
Abstract
Introduction:
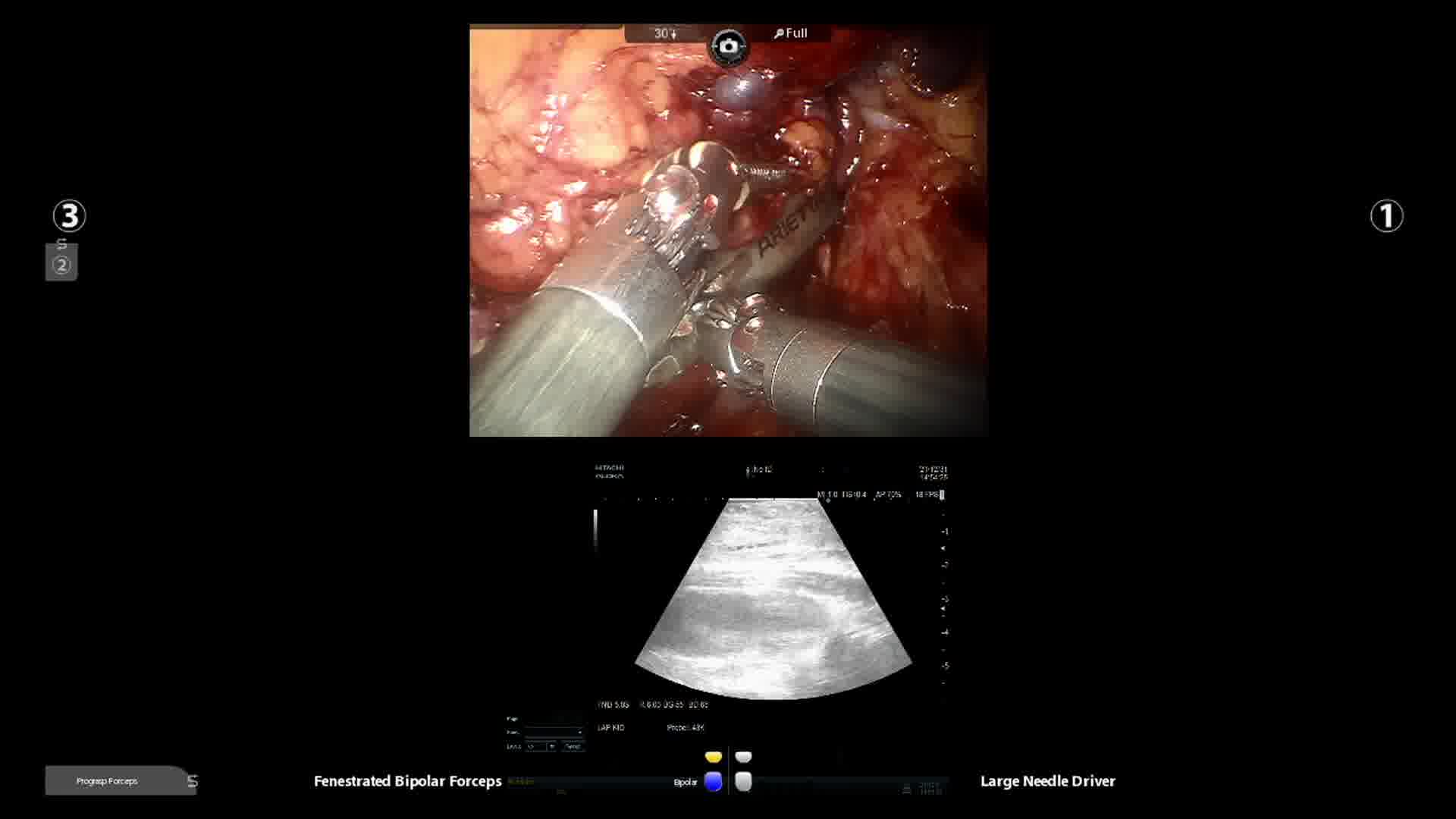
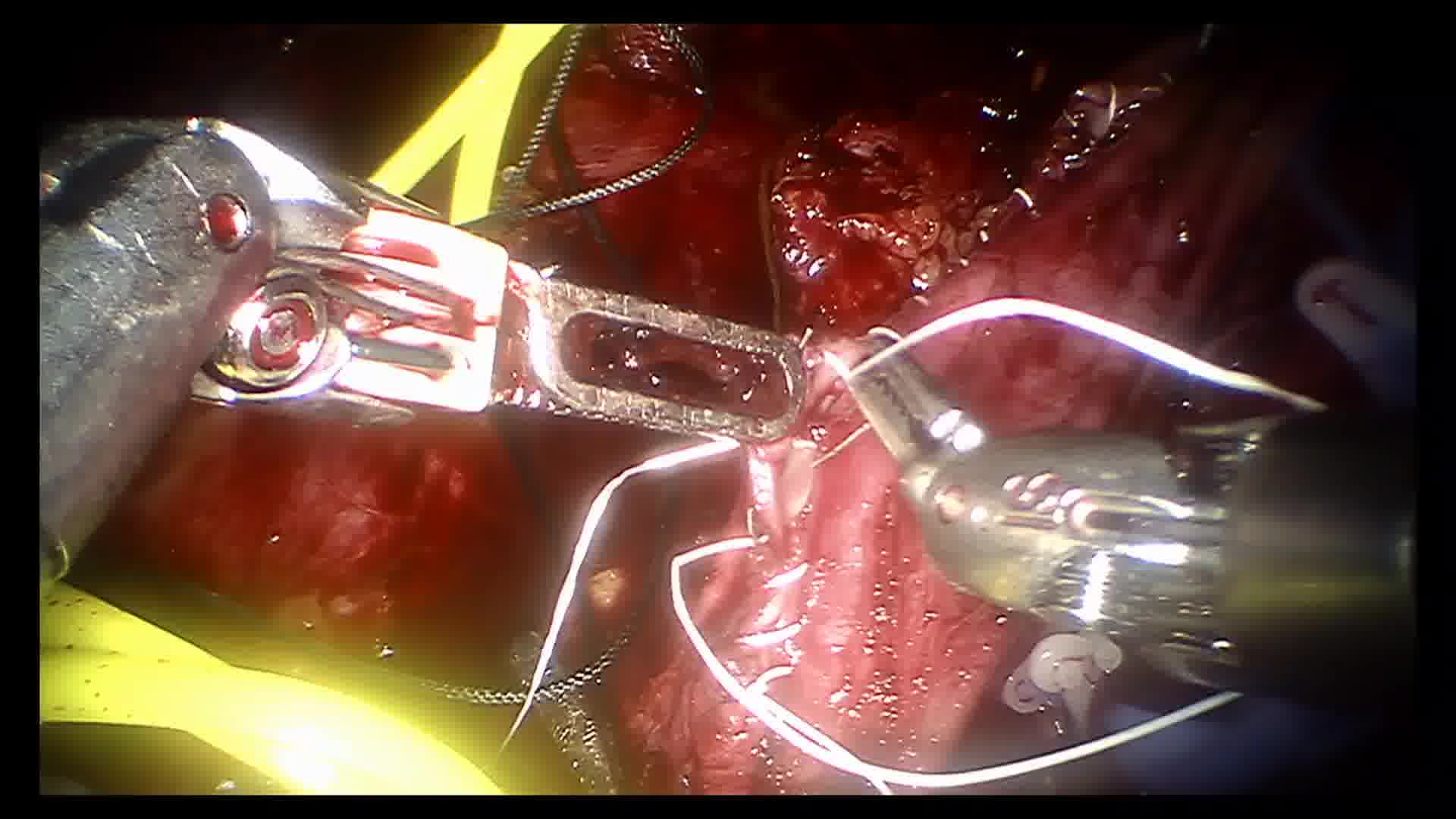
To present our experience in a series of patients with robot-assisted inferior venecava thrombectomy and radical nephrectomy (RAITRN) with emphasis on level 3 thrombus and suprahepatic control of inferior venecava (IVC). RAITRN with suprahepatic clamping has been previously reported only from a center in China. 1,2 There have been studies on cadaveric model done by leading centers in the United States. 3,4 Till now, the technique has not been reproduced in any centers outside China. The video depicts the technique of liver mobilization and suprahepatic control of IVC.
Materials and Methods:
Retrospective analysis of data collected from two patients who had RAITRN from September 2019 to December 2021 was carried out. This study was approved by the ethics committee of Aster Medcity Hospital, Kochi, India, and written informed consent was taken from all the patients for the study. Da Vinci Si system (Intuitive Surgicals Sunnyvale, CA) was utilized. In level 3 thrombus, the patient was in supine position and the left lobe of liver was mobilized. The falciform ligament, left triangular ligament, and gastrohepatic ligaments were divided. The left lobe of liver was mobilized and suprahepatic IVC was dissected off the caudate lobe. Radical nephrectomy and right lobe liver mobilization were performed after converting the position to 90° flank right side up position. After mobilizing the right lobe of liver, a vascular loop was placed beneath the IVC from the right side directed toward the left side. Subsequently the patient was placed in 45° flank position, the vascular loop was retrieved from the left side of the IVC, and circumferentially encircled over the suprahepatic IVC. Finally, the patient was again tilted back to 90° right side flank up position and IVC thrombectomy was accomplished.
