
Abstract

Introduction:
Medullary thyroid carcinoma (MTC) accounts for approximately 5% of all thyroid cancers. 1 The majority of cases (75%) are sporadic; however, the remaining 25% are associated with hereditary syndromes and conditions. 1 The multiple endocrine neoplasia type 2B (MEN2B) syndrome is an autosomal dominant hereditary cancer syndrome and accounts for 5% of all hereditary MTCs with an incidence of 1/38,750,000.2–4 It is the rarest and most aggressive form of MEN2, associated with early-onset MTC and metastases at diagnosis, pheochromocytoma, mucosal ganglioneuromas, gastrointestinal symptoms, skeletal deformity and Marfanoid habitus.3–6 Nevertheless, few of these signs and symptoms manifest during the first 12 months of life. 7 Failure to thrive due to sucking weakness, chronic constipation and reduced lacrimation can start within the first months of life after uneventful intrauterine development and birth. 7 More than 95% of cases presents an M918T mutation on exon 16 of the RET proto-oncogene. 4 The current standard treatment is prophylactic total thyroidectomy within the first year of life, although a minority of patients actually benefits of this procedure since most of them are not recognized early enough.2–6
Materials and Methods:
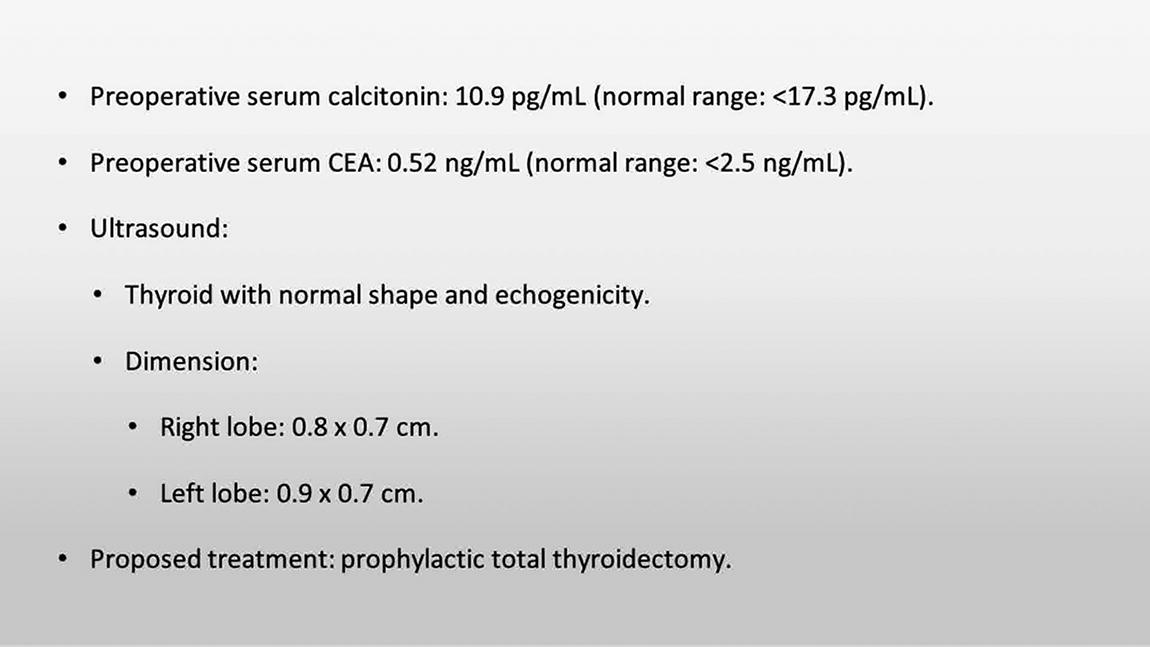
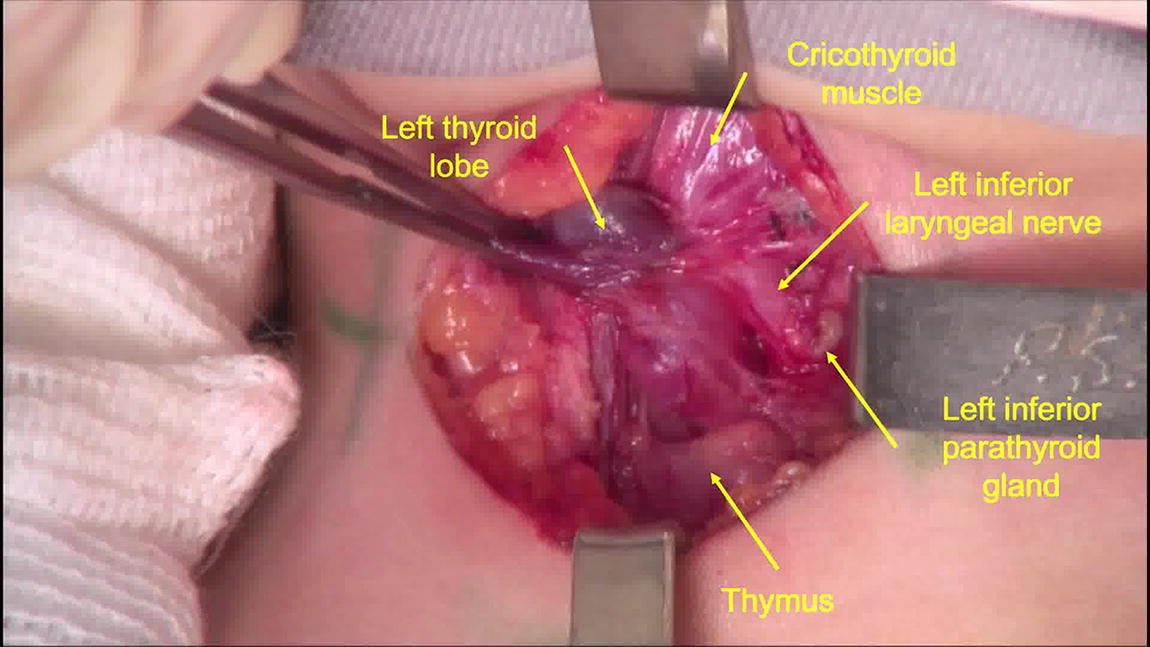
A female infant was born to a mother with known MEN2B due to M918T RET proto-oncogene mutation. Her mother has advanced metastatic disease (cervical lymph nodes, bone, lung, and liver) and underwent total thyroidectomy and lymph node dissection at age 17. The infant had uneventful birth and no signs of disease other than constipation and a tongue neuroma. She underwent genetic testing at 6 months of age, which confirmed the same mutation. Serum calcitonin at 6 and 9 months of age was 17.6 and 10.9 pg/mL (normal range: <17.3 pg/mL), whilst carcinoembryonic antigen was 0.52 and 0.5 ng/mL (normal range: <3.5 ng/mL) at the same period. Neck