
Abstract
Abstract
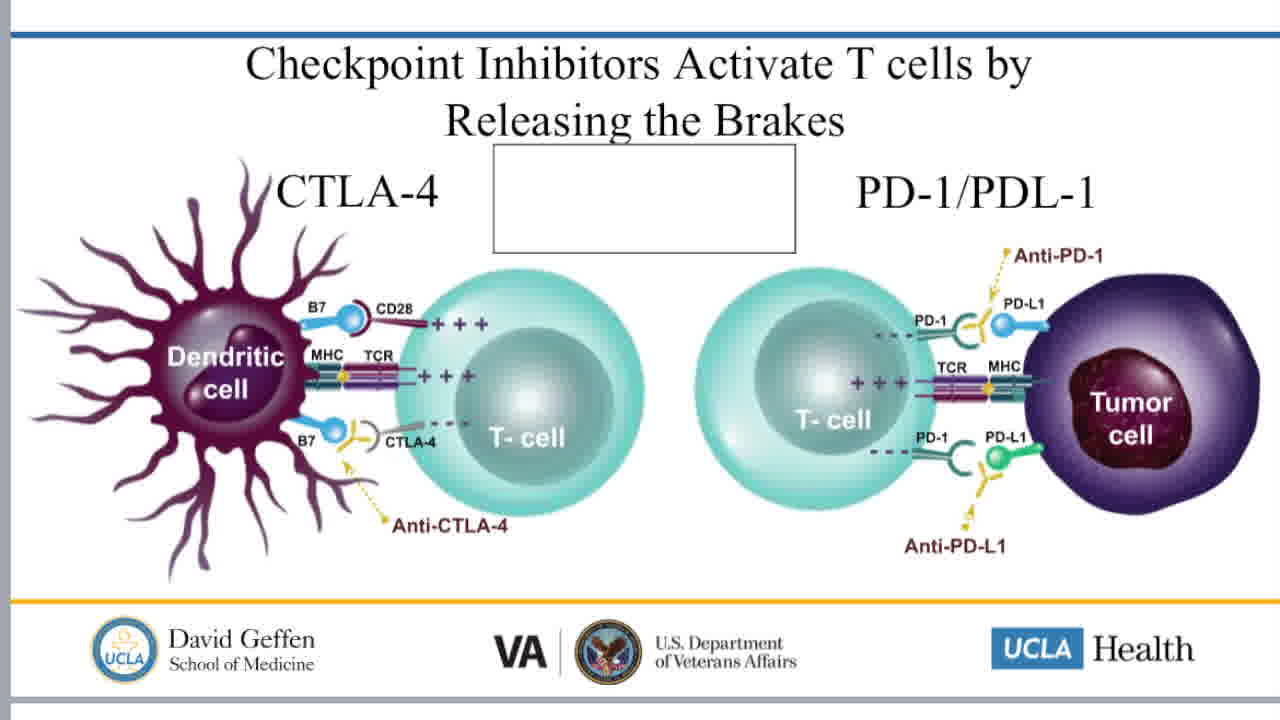
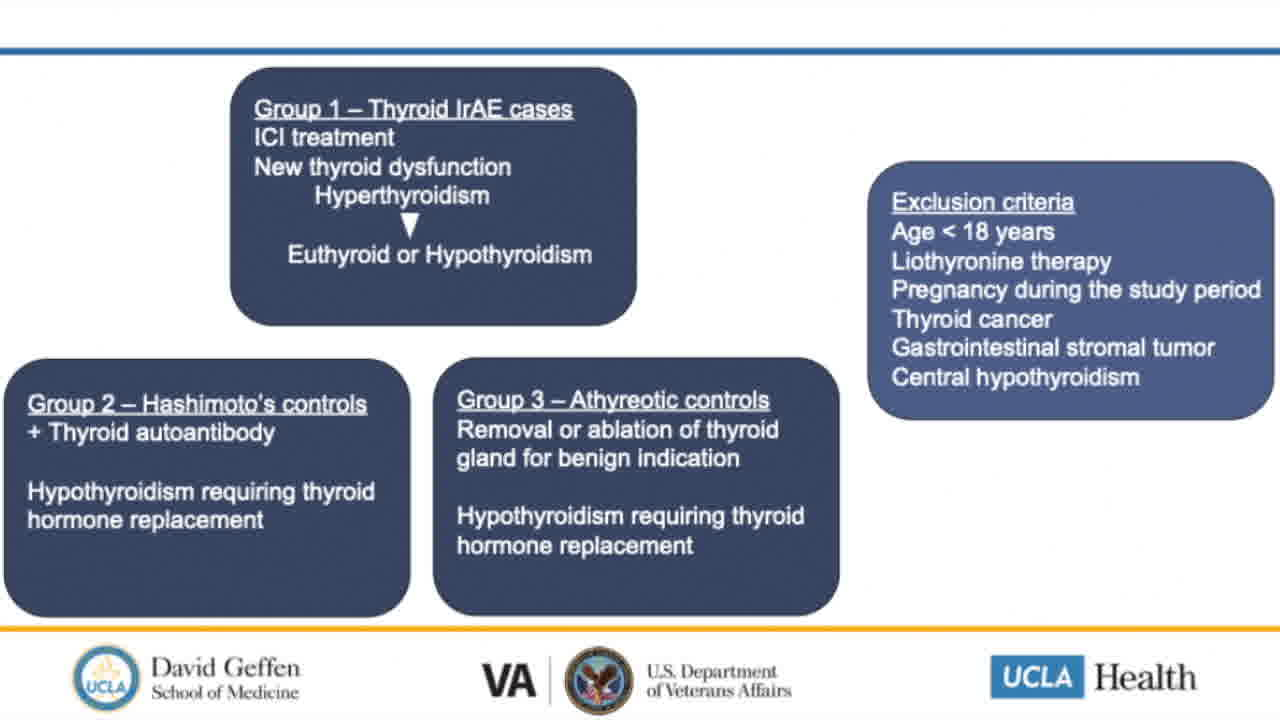
In this Video Endocrinology Fireside Chat we discuss our recent report by Mosaferi et al. entitled “Optimal Thyroid Hormone Replacement Dose in Immune Checkpoint Inhibitor-Associated Hypothyroidism Is Distinct from Hashimoto's Thyroiditis” published in Thyroid, 2022. Lead author Dr. Tina Mosaferi, of the VA Greater Los Angeles Health System and the UCLA Geffen School of Medicine, discusses the clinical observations prompting our investigation, the study design and results, and the significance of our findings with respect to evolving recommendations for patient care. Thyroid dysfunction is the most common endocrine immune-related adverse event in patients treated with immune checkpoint inhibitor (ICI) cancer therapy, occurring in ~15% to 25% of patients treated with combination antiprogrammed death protein-1 and anticytotoxic T lymphocyte antigen-4 therapy, and 10% to 15% of patients treated with ICI monotherapy therapy. Hypothyroidism may occur abruptly after rapid-onset thyroiditis, and the optimal thyroid hormone replacement dose can be difficult to ascertain in light of concurrent nonthyroidal illness and interfering medications. Initiation of ideal thyroid hormone dose at diagnosis may minimize the adverse consequences of inadequately treated hypothyroidism or iatrogenic hyperthyroidism. In this study, we reported the weight-adjusted dose of thyroid hormone needed to achieve stable euthyroid status in patients with ICI-associated hypothyroidism. Furthermore, we determined that the thyroid hormone requirement in these patients is similar to athyreotic patients, but distinct from patients with Hashimoto's thyroiditis. These findings can provide a basis for recommended initial thyroid hormone replacement doses in patients with ICI-thyroiditis managed by endocrinologists, oncologists, or primary care providers.
No competing financial interests exist
.
Runtime of video: 9 mins 38 secs

Keywords
Get full access to this article
View all access options for this article.