
Abstract
Introduction:
Persistent mullerian duct syndrome (PMDS) is a rare congenital disorder of sexual differentiation, which occurs because of lack of anti-Mullerian hormone (AMH) or defect in receptor of AMH. The most common presentation is bilateral undescended testis (UDT) with varying amount of persistent mullerian duct remnants.
Case Details:
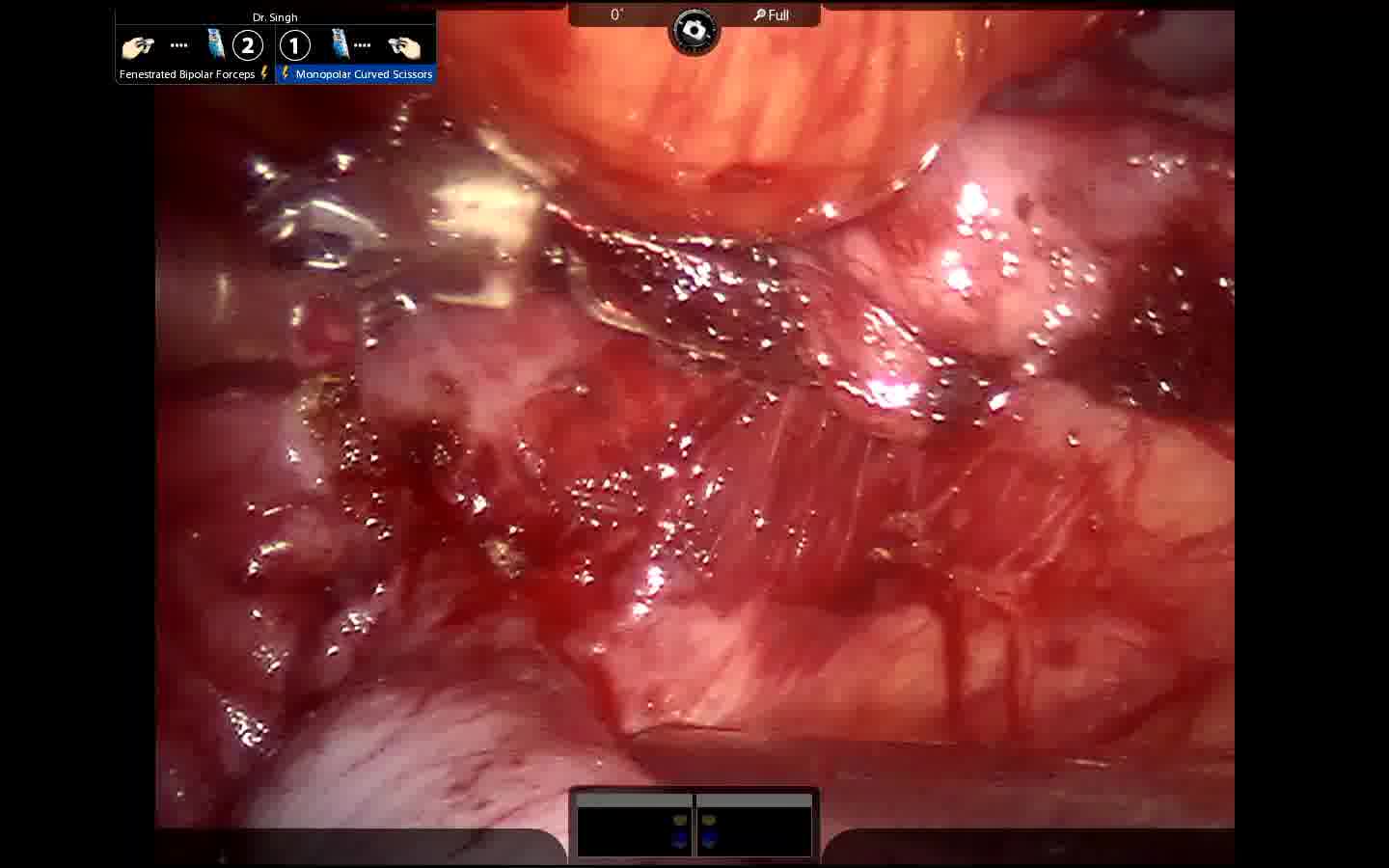
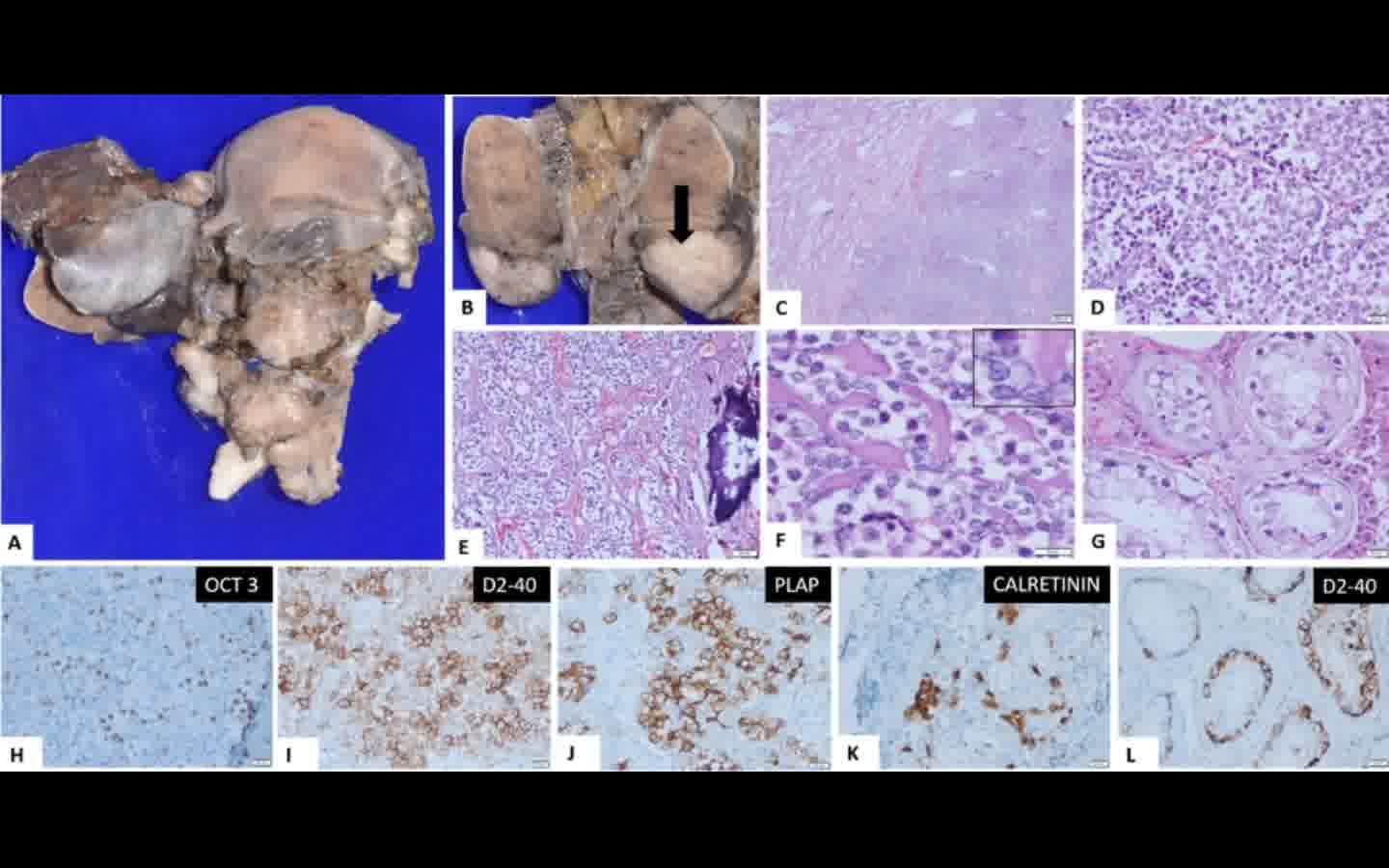
A male patient in his early 20s presented with complaints of lower abdominal pain and pain during ejaculation. Examination showed normal penis and bilateral UDT with rudimentary scrotum. Magnetic resonance imaging revealed bilateral UDT and also distended uterus with cervical canal and bilateral fallopian tubes. Karyotyping done showed 46XY genotype. Patient underwent right orchidopexy with left orchidectomy and excision of persistent mullerian duct remnants. Intraoperatively both testes were located at deep inguinal ring and left testes was also found to be abnormal with nodular growth on its surface. Well-developed uterus and cervix with bilateral fallopian tubes were also found. Postoperative recovery was uneventful and patient was discharged on second postoperative day. Histopathology report revealed seminoma in the left testes.
Discussion:
PMDS characteristically presents as a patient with 46XY karyotype and normal male external genitalia but with persistent mullerian duct structures. Majority of these patients (80%) present with bilateral undescended intra-abdominal testes. The management principles of PMDS is to preserve fertility and avoid complication of malignancy. Orchidopexy should be attempted in the early age itself to preserve the hormonal function of the testes. Increased risk of malignancy either from undescended testes or mullerian remnants is the major concern in patients of PMDS.
Conclusion:
Robot-assisted excision of mullerian remnants with or without orchidopexy for surgical management of PMDS is feasible with good outcome. Magnified three-dimensional vision with robot assistance helps in doing meticulous dissection in deep pelvis to prevent injury to important structures.
No competing financial interests exist.
Authors have received and archived patient consent for video recording/publication in advance of video recording of procedure.
Runtime of video: 04 mins 53 secs
Get full access to this article
View all access options for this article.