
Abstract
Post-traumatic stress disorder (PTSD) is a common condition in post-deployment service members (SM). SMs of the conflicts in Iraq and Afghanistan also frequently experience traumatic brain injury (TBI) and exposure to blasts during deployments. This study evaluated the effect of these conditions and experiences on functional brain connectomes in post-deployment, combat-exposed veterans. Functional brain connectomes were created using 5-min resting-state magnetoencephalography data. Well-established clinical interviews determined current PTSD diagnosis, as well as deployment-acquired mild TBI and history of exposure to blast. Linear regression examined the effect of these conditions on functional brain connectomes beyond covariates. There were significant interactions between blast-related mild TBI and PTSD after correction for multiple comparisons including number of nodes (non-standardized parameter estimate [PE] = -12.47), average degree (PE = 0.05), and connection strength (PE = 0.05). A main effect of blast-related mild TBI was observed on the threshold level. These results demonstrate a distinct functional connectome presentation associated with the presence of both blast-related mild TBI and PTSD. These findings suggest the possibility that blast-related mild TBI alterations in functional brain connectomes affect the presentation or progression of recovery from PTSD. The current results offer mixed support for hyper-connectivity in the chronic phase of deployment TBI.
Introduction
Mild traumatic brain injury (TBI) and post-traumatic stress disorder (PTSD) are common conditions among Iraq and Afghanistan veterans. 1 -3 Both conditions are associated with neurological alterations; however, these alterations present in different ways. PTSD is typically associated with altered brain structure and function in stereotypical areas (e.g., hippocampus, amygdala, anterior cingulate cortex), 4 -6 whereas diffuse heterogeneous alterations are more typical in mild TBI. 7,8 Many service members also have been exposed to blasts, most of which do not result in TBI. 9,10 Emerging literature suggests blast affects the brain independently of PTSD or TBI. 11,12 Graph theory and network analysis offer a robust platform sensitive to the wide array of effects on brain function associated with these conditions. 13
The human connectome is a model of the structural connections across the brain. 14 Functional connectivity represents communication across the connectome based on statistical dependencies in functional neuroimaging data. 15,16 This can be separated into subnetworks 17,18 such as the default mode (DMN) 19 and salience networks, 20 or studied at the broader level of the functional connectome. 21 Graph theoretic approaches allow the calculation of metrics to describe the communication, topology, and structure of the functional connectome and subnetworks. 22
Magnetoencephalography (MEG) has been utilized to evaluate the effect of PTSD and/or mild TBI on the functional connectome. Reduced local efficiency in brain regions associated with the DMN was identified in civilians with mild TBI. 23 Two studies identified increases in small-worldness and clustering coefficient associated with TBI history and decreases in these metrics associated with PTSD in post-deployment Iraq and Afghanistan war veterans. 24,25 Small-worldness is a network architecture that has high levels of subgroup clustering simultaneous with short path lengths. 26 Findings across studies are not consistent; however, differences in time since injury and sample populations may explain these discrepancies.
Studies using functional magnetic resonance imaging (fMRI) to examine functional connectomes have also produced mixed results. Higher modularity and a significant reduction in between-module connectivity was associated with mild TBI history in a sample of active duty military personnel. 27 In contrast, a reduction in modularity was observed in a civilian sample with mild TBI history and current post-concussive symptoms. 28 PTSD was associated with higher levels of clustering coefficient, global efficiency, local efficiency, and lower values of characteristic path length in a civilian sample. 29 Further, TBI has been shown to moderate the relationship between graph-metrics of specific brain regions and re-experiencing symptoms in post-deployment veterans. 30 Mild TBI and PTSD also have been shown to have unique effects on specific aspects of whole-brain networks, including the fronto-subcortical-parietal pathway and medial prefrontal regions. 31 Similar to MEG studies, these findings lack consistency. There is significant variability in both the methods and sample characteristics (e.g., time since injury) across these studies, likely contributing to the variability in findings.
