
Abstract
Sleep-wake disturbances (SWDs) are common after TBI and often extend into the chronic phase of recovery. Such disturbances in sleep can lead to deficits in executive functioning, attention, and memory consolidation, which may ultimately impact the recovery process. We examined whether SWDs post-TBI were associated with morbidity during the post-acute period. Particular attention was placed on the impact of sleep architecture on learning and memory. Because women are more likely to report SWDs, we examined sex as a biological variable. We also examined subjective quality of life, depression, and disability levels. Data were retrospectively analyzed for 57 TBI patients who underwent an overnight polysomnography. Medical records were reviewed to determine cognitive and functional status during the period of the sleep evaluation. Consideration was given to medications, owing to the fact that a high number of these are likely to have secondary influences on sleep characteristics. Women showed higher levels of disability and reported more depression and lower quality of life. A sex-dependent disruption in sleep architecture was observed, with women having lower percent time in REM sleep. An association between percent time in REM and better episodic memory scores was found. Melatonin utilization had a positive impact on REM duration. Improvements in understanding the impact of sleep-wake disturbances on post-TBI outcome will aid in defining targeted interventions for this population. Findings from this study support the hypothesis that decreases in REM sleep may contribute to chronic disability and underlie the importance of considering sex differences when addressing sleep.
Introduction
Long-lasting memory impairments and emotional/behavioral issues that have an impact on life quality are prevalent after traumatic brain injury (TBI),1–3 with women reporting a higher percentage of symptoms.4–6 The cognitive and emotional sequelae of TBI may be additionally exacerbated by sleep-wake disturbances (SWDs).7–9 Prevalence of SWD is higher after a TBI compared to the general population.8,10 Sleep is known to be an essential component of daily living, impacting cognition and emotional regulation.11–16 Of interest is the role that sleep architecture plays in memory. 17 Persons with no SWDs cycle through sleep stages that include wakefulness, non-rapid eye movement (NREM) sleep, and rapid eye movement (REM) sleep. NREM sleep is further divided into three stages (N1, N2, and N3) and includes oscillations associated with learning and memory.16,18,19 REM sleep has also been demonstrated to facilitate memory.20–23
Women are more likely to report insomnia and excessive daytime sleepiness.24–28 Moreover, sex differences in network organization during REM sleep have been observed in polysomnography (PSG) studies.29,30 In this observational study, we aimed to identify SWDs during the post-acute TBI period while considering sex as a biological variable. We hypothesized that disruptions in N3 and REM sleep stages would be associated with cognitive deficits. We also examined subjective quality of life, depression, and disability levels. Consideration was given to medications, given that a high number of these are likely to have secondary influences on sleep characteristics.
Methods
Study population
Study methods were approved by an institutional review board. We conducted a retrospective chart review of TBI patients having underwent a type I, fully attended overnight PSG while being treated at a post-acute rehabilitation facility (Centre for Neuro Skills, Dallas, TX; Bakersfield, CA). Exclusion criteria were: 1) under the age of 18 years or over the age of 60 years, 2) past diagnosis of neurodegenerative disease, 3) diagnosis of SWD before TBI, and 4) poor signal quality during PSG recording.
Medical records from the rehabilitation facility were reviewed to determine functional status during the period of the PSG sleep evaluation. The following assessments were utilized: Mayo Portland Adaptability Inventory 4 (MPAI); California Verbal Learning Test 2 (CVLT); Neurological Quality of Life Questionnaire (Neuro QoL) subscales; and the Beck Depression Inventory II (BDI). Medical records of medications taken during the night of the PSG that may impact sleep were documented for analysis.31–37
Polysomnography
Sleep studies were performed by a Registered Polysomnographic Technologist (PSG-1100; Nihon Khoden, Irvine, CA). Recordings included frontal, central, and occipital electroencephalogram, electrooculogram, submentalis and anterior tibialis electromyography, body position, nasal and oral airflow, electrocardiogram, and oxygen saturation. Sleep staging and scoring was done according to the American Academy of Sleep Medicine manual, version 2.5. Apnea was scored at ≥3% oxygen desaturation. The Epworth Sleepiness Scale was utilized to detect subjective sleepiness.
