
Abstract
Clinical History:
A ureteroduodenal fistula (UDF) is an uncommon diagnosis associated with patient morbidity, including recurrent urinary tract infections, pneumaturia, and flank pain. Surgical management may be complex because of extensive fibrosis and scarring surrounding the UDF site secondary to chronic inflammation.
Physical Examination:
The patient presented with right flank pain.
Diagnosis:
We report the case of a 42-year-old woman with history of a right UDF secondary to iatrogenic injury causing urine extravasation during a ureteroscopy and laser lithotripsy procedure at an outside hospital 1 year prior. The patient was previously managed with chronic ureteral stent exchanges before surgery. A retrograde pyelogram was performed before definitive surgery, which demonstrated a fistula connecting the proximal right ureter to the third part of the duodenum.
Intervention:
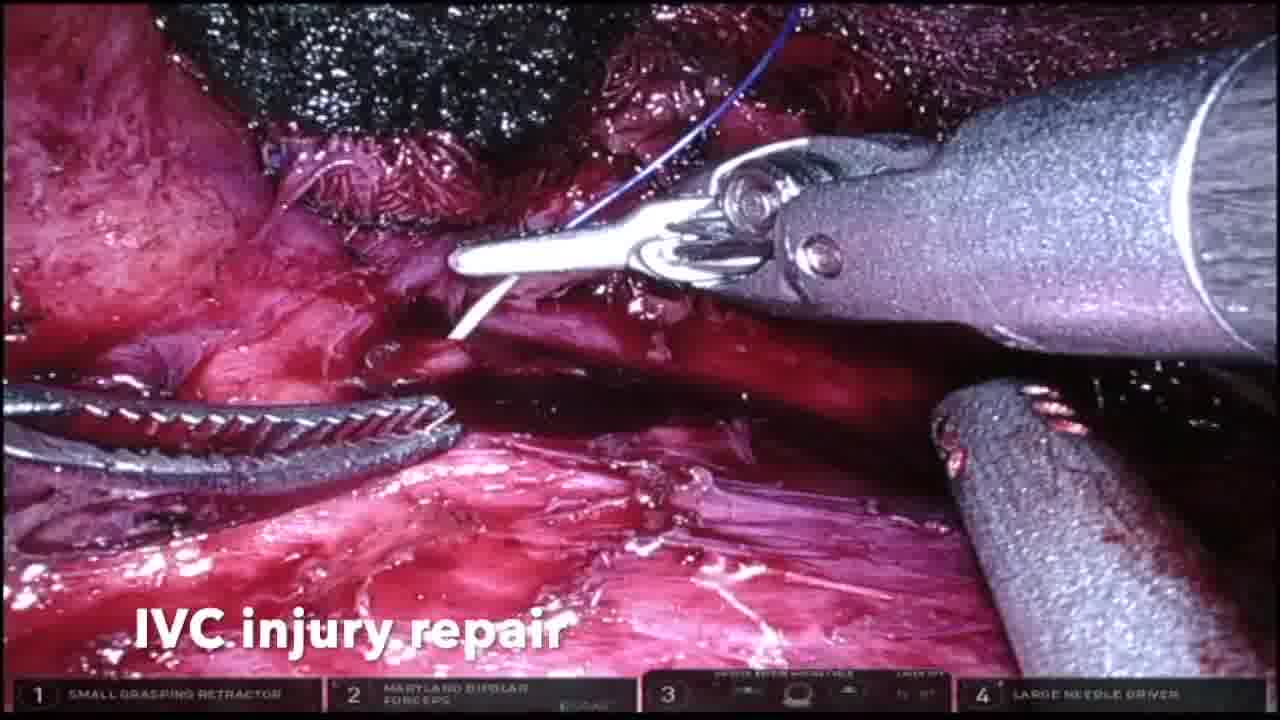
We demonstrate robotic repair of a UDF in a patient with an associated ipsilateral atrophic kidney. Intraoperatively, extensive retroperitoneal fibrosis and purulent debris were evident surrounding the right renal hilum and pelvis. Intraureteral indocyanine green was observed under near infrared fluorescence to aid in dissection. A total right nephrectomy was performed, leaving a 2-cm margin of kidney parenchyma and ureter that remained connected to the duodenal fistula. The general surgery team then performed a duodenotomy and primary repair with omental patch.
Follow-Up/Outcomes:
Intraoperatively, estimated blood loss was 400 mL and operative time was 200 minutes. An upper gastrointestinal series was performed on postoperative day 3 that confirmed no duodenal leak. The patient was discharged on postoperative day 4 after an uncomplicated hospital course. At 16 months follow-up, there were no major (Clavien >2) postoperative complications. Robotic total nephrectomy and UDF repair may be performed effectively in a patient with UDF and associated ipsilateral atrophic kidney.
M.L. and J.J. have no conflicts of interest to disclose. D.E. is founder of Melzi Corp. and a consultant for Intuitive Surgical and Johnson and Johnson
.
Authors have received and archived patient consent for video recording/publication in advance of video recording of procedure. The study was approved by the Institutional Review Board at Temple University (Protocol No. 20793).
Runtime of video: 4 mins 28 secs
Get full access to this article
View all access options for this article.