
Abstract
Introduction and Objectives:
Urethral stricture disease is a challenging urologic problem with a high recurrence rate. Initial management is typically completed endoscopically (e.g., urethral dilation, direct visual internal urethrotomy); however, guidelines recommend against repeated endoscopic management. Currently, surgical urethroplasty or intermittent catheterization remains the only other option. We have demonstrated a minimally invasive approach to urethroplasty. In this video, we aim to demonstrate the techniques and early outcomes of transmeatal urethral surgery for short urethral strictures.
Materials and Methods:
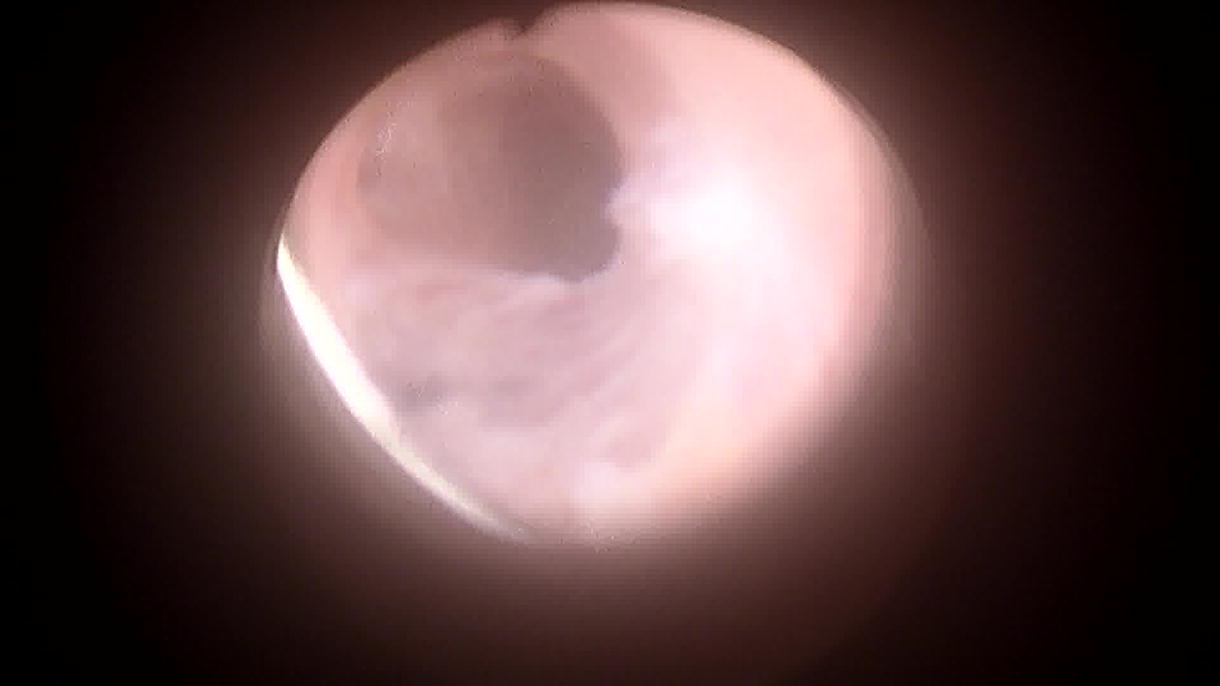
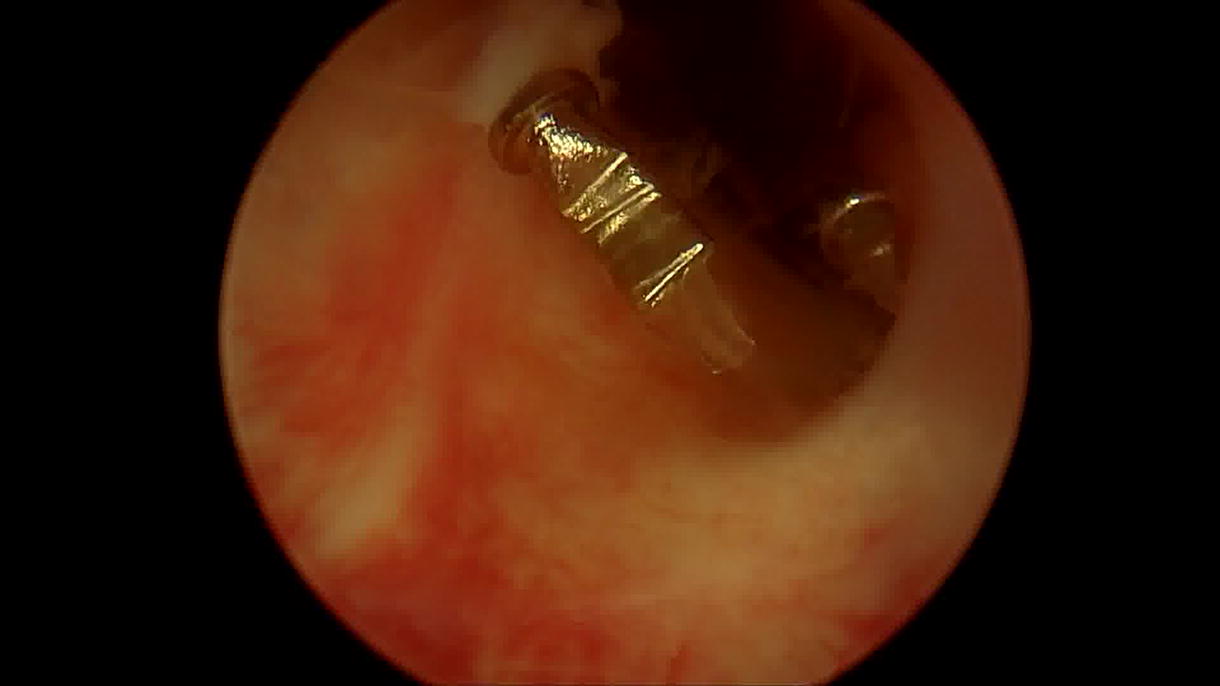
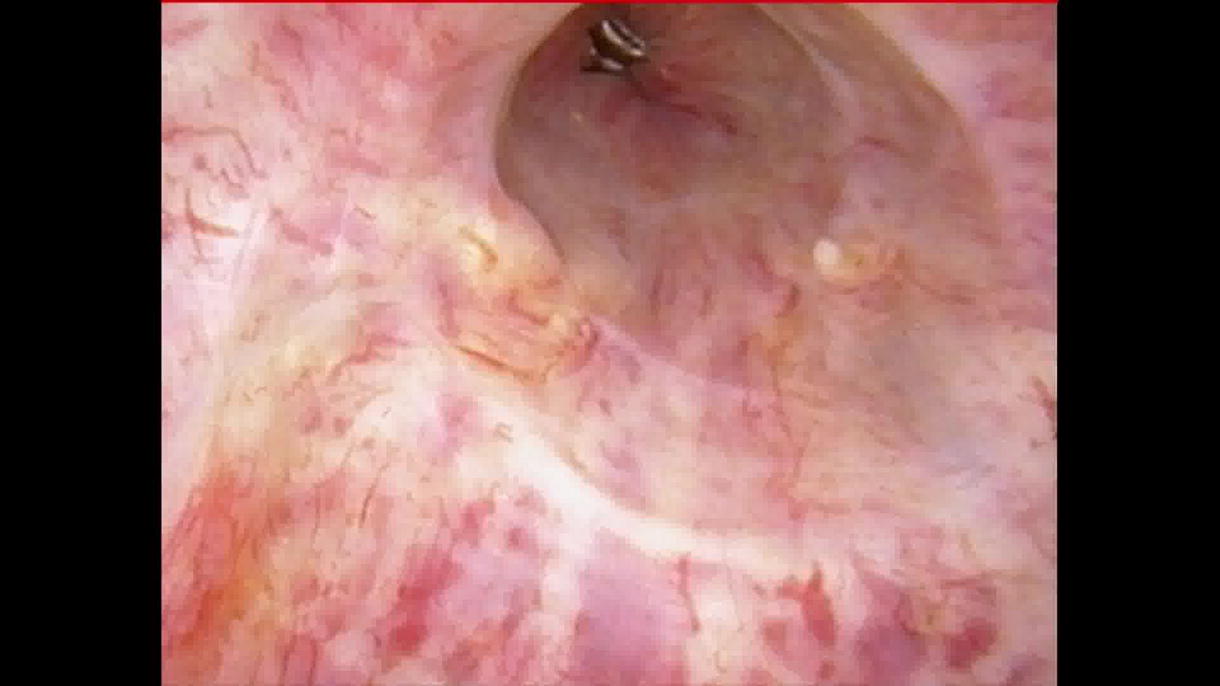
We demonstrate the procedure in two different individuals with idiopathic bulbar urethral strictures less than 2 cm. The patient is prepped in dorsal lithotomy position. Under direct visualization via cystoscopy, the ventral place of the urethral stricture is first incised to a goal of 26 Fr lumen. Next, mucosal realignment is completed via LSI Solutions’ URTRAC sheath and the RD 180 endoscopic suturing device. Two sutures are placed on either side of the urethrotomy incision site, allowing the proximal and distal ends of the mucosa to be pulled perpendicular to the urethrotomy. After reapproximation, a titanium knot is introduced endoscopically to anchor each suture into place. An indwelling catheter is then left in place. Patients are then seen at four months postoperatively.
Results:
Out of four total patients, there is a 100% success rate cystoscopically at 4 months postoperatively. There have been no recorded intraoperative or postoperative complications. The average operating room time was 54 minutes, and the average estimated blood loss was 9 mL.
Conclusions:
Transmeatal urethral surgery for short strictures via incision and urethral reapproximation appears to be a safe and effective repair option for the management of short urethral strictures.
All research procedures were carried out in accordance with ethical guidelines and institutional policies, reviewed by the IRB. Authors have received and archived patient consent for video recording/publication in advance of video recording of procedure.
The authors declare that there are no commercial associations or financial interests in any product or service discussed in this article that might create a conflict of interest. The authors have not engaged in any activities or relationships with commercial entities that would bias or influence the content of this study.
Runtime of video: 5 mins 40 secs.
Get full access to this article
View all access options for this article.
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.