
Abstract
Introduction:
Robotic laparoscopic partial nephrectomy has become a standard in the surgical management of renal tumors. However, achieving consistent and effective resection and renorrhaphy techniques applicable to tumors in various kidney locations remains a challenge. In particular, variation in tumor anatomy in location, polarity, and its endophytic nature may complicate the surgeon’s approach. This video series introduces a universally applicable resection technique for resection and renorrhaphy, ensuring precise tumor removal and optimal renal reconstruction across diverse renal tumor locations.
Material and Methods:
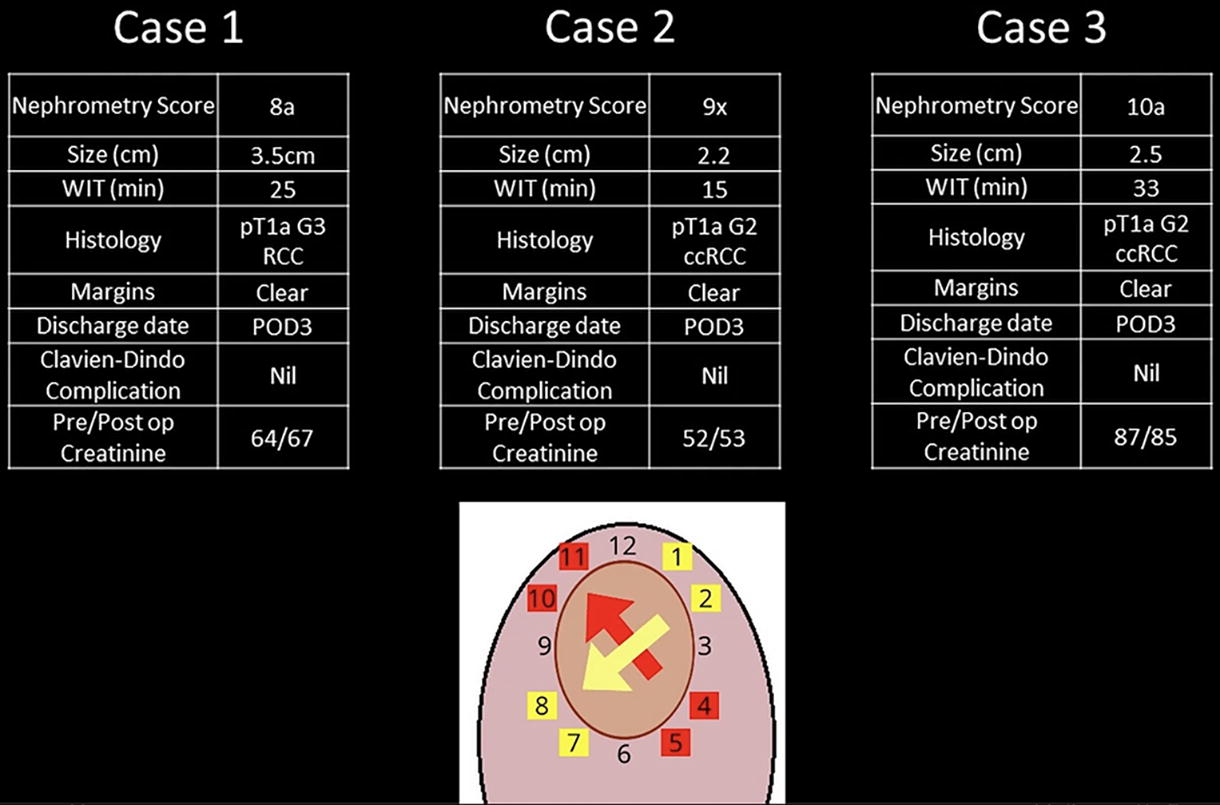
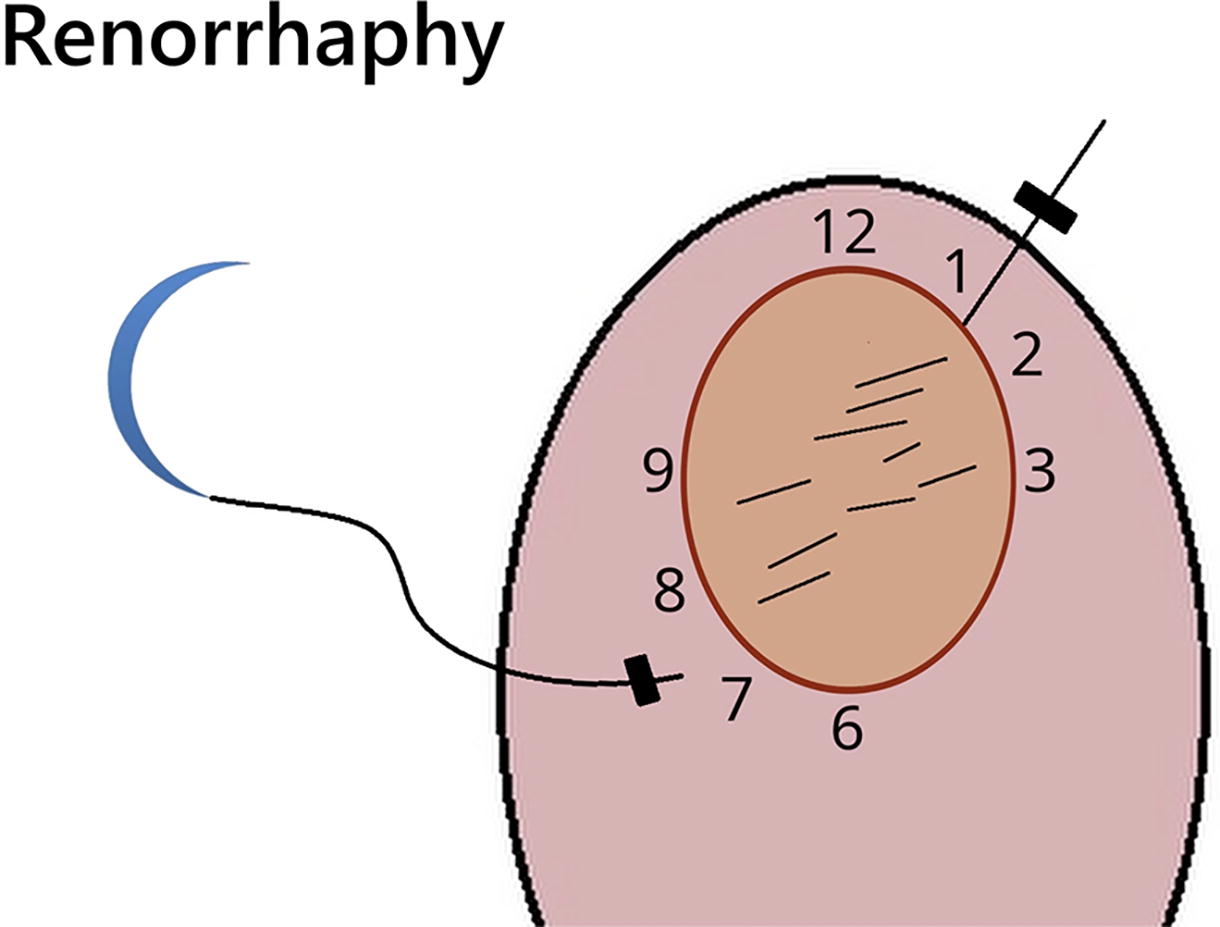
All cases were robot-assisted laparoscopic partial nephrectomy performed by a single surgeon at a tertiary university hospital. Our technique operates on the analogy of a clock, systematically guiding the direction for both the resection and renorrhaphy processes that are the most ergonomic for a right-handed robotic surgeon. For posterior tumors, we describe the preparation required to mobilize the kidney to an optimal position for our technique. These specific preparatory measures include perinephric dissection and the application of a gauze bolster to maintain the kidney in an optimal position. We also describe techniques to provide the optimal retraction with the aid of the surgical assistant, to facilitate better tumor enucleation.
Results:
All patients recovered well postoperatively and were discharged on postoperative day 3. Notably, no Clavien Dindo complications were observed, including requirement for blood transfusion or presence of urine leak. Histology in all cases revealed clear cell renal cell carcinoma, with clear histological margins.
Conclusion:
This standardized approach offers a systematic and replicable method for performing resection and renorrhaphy during robotic partial nephrectomy. Its adaptability to varied tumor anatomy enhances its utility. We hope that this technique can be considered by Uro-oncologists, helping to reduce the risks of R1 resections, extensive hemorrhage/urine leak, and conversions to radical resection.
Funding Acknowledgements:
The authors have no fundings disclosures or conflicts of interest to disclose.
Patient Consent statement:
The authors have received and archived patient consent for video recording/publication in advance of video recording of procedure.
Publication/previous presentation:
At this time this work has not been presented or published at any other journal or conference.
Runtime of video: 6 min, 34 sec
Get full access to this article
View all access options for this article.