
Abstract
Introduction:
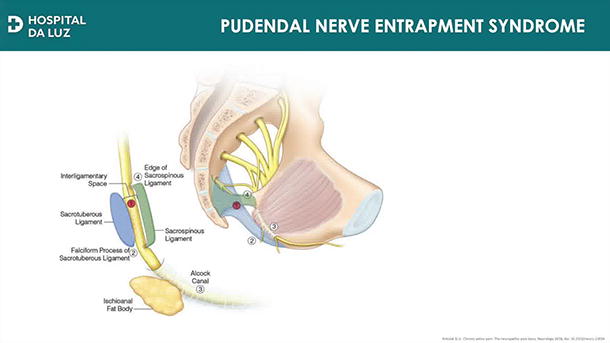
The pudendal nerve (PN) arises from the S2-S4 roots and plays a critical role in motor, sensory, and autonomic functions, with its sensory fibers responsible for the sensation in the perineal area and external genitalia. 1 Compression of the PN can lead to neuropathic pain, often referred to as pudendal nerve entrapment syndrome (PNES), characterized by perineal pain that worsens when sitting. 2 Pudendal neuralgia is a chronic and often disabling condition, and when conservative treatments fail, surgical decompression becomes necessary.
Conservative management of PN neuralgia may include pelvic floor muscle training, pharmacological therapies, PN blocks, or sacral neuromodulation. 3 However, surgical decompression is regarded as the most effective long-term treatment and potential cure. In this report, we demonstrate a minimally invasive, robotic-assisted surgical technique, which provides improved visualization of the sacral roots, minimal bleeding, cosmetic benefits, and quicker recovery, making it a promising option for patients suffering from this debilitating condition.
Clinical History and Physical Exam:
We present a case of a 49-year-old female who reported perineal pain, primarily on the left side, along with numbness and discomfort in the left labia majora. The pain worsened while sitting and was alleviated when lying down. Her symptoms were unresponsive to pharmacological therapy.
Diagnosis:
Pelvic MRI showed no expansive lesions, and a CT-guided pudendal nerve block offered significant symptom relief. Based on the Nantes criteria, the patient was diagnosed with PNES and subsequently recommended for robot-assisted pudendal nerve release.
Intervention:
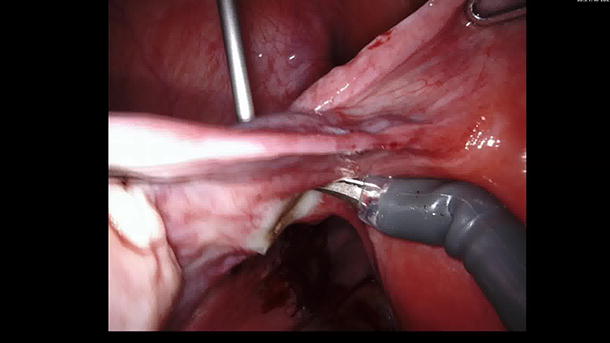
The patient was positioned in a 29° Trendelenburg lithotomy. Four ports were placed in a linear arrangement at the umbilical level for the robotic arms, with two additional ports for the assistant and the insufflator. An incision was made on the posterior aspect of the broad ligaments, and dissection proceeded until the obturator nerve and vessels were identified. By following the avascular plane of the obturator internus, bleeding and damage to lymphatic vessels were avoided. Dissection continued laterally along the arcus tendineus at the level of the pelvic floor muscles. Posteriorly, the fibers of the coccygeus muscle were opened to expose the sacrospinous ligament. Anteriorly, the fascia of the obturator internus was dissected to release the neurovascular pedicle running through the Alcock’s canal. Finally, the sacrospinous ligament was sectioned, allowing for decompression of the pudendal nerve along its course.
Follow-up/Outcomes:
Procedure lasted 2 hours and 15 minutes with minimal blood loss. Patient was discharged the next day, reporting significant symptom relief at follow-up.
Patient Consent Statement:
The patient has provided informed consent to undergo the robot-assisted pudendal nerve release procedure. She has been fully informed about the nature, risks, and benefits of the surgery and has agreed to proceed with the intervention. In addition, the patient has given her consent for the procedure to be recorded on video and for the video to be used for the purpose of publishing and sharing the surgical technique. All personal identifying information will remain confidential.
Author Disclosure Statement:
The author(s) have received and archived patient consent for video recording/publication in advance of video recording of procedure.
Conflicts of Interest and Funding:
The authors report no conflicts of interest. This work did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
The music used in the video is royalty-free and not copyrighted material.
Runtime of video: 4 min and 57 sec.
Video URL: https://videos.liebertpub.com/preview?videoId=fb83c694-ffde-4323-ac25-44e8275a2915.
Get full access to this article
View all access options for this article.