Other work evaluating strength of and changes to connectivity between specific brain regions suggest that TBI results in hyper-connectivity instead of disrupting or diminishing connectivity. 32 MEG has been utilized to demonstrate support of the hyper-connectivity hypothesis in mild TBI, including reports of increased connection strength in several frequency ranges in the DMN, 33,34 as well as the Rich Club. 35 Although most studies have demonstrated decreased levels of connectivity in PTSD, 36 –41 some have reported increased connectivity. 42 -44 Studies evaluating effects of blast (rather than blast-induced TBI), demonstrate reductions in connectivity. 11,45 These findings establish significant differences in the effects of blast, mild TBI, and PTSD on functional connectivity within the brain.
Results describing the effect of TBI and PTSD on the strength of connectivity are relatively cohesive; however, those describing the effect of TBI and PTSD on the organization and topology of the functional connectome are mixed. This is potentially a result of studies varying by sample population (e.g., civilian, veteran, mixed severities), time since injury, methods utilized, and the imaging technology. 23,24,27,28,31,46 The current study sought to determine the effect of mild TBI and PTSD on the functional connectome of combat exposed veterans of the recent wars in Iraq and Afghanistan using the same methods applied in two prior studies of this population. 24,25 Based on previous work, we anticipated observing increased connection strength associated with TBI and decreased connection strength associated with both PTSD and blast. We also anticipated mild TBI would be associated with increased levels of organization (e.g., higher clustering coefficient, increased modularity), whereas PTSD would be associated with lower levels of organization (e.g., lower levels of clustering coefficient, decreased modularity).
Methods
This project was reviewed and approved by the Institutional Review Board at the W. G. (Bill) Hefner VA Healthcare System in Salisbury, North Carolina. The welfare and privacy of human subjects were protected. Participants voluntarily provided verbal and written informed consent prior to study activities.
Participants
Data were collected as part of the Chronic Effects of Neurotrauma Consortium (CENC) Study. 34 Eligibility criteria were at least one combat deployment in support of the wars in Iraq and/or Afghanistan, combat exposure, English speaking, 18 years of age or older, and able to provide informed consent. Exclusion criteria were as follows: history of moderate or severe TBI; TBI history outside of deployment involving loss of consciousness; neurological disorder; severe mental illness (e.g., schizophrenia or bipolar disorder); current substance use disorder; current psychotic symptoms; or contraindication for neuroimaging. Following the screening visit, participants were also excluded if they failed symptom validity testing (Structured Inventory of Malingered Symptoms) 47 or performance validity testing (Medical Symptom Validity Test 48 ; b test 49 ). MEG data for 16 participants were reported previously. 25
Of the 201 participants who completed neuroimaging, usable data for both MEG and MRI were acquired for 181 (did not provide MRI, n = 6; did not provide MEG, n = 7; data quality issues such as excessive motion, artifacts, n = 7). The final sample size for analyses was N = 181.
Measures
The Clinician Administered PTSD Scale 550 determined presence or absence of lifetime and current PTSD. The Mid-Atlantic Mental Illness Research, Education, and Clinical Center Assessment of Traumatic Brain Injury 51 identified history of deployment-acquired TBI, as well as further characterizing injuries as blast-related or not. The Salisbury Blast Interview 9 characterized blast events across the lifespan. Because no widely accepted definition of blast exposure exists, the frequency (number of blasts involving a pressure gradient) and severity (highest pressure gradient reported) of blast events were utilized for analyses. The Test of Premorbid Function 52 estimated demographically-adjusted pre-morbid intelligence quotient (IQ). Patient characteristics and demographics were obtained using a structured interview.
Magnetoencephalography recordings
Data were acquired using a whole–head CTF Systems Inc. MEG 2005 neuromagnetometer system equipped with 275 first-order axial gradiometer coils. Head localization was achieved using a conventional three-point fiducial system. Resting-state recording was conducted with the participant seated upright, sitting quietly, with eyes open for 5 min. Data were sampled at 1200 Hz over a DC-300 Hz bandwidth and pre-processed using synthetic third order gradient balancing, whole–trial DC offsetting, and band pass filtering from DC-80 Hz with a 60 Hz notch filter. Data were visually inspected for obvious muscle artifact, and such epochs were discarded from further analyses. Following MEG recording, a T1 weighted MRI scan was obtained for each participant for co-registration and source localization.