Statistical analysis
Statistical analyses were performed using PRISM software (version 9.5.1; GraphPad Software, San Diego, CA). Variables were evaluated for normality/lognormality. Two group comparisons were analyzed either through Mann-Whitney U or t-tests. All statistical tests were two-tailed. Data are reported as mean ± standard error of the mean (SEM). Mixed-model analysis was utilized to evaluate sex differences in Neuro QoL measures. For the analysis of sleep stages and memory, men and women were pooled to decrease the risk of type II errors attributable to low statistical power. Analyses of variance and corrected multiple comparisons were performed to compare REM sleep time below and above the normative percentage according to age.38–41 The following groups were compared: Low-Range-REM (<14% REM); Mid-Range-REM (14–22% REM); and High-Range-REM (>22% REM). Linear regression analysis was also utilized to determine the influence of REM on learning and memory.
Analysis of medication use during the sleep evaluation was performed in a binary manner. Fisher's exact tests were utilized to compare group differences in recorded medications. Power analysis indicated that sample sizes were insufficient to analyze the impact of REM sleep on memory while considering sex. To increase the sensitivity of detecting the potential effect of medications on sleep, men and women were pooled. Logistic regression was utilized to evaluate the association and probabilities between binary (medication utilization) and non-binary (percentage of time spent in REM sleep) variables. Significance was determined by a likelihood ratio test. Sensitivity and specificity for significant values were indicated with receiver operating characteristic (ROC) curves.
Results
A total of 64 records were reviewed. Of those, 57 subjects met the inclusion criteria and consisted of 40 men and 17 women (percentage of 70% male). This study population is representative of the incidence of TBI among men. TBI rates in men are higher according to surveillance reports. 42 Mean age in years at the time of the PSG was 41 ± 2 SEM with a median of 42 years. TBI chronicity in days at the time of PSG was 889 ± 300 SEM with a median of 141 days. Glasgow Coma Scale (GCS) was only recorded on 40% of subjects (mean GCS = 8 ± 1 SEM). To determine initial injury severity, additional injury information was obtained from the treating hospital, emergency room, and imaging reports. Only 7% of subjects did not require hospitalization post-TBI, suggesting that the remaining injuries were moderate to severe (Table 1). There were no significant sex differences in age or initial injury severity indicators. Most patients were taking a medication that could potentially have an impact on REM sleep and overall sleep quality (Table 2). No sex differences were observed in medication use.
Demographics
Data are shown as percentage or mean ± standard error of the mean.
PSG, polysomnography; ER, emergency room; ICU, intensive care unit.
Medications During the Sleep Evaluation
Data are shown as percentage of subjects taking the indicating medication.
SSRI, selective serotonin reuptake inhibitor; SARI, serotonin antagonist and reuptake inhibitor.
Functional sex differences during post-acute recovery period
Analysis of medical records revealed significant sex effects in levels of disability, depression, and quality of life during the PSG period. No sex effects were observed for CVLT scores. BDI values in women were indicative of moderate depression. Women also showed more disability, according to the MPAI, particularly in the Ability subscale (Table 3).
Functional Sex Differences
BDI scores (ranging from 0 to 63) and MPAI T scores are shown as mean ± standard error of the mean. Significance is demonstrated by *p < 0.05, **p < 0.005.
BDI, Beck Depression Inventory II; MPAI, Mayo Portland Adaptability Inventory.
Women reported a less desirable quality of life when analyzing scales where a high score indicated better self-reported health (F(1,43) = 20.08, p < 0.0005), as well as those scales where a low score indicated better self-reported health (F(1,43) = 7.88, p < 0.005) (Table 4). There were no between-group sex differences regarding medications taken during the night of the PSG (Table 2).
Sex Differences in Subjective Quality of Life
Neurological Quality of Life T scores are shown as mean ± standard error of the mean. Significance is demonstrated by *p < 0.05, **p < 0.005, ***p < 0.005.
Sex differences in sleep macrostructure
No sex effects were observed for total sleep time (338 min ±12 SEM), sleep latency (21 min ±4 SEM), wakefulness after sleep onset (WASO; 73 min ±4 SEM), and subjective sleepiness according to the Epworth Sleepiness Scale (6 min ±0.1 SEM). Overall, average percent time for sleep stages was: N1 (11 min ±1 SEM); N2 (60 min ±2 SEM); N3 (11 min ±2 SEM); and REM (18 min ±1 SEM). Analysis of sleep stages indicated a higher percent time in REM sleep for men (p < 0.005; Fig. 1A), whereas women showed a tendency to have a higher percent time in N2 (p = 0.08). Men had more periodic limb movements during sleep (PLMS; p < 0.05) and had a higher microarousal index per hour (p < 0.05; Fig. 1B,C). No significant sex differences were observed when analyzing apnea and hypopnea measures.