Results:
Case I was a 58-year-old male patient with a body mass index (BMI) of 25.09 kg/m2 and a left-sided renal tumor with level 3 IVC thrombus, IVC clamp time was 21 minutes, thrombus length was 10.5 cm, console time was 270 minutes, total operative time was 370 minutes, and blood loss was 320 mL. Nadir postoperative creatinine was 1.2 mg%, pathologic staging was pT3N0M0 clear cell renal cell carcinoma, the patient received no adjuvant treatment, and was disease free at the end of 30 months after surgery. Case 2 was a 59-year-old male patient with a BMI of 24.95 kg/m2 and a right-sided renal tumor with a level 3 IVC thrombus, IVC clamp time was 26 minutes, thrombus length was 11 cm, console time was 280 minutes, total operative time was 440 minutes, and blood loss was 150 mL. Nadir postoperative creatinine was 1.5 mg%, pathologic staging was pT3N0M0 grade 4 papillary renal cell carcinoma, the patient received no adjuvant treatment, and was disease free at the end of 6 months after surgery.
Conclusions:
RAITRN can be performed safely in level 3 thrombus where a suprahepatic clamping is required. An experienced multidisciplinary team including urologist, hepatobiliary surgeon, and a skilled bedside assistant is of paramount importance in these advanced robotic procedures. Prolonged operative time and multiple changes in position may be considered a limitation.
No competing financial interests exist.
Author(s) have received and archived patient consent for video recording/publication in advance of video recording of procedure.
Runtime of video: 09 mins 47 secs
Get full access to this article
View all access options for this article.