Connectomes
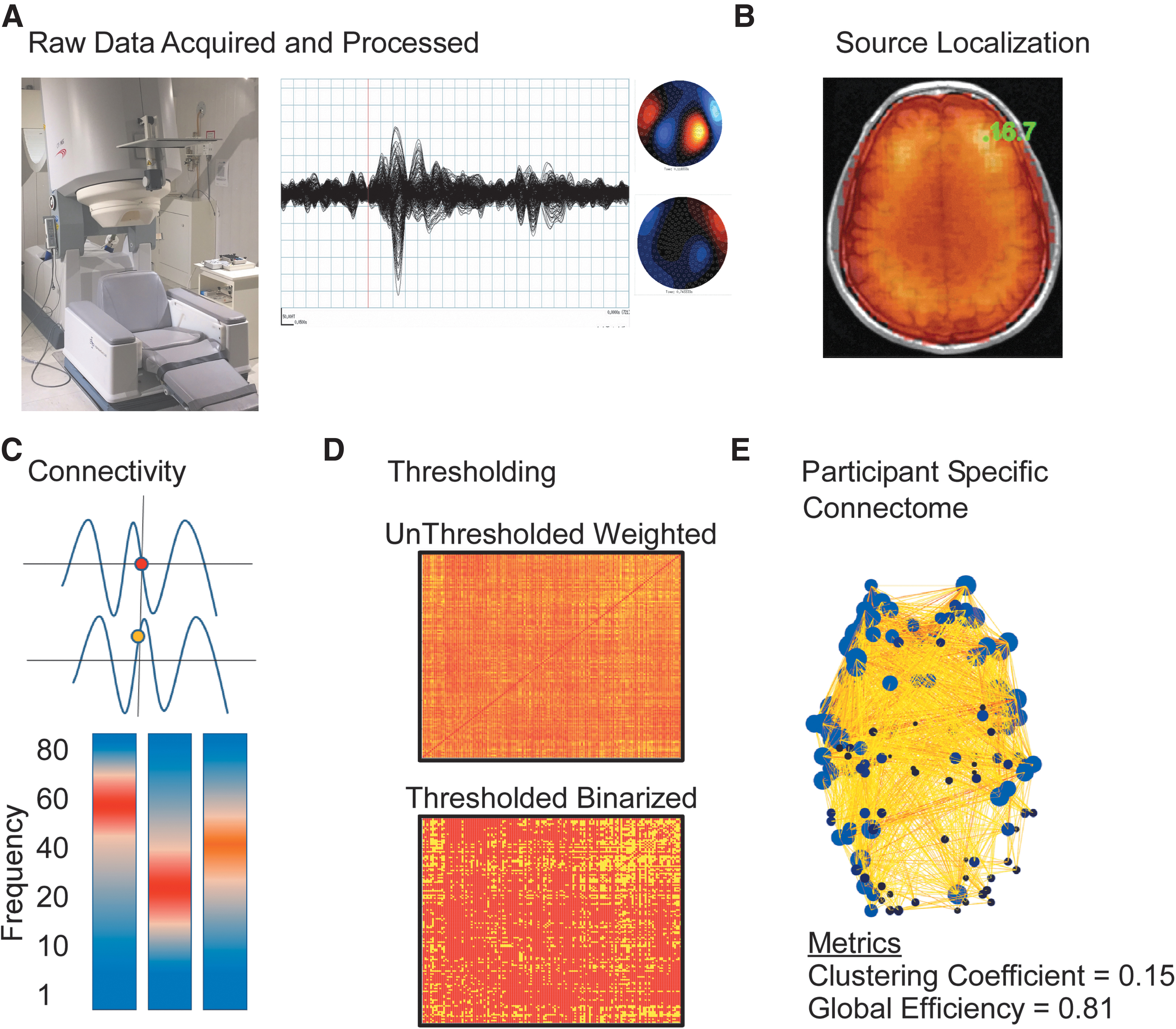
Data processing has been described previously. 24,25 As illustrated in Figure 1, connectomes were created by identifying areas of brain activity, then quantifying communication among those areas. Graph theory was applied to resulting adjacency matrices producing metrics describing characteristics of the functional connectome.
