
Abstract
Introduction:
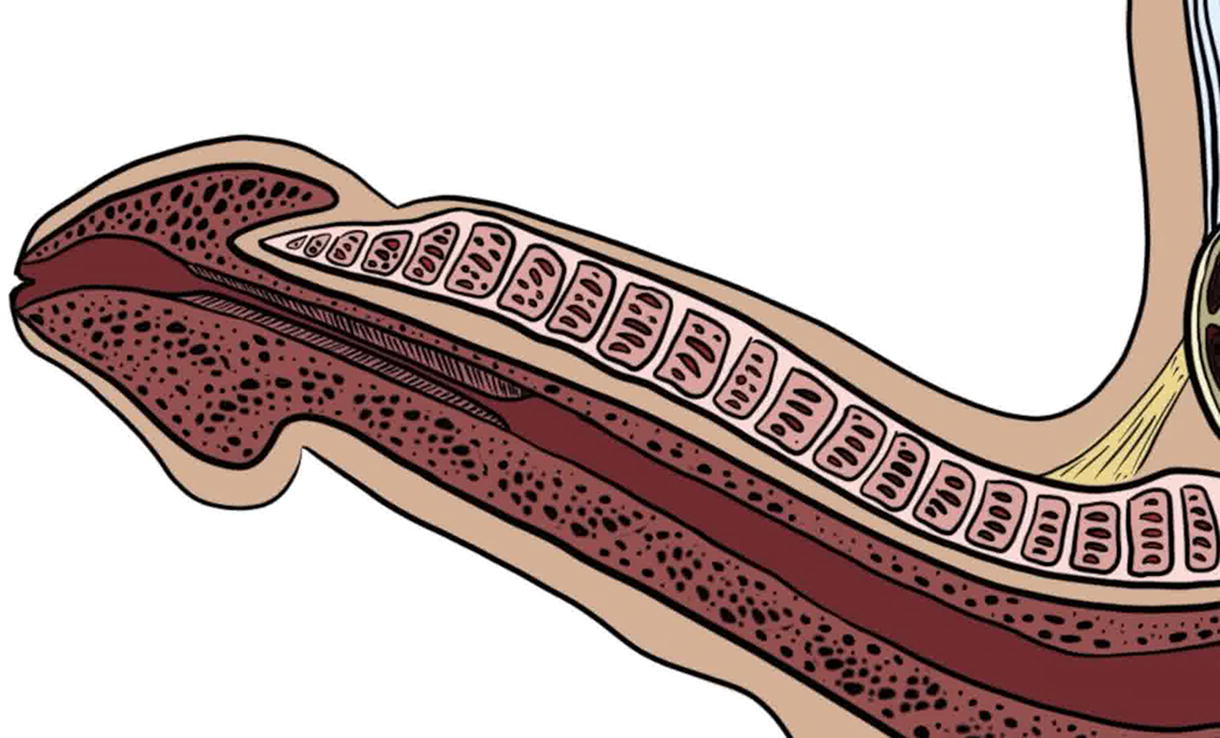
Endoscopic urethroplasty combines the minimally invasive benefit of endoscopic dilation or urethrotomy with the durability of open urethroplasty. Novel techniques in endoscopic urethroplasty have appeared through the years since the 1970s, including several techniques to hold free grafts against urethrotomy beds, such as grafts glued or sutured to a catheter, double-balloon catheter, and a novel balloon-graft carrying device along with transperineal sutures. 1 –7 Ungerer et al. describe their endoscopic buccal graft urethroplasty using laparoscopic suturing instruments and a procedure-specific transurethral sheath. 8 In this video, we present our technique and early outcomes for transmeatal urethral surgery (TraMUS) for distal penile strictures. This technique applies to any stricture of the penile urethra where the distal aspect of a buccal mucosa graft (BMG) can be accessed transmeatally.