ultrasound showed a thyroid with normal shape and echogenicity without nodules. Prophylactic total thyroidectomy was performed at 10 months of age. Parathyroid glands and both recurrent laryngeal nerves were visualized and left in situ. No palpable lymph nodes during surgery were noticed. Extreme caution with bleeding and adjacent structures were conducted.
Results:
The Perioperative course was unremarkable. She recovered without complications. The thyroid gland weighed 6 grams and histopathology and immunohistochemistry showed no lesions on the thyroid gland, not even C cell hyperplasia. First post-operative day calcitonin concentration was 2.5 pg/mL and the parathyroid hormone was 26 pg/mL (normal range: 15–65 pg/mL).
Conclusions:
This case report highlights that prophylactic thyroidectomy within the first year of life remains the standard course of treatment for patients with MEN2B and M918T RET proto-oncogene mutation. When feasible, it should be done in a high-volume center with expertise in thyroid disease management and by experienced professionals. Some technical considerations should be attempted to improve outcomes: use of optical magnification and more delicate instruments, extreme care with bleeding, dissection close to the thyroid capsule, caution with tiny parathyroid glands, rigorous hemostasis, and greater care for post-surgical hypocalcemia.
Disclosure statement:
The authors have no commercial associations or conflicts of interest to declare.
Acknowledgment:
The authors sincere gratitude to Dr. Magnabosco, BF, DDS, for her contribution to the audio narration.
Source of work:
The authors have no funding/financial support to declare.
Conflicts of interest:
The authors have no related conflicts of interest to declare.
Consent:
Written informed consent was obtained from the patient’s mother for publication of this case report and accompanying images.
Runtime of video: 10 min
Get full access to this article
View all access options for this article.