Data processing. Data acquisition
Node identification
Nodes (areas of significant brain activity) were identified by applying a well-validated beamformer, synthetic aperture magnetometry (SAM 53,54 ; voxel size of 5 × 5 × 5 mm, lead fields for equivalent current dipoles, maximizing noise-normalized power) using a three-spherical shell, multiple local spheres head model 55 based on each participant's MRI in the following frequency ranges: delta (1-4 Hz), theta (4-8 Hz), alpha (8-13 Hz), beta (13-30 Hz), gamma (30-80 Hz), and 1-80 Hz. Nodes were combined across frequency ranges to create a single connectome for each participant. Using signal power (SAM) to identify nodes and then estimating connectivity utilizing a phase-based metric helps avoid issues of circularity in analyses.
Estimating functional connectivity between nodes
Source-series were calculated for each node representing the unique weighted sum of the output across all MEG sensors for a specific location in the brain across the 5-min scan. 53,54 The weighted phase lag index (wPLI) 16 was calculated between all pairs of source-series from 1-80 Hz. A surrogate distribution of connectivity data was created for each participant using 5000 pairs of phase-randomized source-series calculated from that participant's data. 56 For each node pair, connectivity was operationalized at the frequency with the greatest difference (using standard deviations [SDs]) in wPLI between the real and surrogate data. To ensure connectivity exceeded that expected in noise, node pairs with real-surrogate connection differences <2.5 SD were labeled as unconnected. The resulting connectomes were then binarized and thresholded to achieve appropriate levels of sparsity by satisfying the equation S = log(N)/log(K), where N represents the number of nodes in the network and K the average degree using S = 2.5. 57
Metrics
Clustering Coefficient 58 indicates how likely the neighbors of a node are to also be connected with one another. Global Efficiency indicates the efficiency of information transfer within the connectome. Modularity 59 indicates how many cohesive subnetworks can be identified within the larger network. Following the recommendations of the Brain Connectivity Toolbox, 60 the analysis was conducted 500 times, using the average Q (Modularity) and average number of modules (Number Modules) as outcome variables. K-core Degree and K-core Nodes were calculated at the maximum K-core Value 61 of the network. The Rich Club is a subset of highly connected and interconnected nodes forming the basis of the broader network. Rich Club metrics were calculated 62 using 500 independently generated random networks. The number of nodes (Rich Club Nodes) within the Rich Club, the minimum degree of those nodes (Rich Club Degree), and interconnectivity among those nodes (Rich Club Coefficient) were used as outcome variables. The number of connections falling within canonical frequency bands was calculated (Delta Connections, Theta Connections, Alpha Connections, Beta Connections, Gamma Connections). Other metrics included the average strength of connections within the network (Connection Strength), average frequency at which connections occur (Average Frequency), mode frequency at which connections occur (Mode Frequency), number of nodes within the network (Nodes), and the minimum threshold level across connections (Minimum Threshold). Connectome metrics have been shown to have test–retest reliability in the good to excellent range depending on variables such as the inter-scan interval, the duration of scan, the functional connectivity metric, and the frequency band examined. 63 –66
Materials
Beamforming and source series construction were completed using software provided by CTF MEG International Services LP (Coquitlam, BC, Canada). Further analyses of source series data were conducted using Matlab 2016a (Mathworks Inc., Natick, MA). Metrics were calculated using the Brain Connectivity Toolbox (Rubinov and Sporns, 2010). Statistical analyses were conducted in SAS Enterprise Guide version 7.1 (SAS Institute Inc., Cary, NC).
Statistical analysis
Linear regression evaluated the associations between PTSD, deployment-acquired mild TBI, blast frequency and pressure, and connectome topology. Correlations among connectome metrics, demographic characteristics, and other potential variables of interest were examined to identify appropriate covariates. Age, sex, minority status, and time since the most recent deployment-acquired mild TBI were identified as relevant covariates. Time since most recent deployment-acquired mild TBI was imputed with the time since most recent deployment for individuals without a history of deployment-acquired mild TBI (n = 107). Results using this variable were drastically different than using time since most recent deployment for all participants. Prior work has demonstrated that the number of nodes within a network can influence metrics describing the topology. 67 To address this issue the current analysis included the number of nodes within each connectome as a covariate (except for the model predicting the number of nodes).
