
Abstract
Urologists are commonly faced by a challenging situation in patients with significant or complicated lower urinary tract symptoms caused by large prostate glands (>80 g). 1,2 Although open simple prostatectomy (OSP) has been considered the gold standard in such scenarios, it is still associated with substantial perioperative complications of up to 42%. 3 Robot-assisted simple prostatectomy was regarded as the evolution of OSP in a minimally invasive direction and has been published in the literature. 4,5 This video demonstrates different robot-assisted transperitoneal approaches for massive (>100 cc) benign prostatic hyperplasia.
Technique:
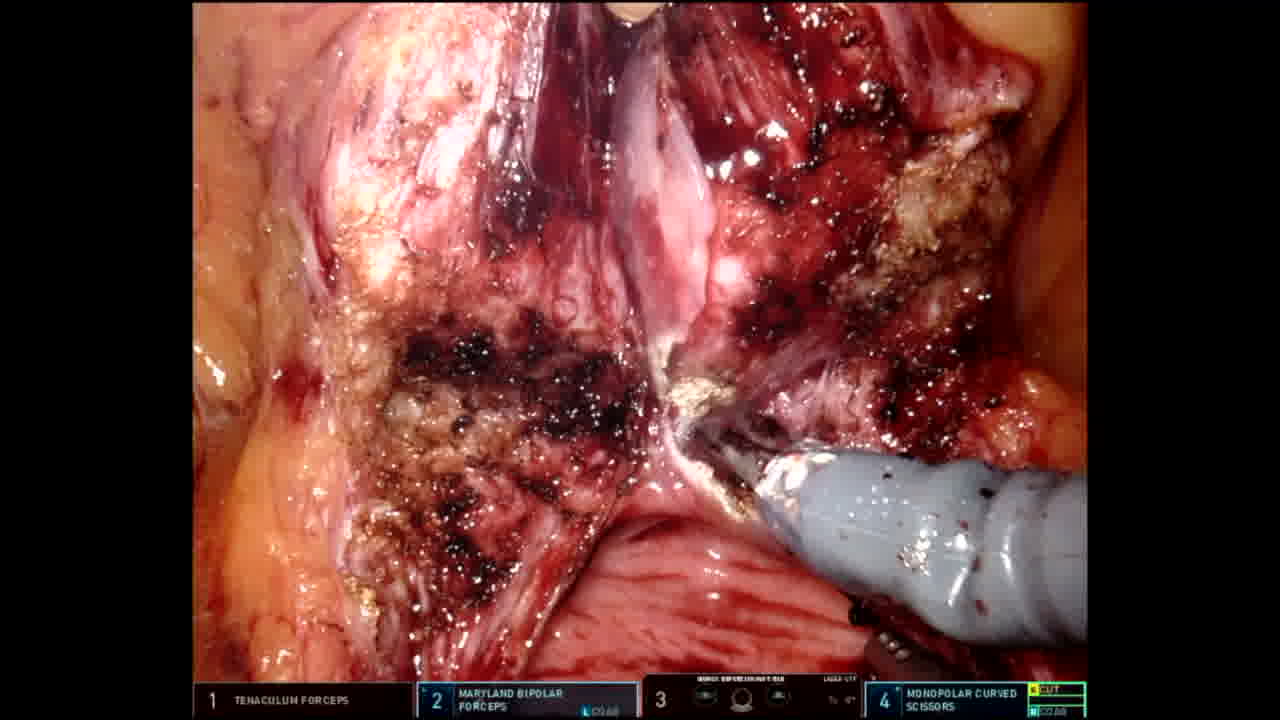
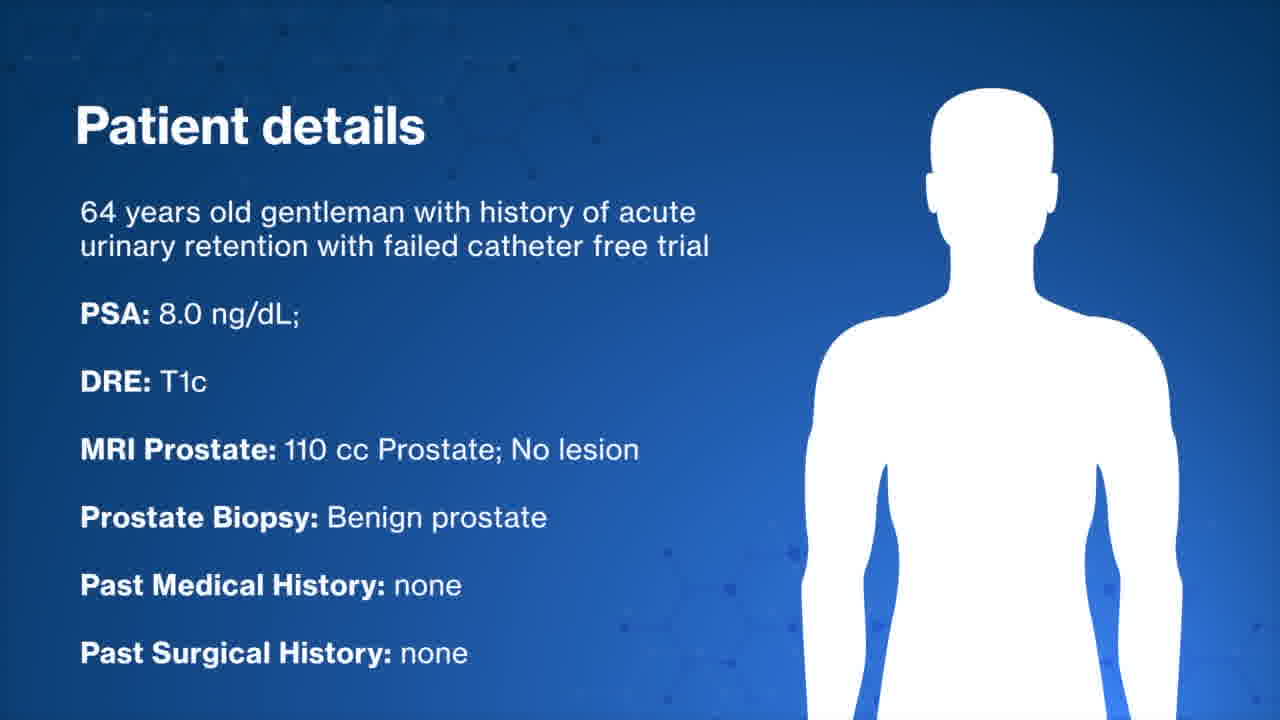
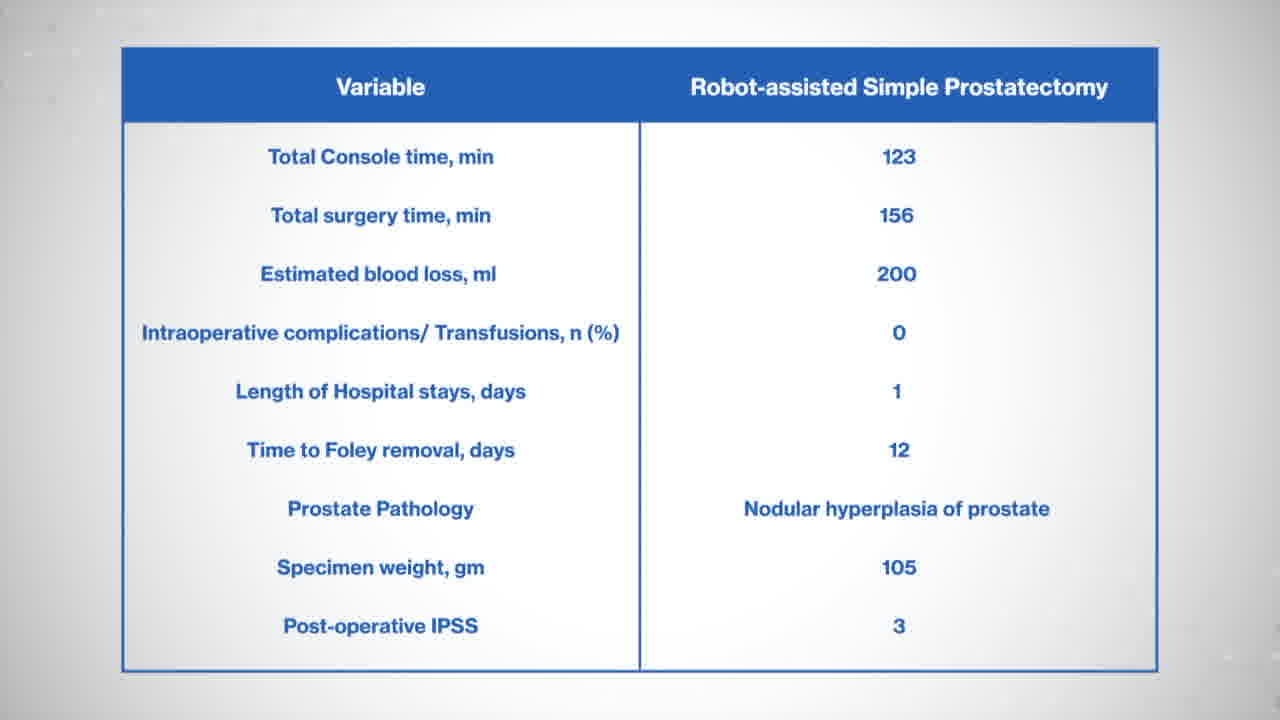
1. Suprapubic approach: A case shown here is 58 years old gentleman with history of acute urinary retention and failed trial of void. His prostate volume was 154 cc and biopsy showed benign prostate. Patient was positioned in steep Trendelenburg and six laparoscopic ports were inserted (four robotic and two for assistant). After bladder drop, anterior bladder neck is incised and deepened till the Foley catheter was seen. The catheter grasped with third arm with firm anterior traction. Using the shaft of the catheter as a landmark, the mucosa at the posterior bladder neck was incised precisely. We then developed a plane under the posterior bladder neck and above the peripheral zone of the prostate. We then developed a plane between the adenoma (transition zone) and the peripheral zone of the prostate. We continued in the developed plane all the way to the apex of the prostate. Then, the urethra was sharply dissected and the specimen was collected. Using a V-lock suture and a self-cinching technique, we completed the posterior reconstruction. A tension-free urethrovesical