Sex differences in sleep macrostructure. (
Association between sleep stages and memory
A significant association between percent time in REM and immediate recall for CVLT-List A (trials 1–5) was observed. List A requires the subject to recall a list over five trials. Tukey's corrected comparison of scores below and above the normative percentage of REM sleep showed a better performance in CVLT-List A in those subjects with High-Range-REM compared to Low-Range-REM (p < 0.05). This was supported by a main effect for percentage of REM sleep in CVLT-List A (F(2,31) = 3.4, p < 0.05; Fig. 2A). Simple linear regression revealed that the amount of REM accounted for 13% (F(1,32) = 4.8, p < 0.05) of the variance in immediate recall of CVLT-List A (Fig. 2C).
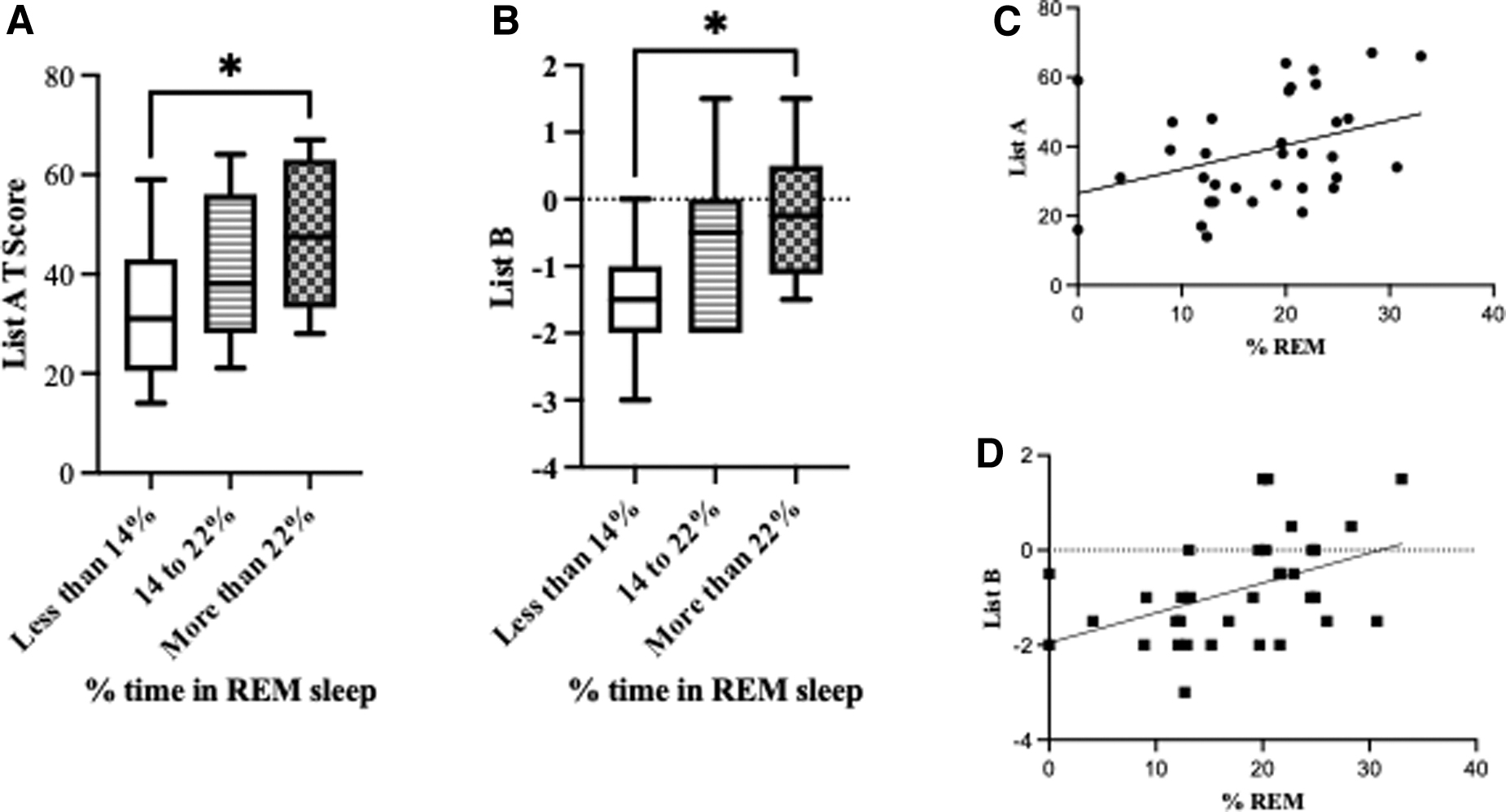
Time spent in REM was associated with performance in the California Verbal Learning Test. (
Likewise, a significant association between percent time in REM and immediate recall for CVLT-List-B was found. List B is an interference list administered immediately after List A that requires the subject to recall after one trial. Tukey's corrected pairwise comparisons showed a better performance in the interference list recall (CVLT-List B) in those subjects with High-Range-REM compared to Low-Range-REM (p < 0.05). This was supported by a main effect for percent REM sleep in CVLT-List B (F(2,31) = 4.1, p < 0.05; Fig. 2B). Simple linear regression revealed that the amount of REM accounted for 20% (F(1,32) = 8.2, p < 0.05) of the variance of CVLT-List B (Fig. 2D).