Categorical variables indicating the presence or absence of current PTSD, blast-related deployment-acquired mild TBI, non-blast-related deployment-acquired mild TBI, and the interaction between PTSD and the mild TBI variables were included in the models after covariates (Table 3). To further explore the role of blast two additional models were evaluated (Tables 4 and 5). Both models included categorical variables indicating the presence or absence of current PTSD and deployment-acquired mild TBI as well as their interaction in addition to covariates. The first model included the frequency of blasts during which a pressure gradient was experienced and the second included the maximum pressure gradient reported across all blast events. The interaction between deployment-acquired mild TBI and each respective blast variable was also included. An alternate model classified participants as current PTSD, lifetime PTSD (no longer meeting diagnostic criteria), and never diagnosed. Two indicator variables described the presence or absence of current and lifetime PTSD. False discovery rate 68 was applied at the model level (number of tests = 20) to correct for multiple comparisons.
Results
Participant characteristics are reported in Table 1. There were no significant group differences on any demographic or characteristic variables. Participants with deployment-acquired TBI were significantly more likely to have a current (χ2 (1) = 4.27, p = 0.039) or lifetime, (χ2 (1) = 6.45, p = 0.01) diagnosis of PTSD (groups are mutually exclusive).
Descriptive Statistics of Characterizing Variables
Values are presented as mean (standard deviation) unless otherwise indicated.
N = 181.
PTSD, post-traumatic stress disorder; TBI, traumatic brain injury; IQ, intelligence quotient.
Correlations among connectome metrics are presented in Table 2. Table 3 presents connectome metrics significantly predicted by the model after false discovery rate correction that also included significant effects of non-demographic variables. Interaction effects are depicted in Figure 2. These results demonstrate that blast-related deployment-acquired mild TBI has a much stronger relationship to aspects of the connectome than non-blast related events. The time since the most recent injury was also related to several aspects of the connectome.
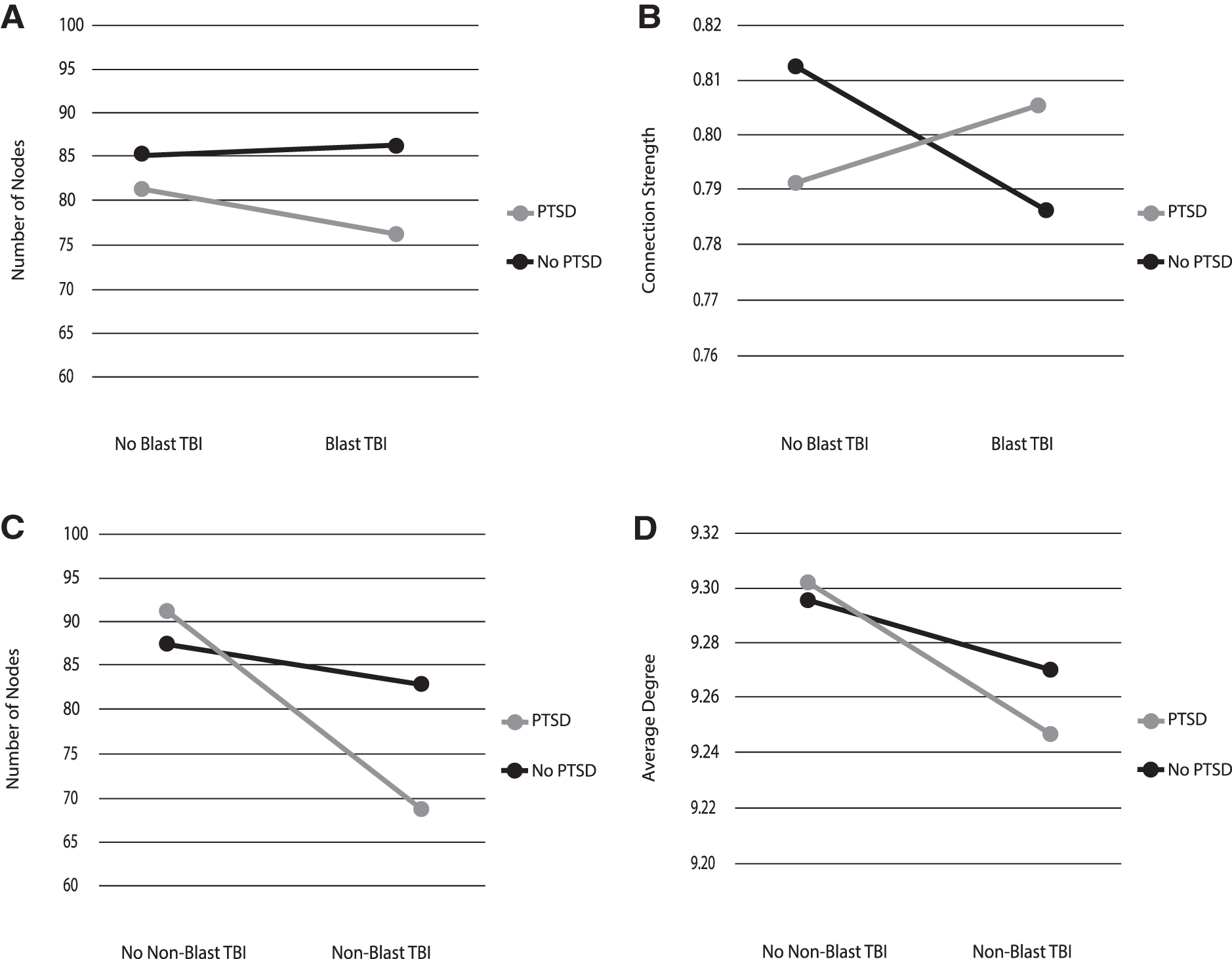
Interactions of post-traumatic stress disorder (PTSD) with Blast and non-Blast traumatic brain injury (TBI). These interactions generally followed the same pattern with the exception of connection strength. This figure presents least squared means, adjusted for all variables in the model, including covariates.
