
Abstract
Introduction:
The technique used for the bladder neck (BN) dissection and reconstruction during robot-assisted radical prostatectomy (RALP) can influence the continence rate. A detailed BN dissection usually allows for the early achievement of a continent BN. 1,2 However, sparing the BN is not always possible. According to presurgery tumor and anatomical features, a subgroup of patients necessitate a wider resection of the base, considered imperative for obtaining negative margins and better oncologic outcomes. 3 In such cases, a more extensive BN reconstruction might be required. Nowadays, ventral and dorsal reconstruction are the most frequently adopted techniques to overcome the mismatch between the BN and the urethral stump. 4,51 Both reconstruction methods are adequate, however, suffer from inferior early continence rates when compared with BN sparing techniques. 1 The aim of this video is to present our technique for BN reconstruction during RALP.
Materials and Methods:
The 3/0 Monocryl (Ethicon®) polyglecaprone 25 suture was used to perform the BN reconstruction during RALP and is highlighted in this video demonstration. This consists of a single-layer through-and-through suture, resembling the that used in gastrointestinal surgery to perform bowel anastomosis and described by Connell. 6 Surgical steps to perform this method of BN reconstruction are depicted in the video footage. As a result, this suture recreates a BN that more accurately resembles the native one when compared with the traditional reconstruction techniques.
Results:
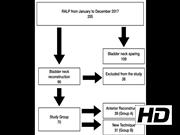
Total reconstruction time was 13 minutes. A 16F Foley catheter was inserted after completion of the anastomosis and removed on the sixth postoperative day. At 6 and 12 weeks after catheter removal, the patient required 1–2 pads per day and 0–1 incontinence pads per day, respectively. After a follow-up of 18 months, no anastomotic stricture was observed. With regard to our experience, between January and December 2017, 205 patients underwent RALP in our center and 70 received a BN reconstruction. According to the reconstruction performed, the patients were divided into two groups: A (n = 39) received the anterior BN reconstruction and B (n = 31) received our technique. Patients were evaluated at 1, 3, and 6 months and urinary incontinence was assessed through the validated Expanded Prostate Cancer Index Composite questionnaire. A prospective trial is in progress, but our preliminary data, which are reported in detail in the video, show promising results in terms of early urinary continence recovery and impact on the quality of life. 7
Conclusions:
Our technique is a feasible alternative to the anterior and posterior techniques that can be used to reconstruct the BN during RALP. This continuous introflecting suture results in a BN with a conic shape that resembles the original anatomy. Although not statistically significant, our initial results show superiority of our technique on early urinary continence recovery, if compared with the anterior reconstruction. A prospective trial with a larger number of patients is currently on at our department and the results will be available in the near future.
No competing financial interests exist.
Runtime of video: 6 mins 9 secs
Consent:
Authors have received and archived patient consent for video recording/publication in advance of video recording of the procedure.


Get full access to this article
View all access options for this article.