
Abstract
Introduction:
Penile torsion is a debatable condition as no consensus exists about its definition, or management. It is a rotational defect of the penile shaft, resulting in an abnormal penile twisted on its axis. The degree of torsion is measured as the angle between a line passing through the urethral meatus and the midline of the scrotum. Recent studies have shown that the dartos, which is the smooth muscle layer lying under the penoscrotal skin, might be responsible for penile torsion and curvature, and it may be associated or not with other congenital penile malformations. 1 The dartos tissue is considered as a superficial fascia, located immediately under the genital skin, originating in Scarpa's abdominal fascia, and in Colle's perineal fascia. 2 The composition of fibro muscular dartos tissue along the penile shaft determines elasticity of the subcutaneous tissue and the skin mobility. Any structural change in organization of these components may influence these characteristics, and might, therefore, be responsible for torsion/chordee. Torsion as a stand-alone condition is usually asymptomatic, but correction of torsion is important; it is even to preserve the genital sensitivity and potency. Whether treatment is needed or not becomes purely esthetic. Many techniques using flaps or penile degloving have been described when correction is desired, all of them being reported in small series. 3
Materials and Methods:
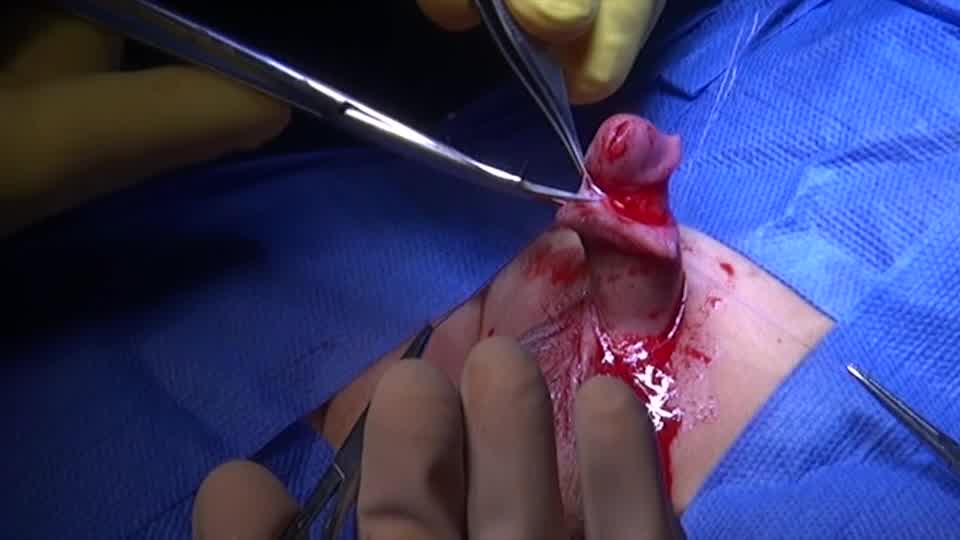
In this study, the least invasive technique, which is most often sufficient to correct mild torsion, was used. Generally penile torque varies from 15° to 180°, and monosymptomatic rotation of <60° considered mild and does not require treatment. 4 This technique was applied in 15 children aged 2 to 6 years, penile degloving, dissection, and resection of the anchoring dysplastic dartos fascia with fixation of the root of the penis in the proper position by applying nonabsorbable stitches between the Bucks fascia and subcutaneous penile skin. Parents of all involved cases gave a consent for both the surgery and using their children data for publication.
Results:
Successfulness of the technique was assisted intraoperatively through an artificial erection and in the follow-up that was commenced at 2 and 6 months postoperatively. Thirteen patients had an acceptable penile look with correction of the rotation either completely with 10° angle of rotation in nine and residual minimal rotation of 10° to 30° in four cases. Two patients with severe degree of torsion (about 180°) had a partial but nonsatisfactory results, and they scheduled for another technique, and it involve penile deglovement, with resection of disorganization dartos tissue, which could be aberrant, thereby usually correcting the problem.
Conclusion:
In this technique penile degloving, dissection, and resection of the anchoring dysplastic dartos fascia with fixation of the root of the penis in the proper position by applying nonabsorbable stitches between the Bucks fascia and subcutaneous penile skin results in an acceptable penile look. Deglovement is insufficient, when some other pathologic mechanism than pure dartos was detectable.
Author have received and archived patient consent for video recording/publication in advance of video recording of procedure.
Author disclosed that there is no any conflict of interest and there is no any commercial associations during the past 3 years that might create a conflict of interest in connection with the submitted video
.
Runtime of video: 3 mins 12 secs


Get full access to this article
View all access options for this article.