Materials and Methods:
The patient is prepped in the supine position. A 6 o’clock incision is made sharply using a nasal speculum with a scalpel, and an endoscopic cold knife set along the ventral plate of the urethra from the proximal end of the stricture to the meatus. Goal caliber is 26 French. The urethrotomy length is measured.
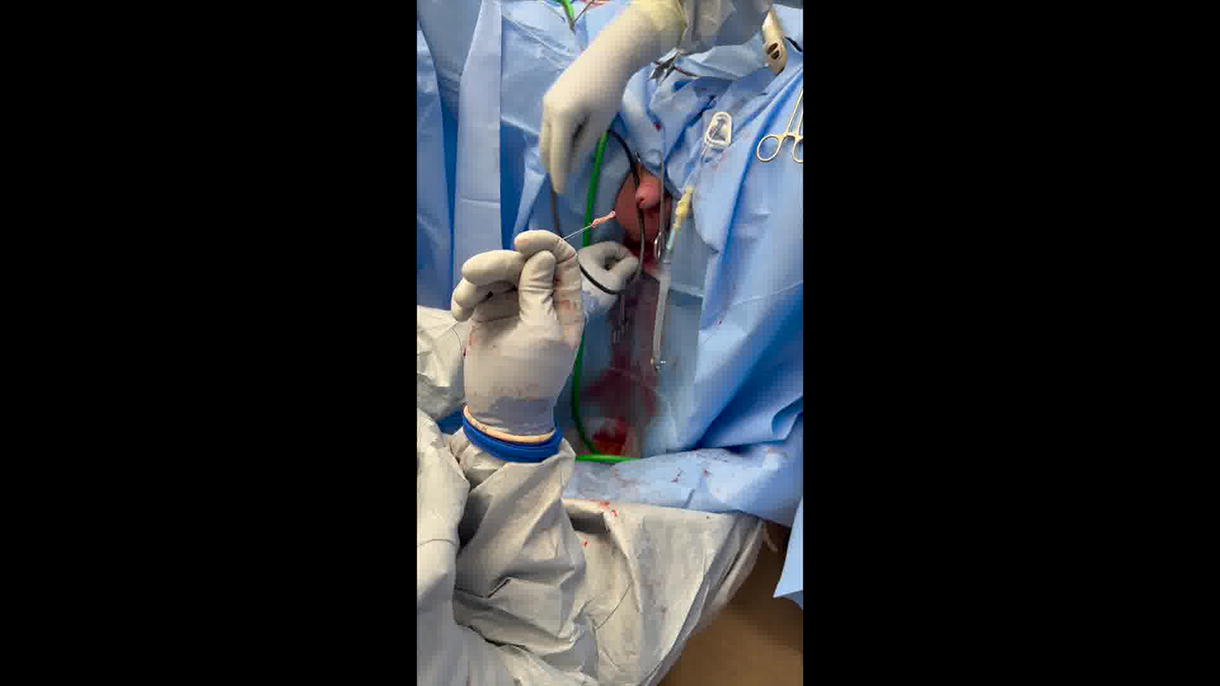
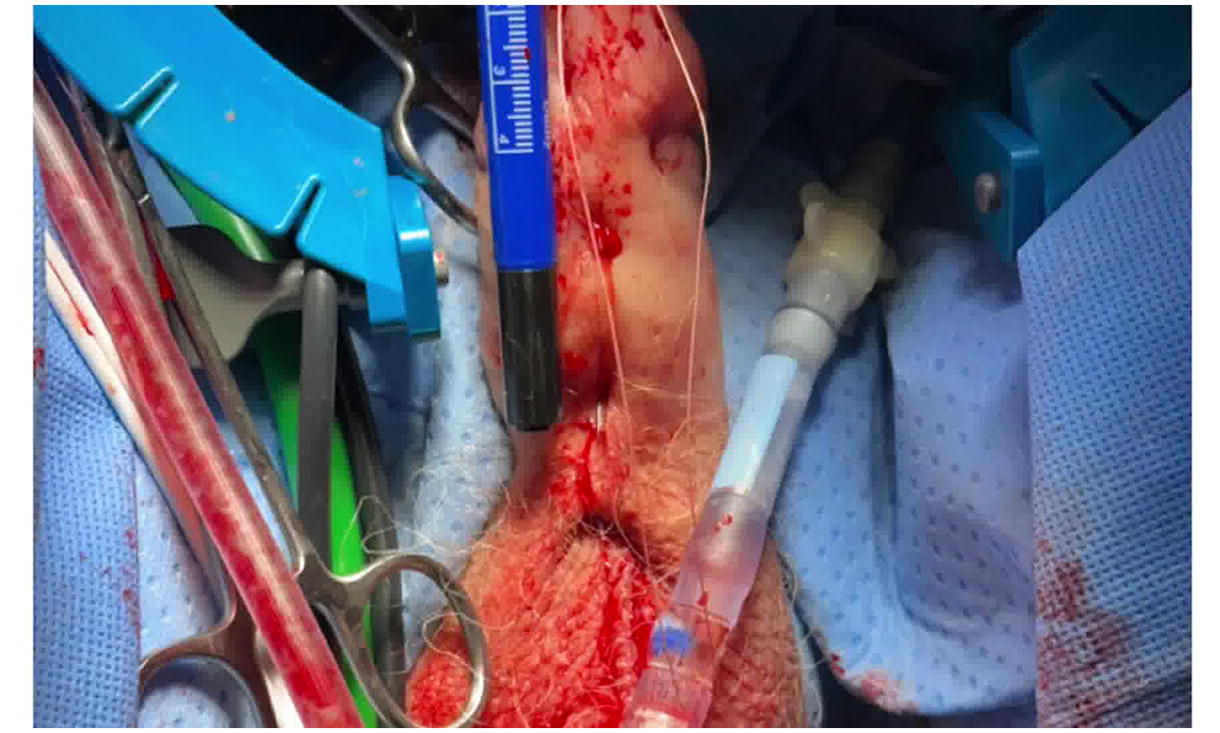
A split-thickness BMG is deployed by passing a 26 French offset scope into the urethra. A Laborie needle is passed through the scope, through the mucosal edge of the urethrotomy, and out the penile skin. With each puncture, a 3-0 PDS free suture is passed through the needle, and the needle is removed to externalize the suture through the meatus. This is repeated until one pair of sutures exists on either side of the proximal urethrotomy. The equipment is removed and the transmeatal ends of each pair of sutures are passed through the proximal end of the graft from anti-mucosa to mucosa using a free needle and tied. The transcutaneous suture ends are pulled to parachute the graft into the urethra over the urethrotomy and then tied externally at the skin. The distal end of the graft is secured to the meatus with interrupted 4-0 Vicryl. Quilting sutures are placed along the graft using 3-0 Vicryl on skiied SH needles, similarly passing the needles through the urethra and out the skin with ends tied together, and then tying externally at the skin. Alternatively, quilting may be performed via the Laborie needle for more proximal placement.
A Foley catheter is placed, and a compressive dressing is applied to the penis. The catheter remains for 2 weeks. Cystoscopy is performed at 4 months and 1 year to ensure patency.
Results:
Nineteen patients have been treated using TraMUS for distal penile strictures. Eighteen patients had at least 4 month of follow-up, with an average follow-up of 8 months (range 4–21 months). 2 failures are documented, in which we were unable to pass the 17 Fr flexible cystoscope. Median graft length was 5 cm (range 3–15 cm, IQR 4.9).
Conclusions:
TraMUS for distal penile strictures is a promising new technique for minimally invasive urethral reconstruction. The technique appears to be effective, and further data about outcomes are still needed.
Patient Consent:
Author(s) have received and archived patient consent for video recording/publication in advance of video recording of the procedure.
Conflicts of Interest:
The authors have no disclosures.
Runtime of video: 8 mins 13 secs.
Get full access to this article
View all access options for this article.