anastomosis is performed using double armed strata-fix suture. There was no intra- or perioperative complications. Patient stayed overnight and catheter was removed on postoperative day 12. He noticed significant improvement in Benign prostatic hyperplasia symptoms (BPH)-nocturia, weak urinary stream & incomplete emptying. 2. Transvesical approach: A 64 years old gentleman presented with history of acute urinary retention and failed trial of void. His prostate volume was 110 cc and biopsy showed benign prostate. The bladder was distended with 300 mL sterile saline and the dome was identified. A vertical bladder incision was made from the dome to the mid bladder. A circular mucosal incision was made around the bladder neck, and prostate tissue was dissected away from the bladder, starting posteriorly and then progressing laterally and anteriorly. Posteriorly we entered the plane between the transition zone and the peripheral zone of the prostate. Dissection was continued in the plane posterolaterally and anteriorly up to the apex of the gland. A robotic tenaculum was used to aid with retraction of the BPH tissue. Hemostasis was achieved with electrocautery during dissection. After dissection of the apex, the foley was removed and the urethra was transected. The BPH tissue was removed en bloc and placed in an endocatch bag. Hemostasis was achieved in the resection bed and the dead space of the resection site was closed with running 3-0 V-lock sutures. The ureteral orifices were identified with clear urine efflux. A tension-free urethral anastomosis was completed with double armed Stratafix suture. 