 2.2 (range, 1.0–5.5). The mean follow-up time was 8.5 months (range, 2–19 months). All specimens (100%) were R0, defined as no tumor tissue within 1 mm of the resection margins, which proves the safety of this technique. All patients were disease-free until the last follow-up.
Discussion
The natural orifices for specimen extraction mainly include the vagina and the anus for laparoscopic colorectal resection.17–19 The vagina has better ductility, making it available for more extensive indications and larger primary tumors. By contrast, the anus is more reasonable for minimizing extra injuries and is suitable for both men and women. By combining five-port laparoscopic proctectomy and specimen extraction through the anal orifice, our surgical technique compensates for the shortcomings of NOTES and improves surgical feasibility. Furthermore, less invasive surgery reduces discomfort and fatigue and shortens the hospital stay. Moreover, our technique results in only five small port scars on the patient’s abdomen (Figure 5 and Supplementary Video 1).

Patient’s abdominal wall 3 weeks after surgery.
We used a sterile protective sleeve to smooth the rectal wall and reduce excessive pressure during specimen delivery, thereby limiting injury to the rectal wall and anal sphincter. In addition, this sleeve prevents extraction site dispersion or recurrence by preventing contact between the distal rectal stump and the removed specimen. Similar devices, such as a polyurethane wound retractor (Alexis; Applied Medical, Rancho Santa Margarita, CA, USA) and a modified proctoscope (40 mm in diameter, 22 cm in length; Novymed International BV, Gorinchem, Netherlands), have been used in other clinical studies.8,9 Postoperative abdominal or pelvic infection due to intestinal bacterial spread from the bowel opening during the surgery and specimen extraction is still a serious concern of laparoscopic proctectomy. However, no postoperative infection was observed in this study. Therefore, intracorporeal bowel opening might not increase the probability of pelvic contamination after laparoscopic proctectomy. 20 These results also reflect the importance of preoperative bowel preparation, intraoperative rectal irrigation with diluted 1% povidone-iodine solution prior to resection, and postoperative application of antibiotics.
The two main indications for this surgical technique are as follows. First, the depth of invasion of stage T2 and T3 tumors is appropriate, and such tumors accounted for 72.6% of all patients in this study. Stage T1 rectal tumors and benign adenomas, considered challenging to resect by transanal surgery because of their large size, were also selected for this approach. Preoperative rectal intraluminal ultrasound and pelvic magnetic resonance imaging were necessary examinations to judge the T stage. Second, the maximal circumferential tumor diameter should be <3 cm. It is difficult to extract the specimen through the anus in patients with local advanced tumors and patients with a higher BMI; the large tumor or bulky mesentery may lead to injuries to the anal sphincter, tearing of the specimen tissue, or even breaking of the tumor when pulling the specimen out. This scenario may explain the occurrence of postoperative anastomotic leakage in the patient whose circumferential tumor diameter was >3 cm in the present study.
