
Abstract
Clinical History:
A 41-year-old man with history of bladder exstrophy managed with cystectomy and ureterosigmoidostomy developed left flank pain. Work-up revealed severe left-sided hydroureteronephrosis and accompanying atrophic left kidney caused by an obstructing sigmoid colonic mass at the left ureteral orifice. Colonoscopy and biopsy revealed adenocarcinoma and staging imaging confirmed localized cancer. The patient elected to undergo a robotic left nephroureterectomy with en bloc sigmoid resection.
Intervention:
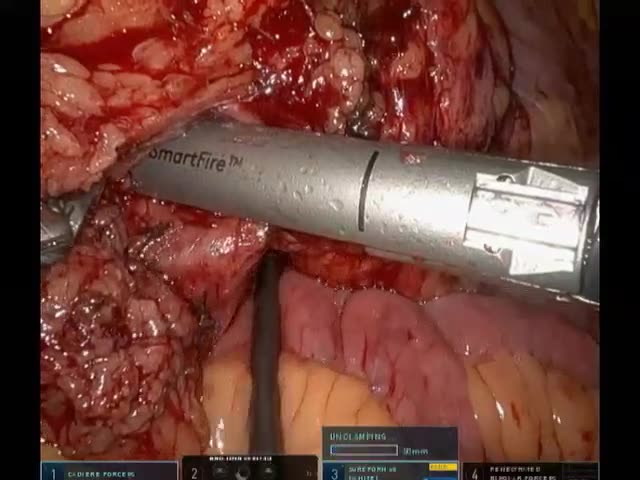
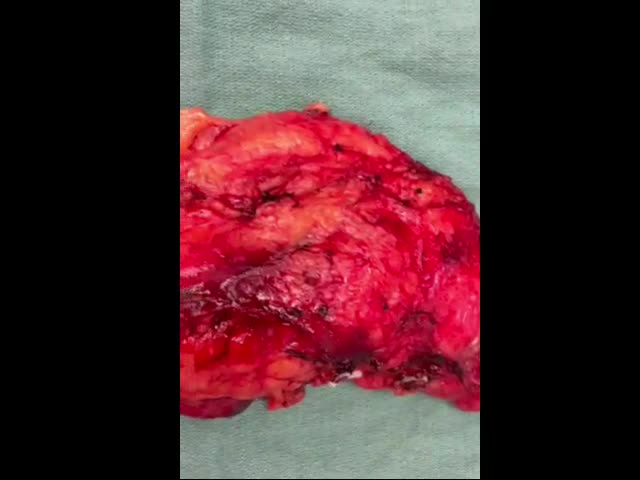
The patient was positioned in a right lateral decubitus position with ports placed as depicted in the accompanying video. A left nephrectomy was performed in the standard manner with the ureter left intact and dissected freely down to its insertion point into the sigmoid colon. The patient was repositioned into low lithotomy and steep Trendelenburg to perform an en bloc sigmoid colon resection. Flexible sigmoidoscopy and preoperative right ureteral stent placement were utilized to ensure the right ureteral orifice was excluded from the colonic resection. A Natural orifice-assisted IntraCorporeal anastomosis with transrectal Extraction of specimen (NICE) procedure was performed to extract the specimen transrectally and restore bowel continuity. To our knowledge, this is the first transrectally extracted kidney specimen reported in the literature.
Follow-up/outcomes:
Postoperatively the patient had a routine course, meeting discharge milestones by postoperative day 2. He was seen in the clinic at 2 and 4 weeks postoperatively and was noted to be functioning at his baseline with excellent continence.
No competing financial interests exist.
Patient Consent:
Consent was obtained from the patient to publish this video.
Runtime of video: 5 mins 0 sec
Get full access to this article
View all access options for this article.