18F foley catheter was inserted without difficulty catheter balloon is inflated with 30 mL sterile saline. Bladder closure was performed in two layers. A 2-0 Stratafix suture was used to close the detrusor and mucosal layers, with careful approximation of the mucosal edges.The patient was discharged next day. Cystogram followed by catheter removal was performed on postoperative day 12. He noticed significant improvement in BPH symptoms. In total 50 men underwent robotic simple prostatectomy. Patients presented with a baseline International prostate symptom score of 23 and a median prostate-specific antigen of 7.7 ng/mL. Median preoperative prostate volume was 167 cc. In 80% of cases, patients had an indwelling foley catheter. Median console time was 118 minutes, and median estimated blood loss was 148 mL. None of our cohort needed intraoperative transfusion, conversion to open surgery, or developed any complications. Median time to foley removal was 10 days. Significant improvement in Qmax was noted over the period of follow-up.
Conclusions:
Robot-assisted simple prostatectomy through transperitoneal approach is feasible in massive BPH with favorable functional outcomes. Comparative studies evaluating efficacy of this procedure with endoscopic treatment of massive BPH are warranted to provide further evidence.
Music Source:
Copyright:
Author owns copyright/license for the music used in the video.
Dr. A.K. Tewari has served as a site-PI on pharma/industry-sponsored clinical trials from Kite Pharma, Lumicell, Inc., Dendreon, and Oncovir, Inc. He has received research funding (grants) to his institution from DOD, NIH, Axogen, Intuitive Surgical, AMBFF, and other philanthropy. Dr. A.K. Tewari has served as an unpaid consultant to Roivant Biosciences and advisor to Promaxo. He owns equity in Promaxo. Rest of the authors do not have conflicts of interests.
Author(s) have received and archived patient consent for video recording/publication in advance of video recording of procedure.
Runtime of video: 15 mins 10 secs
Get full access to this article
View all access options for this article.