
Abstract
Introduction:
Renal hypothermia during robot-assisted partial nephrectomy (RAPN) has not yet been fully described, because none of the methods using a minimally invasive approach has gained widespread acceptance. The aim of this study is to present our technique for achieving cold ischemia with ice slush during RAPN.
Materials and Methods:
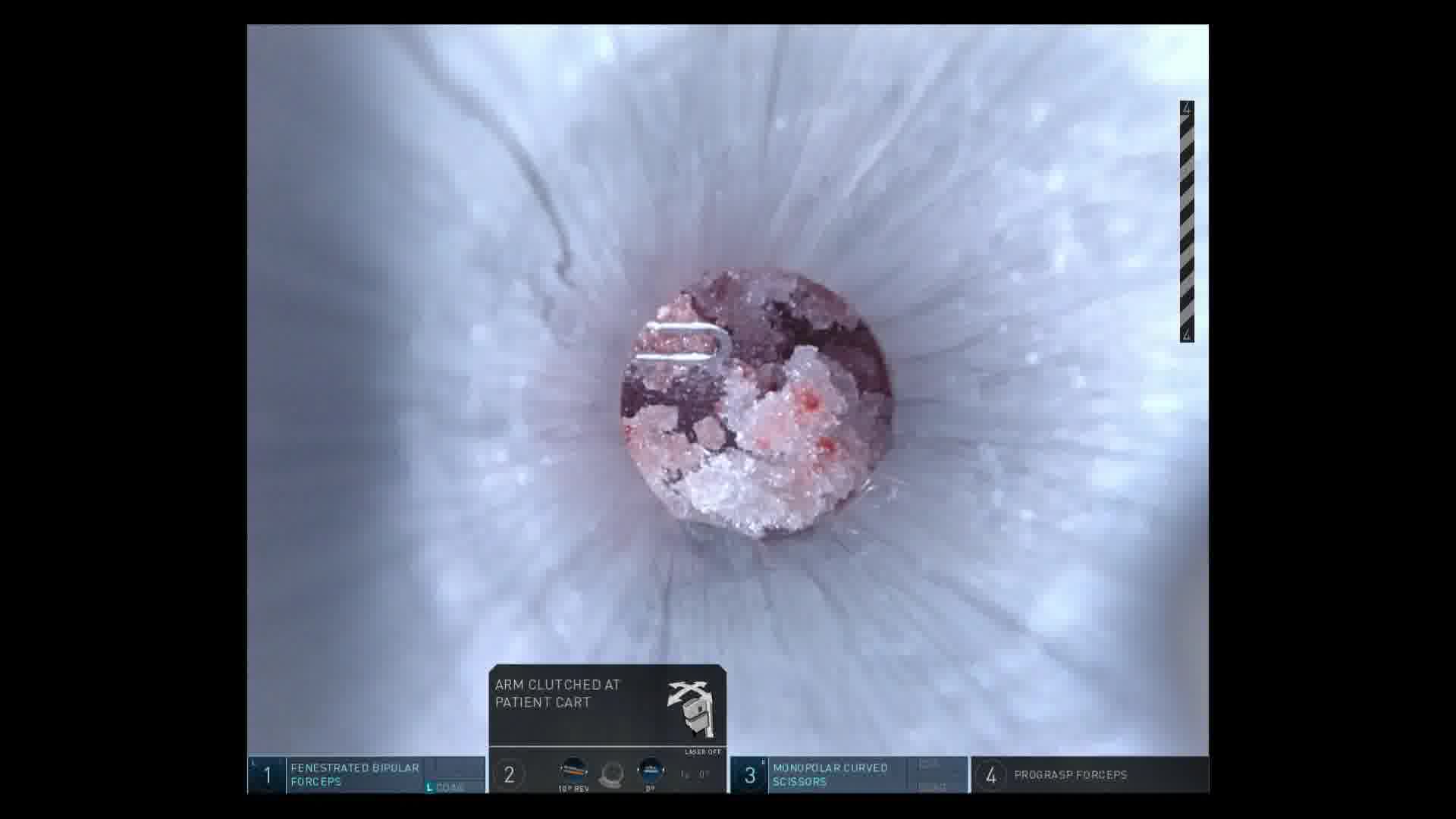
A total of 20 consecutive Japanese patients with solid renal masses underwent RAPN with cold ischemia by retroperitoneal approach between July 2016 and March 2020. An EZ Access (Hakko Co., Ltd., Medical Device Division, Nagano, Japan) port was used for the camera port. After the clamping of the renal artery with or without the renal vein, ice slush >1000 mL was injected through the EZ Access onto the surface of the kidney. After cooling for 10 min, tumor extraction was performed. Perioperative, and 3- and 12-month postoperative functional outcomes in the cold ischemia group were compared with those of a cohort of 32 patients who underwent RAPN with warm ischemia.
Results:
Median RENAL nephrometry score was 9 (range: 4–10) in cold ischemia group and 7 (range: 4–10) in warm ischemia group. Mean cold ischemia time was 39.3 min (range: 22–53) and mean warm ischemia time was 23.6 min (range: 10–43). The mean postoperative rate of decline of estimated glomerular filtration rate evaluated at 3 months and 1 year was 8.3% ± 15.2% and 18.5% ± 9.6% in cold ischemia group and 6.5% ± 10.2% and 9.4% ± 16.8% in warm ischemia group, respectively. As for the functional outcomes, there were no significant differences between the two groups, despite tumor extraction tended to be technically difficult in the cold ischemia group. There were no postoperative severe complications. The limitations of this study include a small number of patients and short-term follow-up.
Conclusions:
RAPN with renal hypothermia using intracorporeal ice slush is technically feasible and may improve postoperative renal function in the short term. Our method of introducing the ice slush was not complicated and highly reproducible.
Corresponding author has received and archived patient consent for video recording/publication in advance of video recording of procedure.
No competing financial interests exist.
Runtime of video: 11 mins 36 secs
Get full access to this article
View all access options for this article.