
Abstract
Introduction:
Postoperative urinary incontinence is a side effect that can dissuade prostate cancer patients from proceeding with robot-assisted radical prostatectomy (RARP). Numerous technical modifications and refinements have been proposed to enhance early recovery of continence. However, incontinence rates still range between 14% and 40% at 3 months after RARP. 1,2 This imposes a significant burden on both the patient and the health care system. To improve adequate preoperative patient consultation, various patient characteristics have been assessed to predict a delay in postoperative urinary continence recovery, such as older age (≥68), 3 higher BMI (>30 kg/m2), 4 surgeon’s technical skills, 5 and short membranous urethral length (MUL) (<1.2 cm). 6 As a short MUL has been observed to be associated with a significant delay in continence recovery, precise dissection of the prostatic apex and extended preservation of the urethral stump have been studied and proven effective in enhancing continence recovery. 7,8 Here we describe our modified apex dissection during RARP and present our outcomes.
Methods:
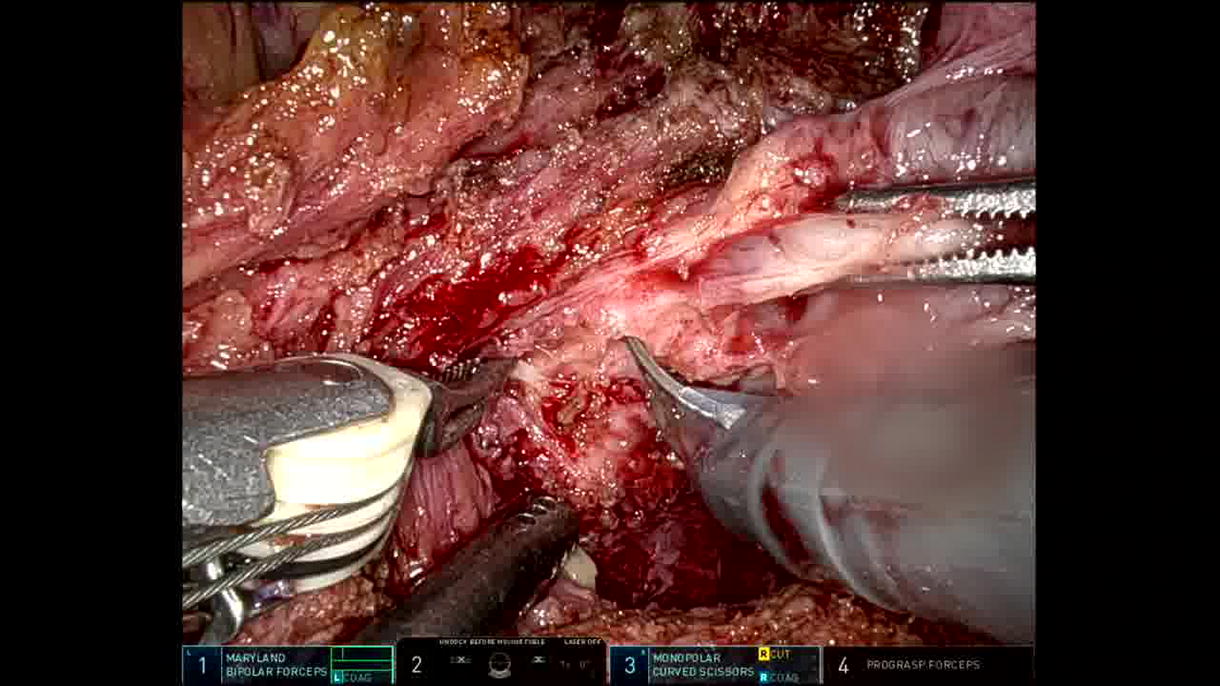
A total of 175 patients underwent RARP with the Hood technique between March 2022 and July 2023. Bladder neck sparing was applied in all cases. Preoperative MUL measurement was available from 115 (66%) patients. Short MUL was defined as <1.2 cm measured on T2-weighted MRI. Extended preservation of the urethra by 360-degree dissection of the prostatic apex before urethral transection, as demonstrated in the video, was applied to all patients. Postoperative urinary continence rates at 3 months were compared between patients who had short (n = 19) and normal (≥1.2 cm) MUL (n = 96). Daily use of 0–1 security pad was defined as continence. The two-tailed Fisher’s exact test was used to compare continence rates between the two groups.