Low-Range-REM was associated with a higher number of awakenings and WASO% (p < 0.05). This was supported by main effects for Awakenings (F(2,54) = 5.9, p < 0.005) and WASO% (F(2,54) = 3.5, p < 0.05; Fig. 3A,B). Pairwise comparisons also revealed that percent arousal during N2 was higher in those subjects with Low- and Mid-Range-REM compared to those with High-Range-REM (Fig. 3C). This was supported by a significant main effect (F(2,53) = 4.6, p < 0.05). As expected, the percentage of arousals during REM sleep was higher in the High-Range-REM group (p < 0.05), with a significant main effect (F(2,53) = 4.7, p < 0.05; Fig. 3D).

Subjects with <14% REM sleep showed a higher number of (
Impact of medications on REM sleep
Results from logistic regression analysis suggest that the amount of REM sleep is a significant predictor of melatonin utilization, with an odds ratio of 1.08, indicating that for each unit increase in REM sleep, there is an associated increase in the odds of melatonin utilization (Fig. 4A). A significant Z value of 2.01 (p < 0.05) was observed, further demonstrating that the slope of the regression line was significant. Further, the likelihood ratio test resulted in a log-likelihood ratio (G squared) of 4.739 (p < 0.05), indicating a strong association between REM sleep and melatonin utilization. Additionally, the area under the ROC curve was 0.6997, with a 95% confidence interval of 0.55–0.85 (p < 0.05; Fig. 4B). These results suggest a statistically significant association between REM sleep and melatonin utilization.

(
In contrast, lower percent REM time was significantly associated with benzodiazepine use (z value = 2.2, p < 0.05). The odds ratio for this association was 0.8965, indicating a lower likelihood of benzodiazepine use among those with lower percent REM time (Fig. 4C). The log-likelihood ratio was 5.5 (p < 0.05). The area under the curve was 0.7 (95% confidence interval 0.56–0.88, p = 0.05; Fig. 4D). These results suggest that lower percent REM time is associated with lower likelihood of benzodiazepine use.
Discussion
Disruption in sleep architecture is sex dependent
Women reported more depression and poorer quality of life compared to men. Clinician-rated measures also showed that the women in this cohort were more impaired compared to men, particularly in the MPAI ability subscale that focuses on sensory, motor, and cognitive abilities. 43 Depression and anxiety are more frequently found in women.44,45 These findings are in accordance with other studies reporting worse post-traumatic outcomes in women.5,6
Sex differences in neurobiological processes underlying depression and anxiety are likely to impact neuronal networks during sleep.44,46,47 Here, we observed that men spent significantly more time in REM sleep, whereas women spent a significant portion of total sleep time in N2. In contrast with these findings, other PSG studies indicate that healthy non-injured women show more REM sleep duration, as well as better sleep efficiency and longer periods of slow-wave sleep.29,39,48 Thus, in the general population, women seem to have better objective sleep, but more self-reported insomnia compared to men. 28 Comorbidities observed after TBI may be associated with REM alterations. 49 Results from this female cohort reveal more depression and decreased REM sleep. These results contrast with other studies suggesting that increased REM can be a biomarker for depression.50,51 Nevertheless, more recent studies have demonstrated that the link between REM disinhibition and depression is not reliable. 52
Reports of REM sleep post-TBI are mixed with some studies showing decreases in REM sleep,53–55 yet systematic reviews and meta-analyses report a trend for either decreases in REM or no changes in REM post-TBI.56,57 However, to our knowledge, sex was not analyzed as a primary variable in any of these studies. In addition to the potential variability attributed to sex, discrepancies in PSG findings are not surprising given the heterogeneity of TBI, use of medications, and differences in equipment utilized. Pre-clinical studies have found that experimental TBI predominantly increases NREM sleep58–61 and has been found to interfere with enriched environment induced increases in REM sleep. 62 It should be noted that sleep stages in murine models of TBI are usually presented as REM and NREM, with NREM being categorized as a single stage. 22 Sex-dependent effects, such as persistent hypersomnia in females, have also been shown after experimental TBI.63,64
Association between REM sleep and short-term episodic memory
