
Abstract
Background:
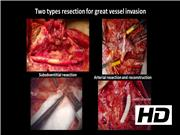
Extrathyroidal invasion has the greatest negative prognostic impact among several adverse prognostic factors of differentiated thyroid carcinoma (DTC). Surgical treatment for locally advanced DTC is challenging. In particular, the presence of great vessel involvement makes it more challenging, with vessel rupture and infection being common occurrences, especially in patients with laryngotracheal or esophageal intraluminal invasion. Locoregional tumors presenting with great vessel and/or multiple organ invasion have been deemed to be unresectable. However, there has been little discussion regarding which types of locoregional tumor are unresectable. For great vessel invasion, two types of resections are performed: subadventitial resection and en-bloc resection of the great vessel, with or without reconstruction of the artery. For cases in which tumor invasion did not exceed the arterial adventitia, complete resection of the tumor from the subadventitial layer is performed, with preservation of the great vessel. For cases in whom invasion exceeded the arterial adventitia, we proceeded with arterial resection and reconstruction.
Materials and Methods:
A right thyroid tumor was unexpectedly detected in a 77-year-old man by computed tomography images. The man was found to have papillary thyroid carcinoma (PTC) by fine needle aspiration biopsy. He was referred for surgical treatment of multiple organ invasion by PTC. Tumor encasement of about 180° of the right common carotid artery and aerodigestive tract invasion were suspected on preoperative magnetic resonance imaging. We performed total thyroidectomy, including resection of multiple organ infiltration and right lateral neck dissection. Subadventitial resection of the common carotid artery was performed using a No. 15 surgical blade under microscope guidance. Our surgical strategy for locally advanced DTC is implemented with curative surgical intent for all patients and functional preservation or reconstruction, if possible.
Results:
The thyroid tumor infiltrated the right common carotid artery, internal jugular vein, prevertebral fascia, pharyngoesophagus, laryngotrachea, and right recurrent laryngeal nerve (RLN). We performed subadventitial resection of the common carotid artery, partial prevertebral fascia resection, muscle layer resection of the pharyngoesophagus, framework resection of the larynx, window resection of the trachea from first to fourth ring, and resection and intralaryngeal reconstruction of the right RLN. After tumor resection, the right common carotid artery was covered using a deltopectoral flap and separated from the tracheocutaneous fistula. Pathology analysis confirmed PTC, which was classified as pT4bN1bM0. The tracheocutaneous fistula was closed 2 months after surgery. The patient underwent radioactive iodine (RAI) adjuvant therapy of 100 mCi, 6 months after surgery. RAI uptake was noticed in only the thyroid bed. Maximum phonation time was 10 sec, 6 months after surgery.
Conclusions:
This video illustrates the technical details of subadventitial resection of the great vessel. This surgical technique is effective for improving surgical curability and functional preservation.1
No competing financial interests exist.
Runtime of video: 9 mins
Funding Information: No funding was received for this article.


Get full access to this article
View all access options for this article.