Breakthroughs in technology have expedited the development of minimally invasive surgical treatments such as CLAPS and NOSE surgery (NOSES). 11 Laparoscopic removal of colorectal specimens is safer and more successful than removal by open surgery.21–25 CLAPS results in superior postoperative healing. 26 Nonetheless, CLAPS specimens require a small laparotomy. Significant incision-related complications include postoperative discomfort, incisional infection, an abdominal wall scar, and incisional hernia formation.27–30
Transanal TME (TaTME) (another hybrid NOTES technique) is helpful for dissection of the very distal rectum and mesorectum and provides an excellent anatomical view of the deep pelvis. Challenging cases (e.g., obese men with large distal tumors) benefit from the transanal approach. In addition, TaTME can improve the prognosis of patients with middle and low rectal cancer and overcome the limitations of dissection of the angulated rectum deep in the pelvis.31,32 Despite these encouraging results, TaTME still has some particular complications. For example, Rouanet et al. 33 reported a urethral injury rate of 6.6%. Moreover, the quality of existing data concerning anorectal, urinary, and sexual function and quality of life after TaTME is still low,33–39 showing that TaTME has a longer learning curve and needs further research.40,41
NOSES is a popular colorectal cancer treatment. It is a substitute for laparoscopic and open surgery. NOSES without small incisions reduces postoperative morbidity and improves recovery. In recent years, NOSES has been largely embraced by colorectal surgeons and patients.14,42,43 In addition, laparoscopic NOSE has been shown to be successful, eliminating the need for an additional incision.44–46 Compared with CLAPS, the main characteristics of NOSES in colorectal surgery are complete intraperitoneal anastomosis and extraction of specimens from the natural orifice.9,43,47 Recently published studies have compared the short-term results between NOSES and CLAPS, providing convincing evidence for the clinical practice of colorectal oncology. 48 The NOSES group had lower complications, better postoperative results, lower pain scores, less analgesic demand, and faster recovery. In addition, the NOSES group had a slightly improved time to first flatus and time to return to a regular diet. Moreover, the total morbidity rate in the NOSES group was significantly lower than that in the CLAPS group. Anastomotic leakage and bleeding were not statistically significant postoperative concerns even though transanal specimen retrieval necessitates laparoscopic expertise and may prolong surgery. 49 There are numerous potential reasons for delay. One is that intraperitoneal anastomosis is a lengthy process. 27 Another is that the surgeon’s learning curve and laparoscopic expertise are essential. After a series of experiments, the NOSES operating time was gradually reduced.46,50 One study showed no statistically significant difference between the operation times of NOSES and CLAPS; thus, a similar operative duration may be attributable to surgeons’ greater knowledge of NOSES and advances in laparoscopic techniques and equipment.51–53
Another study showed that the NOSES and CLAPS groups were comparable in lymph node retrieval. 49 In addition, postoperative pain in the NOSES group was significantly reduced, presumably because NOSES does not require an additional incision for specimen extraction, resulting in faster ambulation, recovery, and discharge. 54 Pain reduction reduced the demand for analgesics. Al-Ghazal et al. 55 found that aesthetic surgery impacts psychosocial morbidity. Follow-up studies showed no local recurrence.27,51,56 Postoperative complications measure the safety of emerging procedures. NOSES has lower postoperative morbidity than CLAPS. This is due to fewer incision-related problems, such as incision infection, mainly because natural orifice points are used to avoid a large incision in NOSES. NOSES has the same risks of peritoneal bacterial contamination and tumor seeding as CLAPS.27,57–59 The reduced operational trauma afforded by NOSES may be indispensable for aged people with increasing comorbidities and diminished physiological buffer and functional reserve. 60
In our recent study, we recommended measures against contamination- or seeding-related complications when retrieving specimens in routine clinical practice, including bowel preparation, prophylactic antibiotic use, peritoneal lavage, and sterile protection devices. 42 Postoperative anal incontinence and dyspareunia are common complications associated with the anal and vaginal extraction routes. However, the occurrence of these two problems is reportedly low, and symptoms are mild and reversible.27,61 Moreover, postoperative outcomes are greatly affected by the surgeon’s expertise, 62 equipment used, and surgical indications. 42 The International Consensus on NOSES for Colorectal Cancer published by our department has demonstrated the aesthetic advantages of NOSES over laparoscopic procedures. Patients who undergo NOSES experience higher satisfaction because of scarless recovery. Whether colorectal aesthetics affects psychological outcomes and prognosis is a worthy area of research. 42 The NOSES technique has some inherent limitations, however. The indications for NOSES should follow the indications for laparoscopic colorectal resection. The surgeon, patient’s sex, and tumor size limit the use of this technique. Experienced laparoscopic colorectal surgeons should perform NOSES. Transanal NOSES is suited for male and female patients with tumors of <3 cm. However, transvaginal NOSES is only applied to female patients, and the tumor diameter is limited to 5 cm. 42 Hence, the tumor size in NOSES should be strictly restricted. Moreover, a comparison of malignant and benign diseases revealed that individuals with malignant diseases had much longer mean hospital stays than those with benign diseases, whereas the mean length of hospital stay for patients with benign conditions was shorter. Therefore, shorter hospitalization periods for NOSES may be associated with benign illnesses.59,63
Notably, these results must be interpreted with caution because of the limited number of studies reporting 3-year and 5-year survival rates. Additionally, NOSES was performed in patients with smaller tumors than in patients who underwent CLAPS. Additional research is required to investigate the potential changes in the patient’s prognosis caused by the surgical procedure of tumor features. Hence, treatment must be individualized for patients and surgeons to improve the benefit-to-risk ratio.