Whereas human and animal studies have shown an increased prevalence of post-traumatic SWDs, the extent to which these disturbances impact chronic outcome remains unclear. Here, we found an association between percent time in REM and better recall scores. Others have observed an association between amount of REM and memory potential. 65 It is widely accepted that both N3 and REM play a critical role in learning memory.16,22,66,67 N3 is characterized by low-frequency, high-amplitude waves and appears to be strongly implicated in cognitive processing. Interestingly, an association between N3 and cognitive function was not observed. It should be noted that the average time spent in N3 was lower than the normative value across all TBI subjects.38,40,41,68
Impact of medications on REM sleep
TBI patients are frequently on several medications that may impact sleep architecture. Most of the study subjects were on antidepressant therapy, of which the majority were taking a selective serotonin reuptake inhibitor (SSRI; 45%), which are known to suppress REM. The duration of treatment was unknown. Despite this, no effects on REM sleep were observed. Effects on REM are maximal early in treatment and diminish significantly over time. 32
Melatonin (nacetyl-5-methoxytryptamine) is widely utilized as an insomnia treatment. 33 Accordingly, melatonin use was registered in 28% of the subjects and was associated with increases in REM sleep duration. The effect of melatonin administration on sleep architecture is equivocal. 69 In accordance with the present described results, others have reported melatonin-associated increases in REM sleep.70,71 Correspondingly, low endogenous melatonin is accompanied by REM sleep reductions. 72 However, other studies show no increases in REM subsequent to melatonin administration.73,74 Effects of melatonin administration are complex because of extrinsic variables, such as time of administration and duration of treatment, as well as intrinsic variables, such as differential and dynamic properties of melatonin receptors.75,76 This is further complicated by the impact that TBI has on melatonin receptors. 77 Clearly, more investigation on the subject is necessary.
Use of benzodiazepines was reported in 16% of the study cohort and was associated with significantly reduced percent time in REM sleep. Benzodiazepine use has also been associated with REM and slow wave sleep reductions in healthy volunteers.78,79
Limitations
Results from this study were based on clinical recordings from single-night PSGs, bringing the potential impact of first night effect (FNE) on the data collected. Considering the potential impact of FNE on REM sleep, 80 it is possible that this effect contributed to the sex differences observed in REM. However, this explanation is made less likely when we consider that there were no observed sex differences in total sleep time.
Whereas we can contemplate the possibility that decreases in REM sleep contributed to the cognitive performance in this cohort of women, because of logistical reasons, we did not have the statistical power to make conclusive claims regarding the impact of REM on verbal memory utilizing sex as a biological variable. Likewise, we did not have the statistical power to determine the impact of medications on REM duration. However, it seems unlikely that elevated REM sleep in men was attributable to medication use, given that no sex effects were observed for melatonin or benzodiazepine utilization. In addition, menstrual cycle stage was not recorded at the time of the PSG. Considering that REM is impacted by changes in the menstrual cycle,81,82 it is possible that the observed sex differences are, at least in part, attributable to menstrual cycle stage.
Conclusion
Findings from this observational study support the hypothesis that decreases in REM sleep may contribute to chronic disability. Results also indicate a sex-dependent decrease in REM sleep that may contribute to disparities in post-TBI outcome. It is becoming increasingly evident that sex provides insight on sleep pathophysiology after injury and more research is necessary, given the notable scarcity of sleep studies focusing on sex differences post-TBI. A better understanding of how changes in sleep impact outcome potential will be useful in defining targeted interventions.
Footnotes
Acknowledgments
Special thanks to Stephanie E. Robinson, RPSGT, Giuliana Cumpa, and Kevin Randle for their contributions to the research and data collection.
The article is not to be considered for CME credit.
Authors' Contributions
All listed authors participated meaningfully in this study and approved the submission of the manuscript.
Stefanie N. Howell: conceptualization, methodology, formal analysis, investigation, writing–original draft, project administration. Grace S. Griesbach: conceptualization, methodology, formal analysis, investigation, writing–review and editing, supervision, funding acquisition.
Funding Information
Financial support for this study was provided by the Centre for Neuro Skills.
Author Disclosure Statement
No competing financial interests exist.