
Abstract
Introduction:
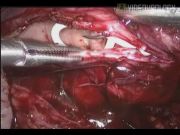
Open dismembered pyeloplasty is a gold standard for managing ureteropelvic junction (UPJ) obstruction resulting in a success rate >90%. 1 The conventional open surgery for failed pyeloplasty is very challenging because of the fibrosis and scarring at the previous surgical site. The current options for managing the failed pyeloplasty are endopyelotomy or redo pyeloplasty, which can be an open, laparoscopic or robot-assisted approach. 2 The ureterocalicostomy is considered to salvage the kidney when there are no other options. The redo pyeloplasty is equally difficult with both the open and laparoscopic approach. We present a video demonstration of laparoscopic redo pyeloplasty. The port positions are depicted in the illustration. After achieving the pneumoperitoneum, the colon was reflected along the line of toldt. The affected renal unit and dilated renal pelvis were exposed after incising Gerota's fascia. The normal ureter was identified and dissection was continued proximally toward the UPJ using cold scissors. The ureter was disconnected from the pelvis and spatulated laterally after excising fibrous tissue and unhealthy segment of ureter completely. Pyelotomy was performed and flap was created out of the lower lip of renal pelvis. The kidney was released from perinephric and fibrous tissue to get tension-free anastomosis. The apical suture was placed between the spatulated ureter and dependent part of the renal pelvis, followed by opposite corner suture. The anterior layer of anastomosis was completed with interrupted suture using 4-0 polyglactin. The neo-pelviureteric junction was upturned, an antegrade Double-J stent was placed, and the posterior layer of anastomosis was completed. The renal pelvis flap was tubularized followed by excision and closure of redundant renal pelvis. Hemostasis was achieved, a drain was placed, and port closure was done.
Materials and Methods:
A 24-year-old male patient presented with recurrent left loin pain after open pyeloplasty. Detailed evaluation revealed recurrent pelviureteric junction obstruction. Laparoscopic redo pyeloplasty was performed. Operative and postoperative details were recorded. The patient was followed up at regular intervals. We analyzed the perioperative and intermediate term functional outcome of all patients who underwent laparoscopic redo pyeloplasty at our center.
Results and Conclusion:
A total of 16 patients presented with failed pyeloplasty. Eleven patients had undergone open pyeloplasty, four patients laparoscopic, and one patient robotic-assisted pyeloplasty. In two patients, endopyelotomy was attempted without success. Fifteen patients underwent laparoscopic redo pyeloplasty and one patient underwent laparoscopic ureterocalicostomy. In three patients, crossing vessel was found. The mean (SD) age was 16.03±11.53 years and the mean preoperative glomerular filtration rate (GFR) was 29.49±6.08 mL/min. The mean duration of surgery was 191.25±24 minutes and the mean duration of hospital stay was 3.2±0.45 days. The mean postoperative GFR was 32.42±6.40 mL/min and the mean duration of follow up was 29.9±18.5 months. There were no operative and postoperative complications. The success rate was 93.3%. The redo pyeloplasty is a successful alternative to endopyelotomy for failed pyeloplasty. To achieve a successful outcome, fibrous tissue should be excised completely avoiding thermal injury, anastomosis should be tension-free, and a Double-J stent should be placed always. The laparoscopic approach, which offers a satisfactory outcome with a low morbidity profile, however, should be attempted by the urologist with experience in reconstructive procedures.
No competing financial interests exist.
Runtime of video: 5 mins 58 secs


Get full access to this article
View all access options for this article.