In addition, most published studies to date have reported short-term results. The long-term results, such as cancer recurrence and disease-free survival, need to be verified by more longitudinal studies. Furthermore, most studies to date were retrospective studies with small samples (<50 patients), reducing their inherent quality.
This study has some limitations. First, only short-term outcomes were reported. As noted above, long-term outcomes such as cancer recurrence and disease-free survival will require more longitudinal studies for validation. Second, the poor delineation of certain variables (such as incision-related complications) and the varied methods of assessing and recording the different outcomes (such as cosmesis and time to flatus) may limit the generalizability of the results to specific situations. Additionally, this was a retrospective study with a small sample size (<50 patients), which decreases its inherent quality. Finally, the inclusion of a control group is required to compare the feasibility, safety, and short-term outcomes of laparoscopic NOSE with other standard proctectomy techniques. Because these data are not currently available from our institution, we conducted a mini-review to compare laparoscopic NOSE with other surgical techniques (CLAPS and open surgery for colorectal resection) to prove the superiority of laparoscopic NOSE.
Although the safety and feasibility have been well demonstrated, these limitations must be considered before NOSES is implemented in colorectal surgery. However, high-quality evidence is still needed to demonstrate its short-and long-term efficacy to obtain reasonable and robust evidence that supports the performance of NOSES.
Conclusion
The herein described laparoscopic proctectomy and transanal specimen extraction technique is undoubtedly a well-established strategy for good intraoperative and postoperative outcomes. Moreover, the results of this study are consistent with other preliminary clinical reports.8,9,64 No evidence of metastasis or recurrence was found in any of the patients included in this study during the short-term follow-up. Although the feasibility and benefits of NOSE have been demonstrated in the literature, patient selection plays a significant role in taking full advantage of this evolution in minimally invasive surgery. The benefits of NOSE require further study, particularly to determine whether the reported benefits can be generalized to larger populations. We also expect a prospective evaluation in a controlled randomized study to further assess the long-term outcomes between this procedure and standard laparoscopic rectal resection.
Research Data
Research Data for Laparoscopic natural orifice specimen extraction, a minimally invasive surgical technique for mid-rectal cancers: Retrospective single-center analysis and single-surgeon experience of selected patients
Research Data for Laparoscopic natural orifice specimen extraction, a minimally invasive surgical technique for mid-rectal cancers: Retrospective single-center analysis and single-surgeon experience of selected patients by Shan Muhammad, YiBo Gao, Xu Guan, Tang QingChao, Shao Fei, Guiyu Wang, Yinggang Chen, Zheng Liu, Zheng Jiang, Kavanjit Kaur, Kamchedalova Tatiana, Qurat Ul Ain, Xishan Wang, Jie He in Journal of International Medical Research
Footnotes
Authors’ contributions
Declaration of conflicting interests
All authors have completed the ICMJE uniform disclosure form. The authors have no conflicts of interest to declare.
Funding
The authors disclosed receipt (pending publication) of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Key R&D Program of China (2020YFC2006400, 2020AAA0109500), the National Natural Science Foundation of China (82122053 to YG, 82188102 to JH), the CAMS Initiative for Innovative Medicine (2021-I2M-1-067 to YG), the Non-profit Central Research Institute Fund of Chinese Academy of Medical Sciences (2021-RC310-020 to YG), and the Key-Area Research and Development Program of Guangdong Province (2021B0101420005 to YG).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.