
Abstract
Abstract
Introduction:
Mediastinal ectopic parathyroid adenomas (MEPAs) are a rare cause of primary hyperparathyroidism, constituting 1%–2% of all parathyroid adenomas. 1 Traditional surgical management entailed sternotomy or thoracotomy for excision, approaches associated with postoperative morbidity. 2 Since the early 1990s, there has been increasing application of video-assisted thoracoscopic surgery (VATS) for resection of MEPAs, with single-center and regional studies reporting improved outcomes.3–7 We present a demonstrative video case report detailing management of a MEPA using VATS.
Materials and Methods:
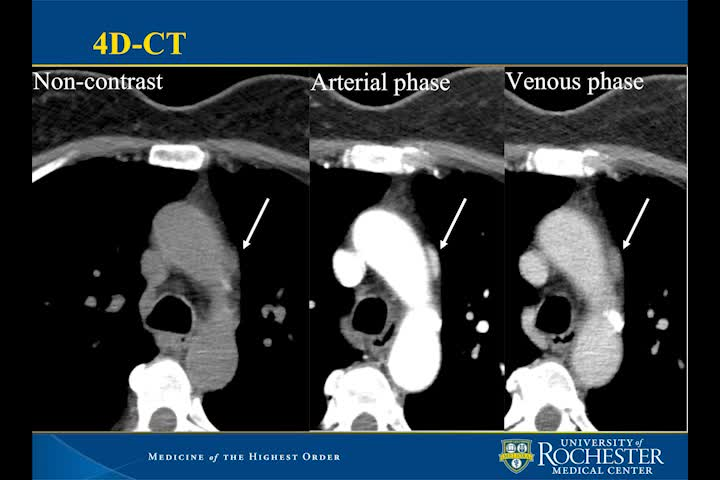
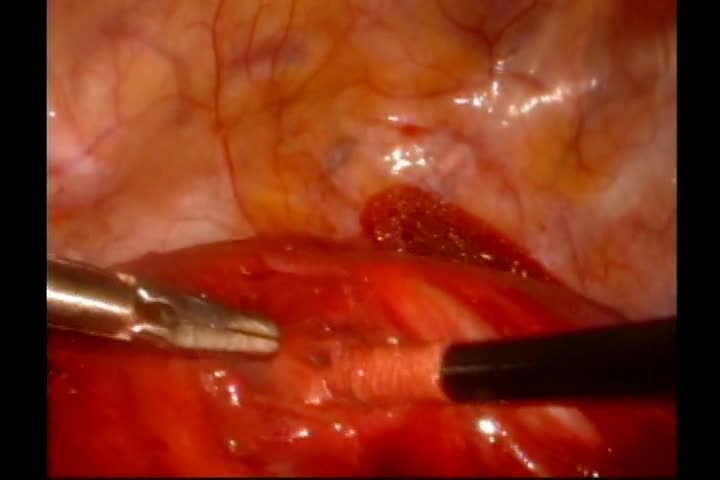
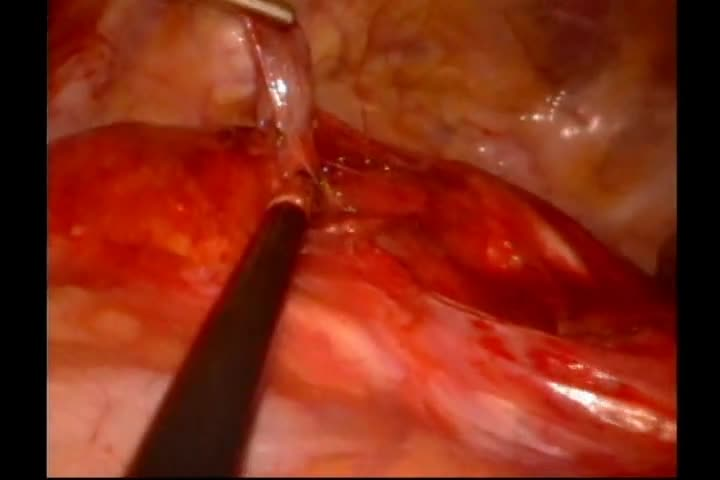
A 62-year-old female presented with aches, pains, and fatigue. Her medical history was significant for depression, on bupropion therapy. Initial work-up demonstrated serum calcium of 10.9 mg/dL (2.7 mmol/L) and a simultaneously elevated parathyroid hormone (PTH) level of 87.8 pg/mL. Pertinent laboratories, including 25-hydroxyvitamin D, creatinine, albumin, and urine microalbumin, were unremarkable, consistent with primary hyperparathyroidism. 8 She had no known history of nephrolithiasis or osteoporosis. Tc99m-sestamibi scan suggested a left intrathoracic parathyroid adenoma, and she was referred for surgical evaluation. In-office thyroid ultrasonography showed a solitary 1.6 cm heterogeneous right thyroid nodule, diagnosed as a colloid nodule by fine-needle aspiration, but no observed parathyroid abnormality. A four-dimensional CT scan (noncontrast, arterial contrast, and delayed venous phases) localized the parathyroid tissue adjacent to the aortic arch at the aortopulmonary window. The patient was taken to the operative suite and placed in the right lateral decubitus position. A dual lumen endotracheal tube was placed to isolate the left lung. Three transthoracic ports were placed. Intraoperative localization with methylene blue was contraindicated given the risk of serotonin syndrome and patient intolerance to bupropion wash out preoperatively.9,10 Blunt and sharp dissection was used to dissect the presumed parathyroid tissue. PTH levels were monitored. A metal clip was placed at the site of resection to serve as a radiologic marker. The pleural cavity was thoroughly irrigated. Finally, a chest tube was placed intraoperatively.
Results:
Serum PTH levels were 73.3 pg/mL pre-excision, 25.9 pg/mL 5 minutes post-excision, and 24.8 pg/mL 10 minutes post-excision. 11 At the night of surgery, her serum PTH level was 35.4 pg/mL, and her serum calcium was 8.3 mg/dL (2.1 mmol/L). Histopathology demonstrated hypercellular parathyroid tissue. Her postoperative course was uneventful. Her chest tube was removed and she was discharged on postoperative day 2. She was regularly seen at routine follow-up visits with resolution of her symptoms and serum calcium that have remained normal.
Conclusions:
We present a video case report of a VATS resection of an MEPA. Our approach for this patient differed from other reports of surgical management of hyperparathyroidism, where MEPAs may only be identified in cases of persistent or recurrent primary hyperparathyroidism.12,13 In this case, preoperative imaging allowed for definitive identification. A VATS approach allowed for a short and uneventful postoperative recovery. When not contraindicated, we recommend use of our reported techniques in addition to intraoperative methylene blue. At this time, given the rarity of MEPA, large multicenter studies assessing outcomes after VATS are lacking, and further investigation is necessary.
Source of Work or Study:
The source of work was during the normal course of clinical practice at an academic medical center utilizing the normal laboratory, imaging, and surgical instruments in our standard of care.
No competing financial interests exist.
Runtime of video: 10 mins 23 secs
Keywords
Get full access to this article
View all access options for this article.