Results:
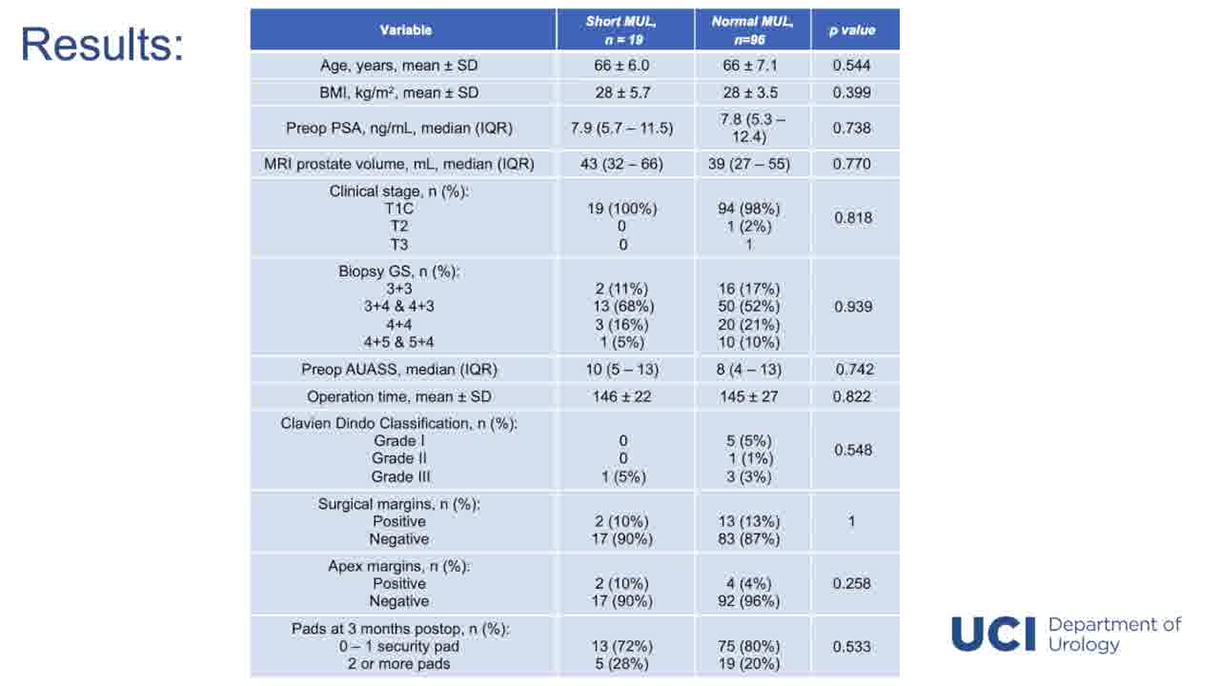
Baseline patient and tumor characteristics such as mean (±SD) age (66 ± 6.0 vs. 66 ± 7.1 years; p = 0.544), mean BMI (±SD) (28 ± 5.7 vs. 28 ± 3.5 kg/m2; p = 0.399), and median (IQR) prostate volume measured on T2-weighted MRI (43 [32–66] vs. 39 [27–55] mL; p = 0.770) were comparable between the group with short MUL and normal MUL, respectively. In both groups, most of the patients were diagnosed with T1C-stage prostate cancer (100% vs. 98%, p = 818). Postoperatively, no differences were observed in surgical margins (p = 1), apex margins (p = 0.258), and complication rates (p = 0.548). At 3 months, there was no difference between continence rates of patients with short preoperative MUL (n = 13, 72%) and patients with MUL ≥1.2 cm (n = 75, 80%, p = 0.533).
Conclusion:
Precise dissection of the prostatic apex aimed at preserving extended urethral length mitigates the impact of short MUL on continence recovery after RARP.
Author Disclosure Statement:
We have no financial disclosure or conflicts of interest with the material presented in this presentation.
Patient Consent Statement:
Author(s) have received and archived patient consent for video recording/publication in advance of the video recording of the procedure.
Runtime of video: 5 mins 48 secs.
Get full access to this article
View all access options for this article.