Correlations among Connectome Metrics for the Full Sample
N = 181; * p < 0.05 uncorrected.
Parameter Estimates for Connectome Metrics Significantly Predicted by the Model including Blast and Non-Blast Deployment TBI
N = 181.
Parameter estimate significant at p < 0.05.
Parameter estimates are not standardized. Models presented are significant following false discovery rate correction at p < 0.05.
PTSD, post-traumatic stress disorder; TBI, traumatic brain injury.
Tables 4 and 5 present connectome metrics significantly associated with blast characteristic (frequency and severity) models. The severity of blast exposures was not significantly associated with connectome metrics. The frequency of blast exposures was significantly associated with the number of connections occurring in the theta bandwidth, but no other aspects of the connectome. Neither the frequency nor the severity of blast exposures interacted with deployment-acquired mild TBI to predict connectome characteristics.
Outcomes remained consistent when the models were altered to include lifetime PTSD diagnosis and its interaction with deployment-acquired TBI. The expanded model was significantly associated with the same connectome metrics; however, parameter estimates for the lifetime PTSD variable were not significant for any of those models.
Parameter Estimates for Connectome Metrics Significantly Predicted by the Model including Blast Exposure Frequency, Corrected for Multiple Comparisons
N = 181. Parameter estimates are not standardized. Models presented are significant following false discovery rate correction at p < 0.05.
Parameter estimate significant at p < 0.05.
PTSD, post-traumatic stress disorder; TBI, traumatic brain injury.
Parameter Estimates for Connectome Metrics Significantly Predicted by the Model including Blast Exposure Severity, Corrected for Multiple Comparisons
N = 181. Parameter estimates are not standardized.
Significant following false discovery rate correction at p < 0.05.
PTSD, posttraumatic stress disorder; TBI, traumatic brain injury.
Discussion
The results of this study demonstrate significant alterations to resting-state functional brain connectomes of combat veterans related to current PTSD, blast-related deployment-acquired mild TBI (blast TBI), and the duration of time since the most recent TBI occurring an average of 11 years since the most recent injury. The initial model demonstrates an interaction between PTSD and blast TBI that reduces the number of nodes present in the connectome, increases the average degree of nodes that are present, and increases the strength of connections within the connectome. PTSD also interacted with non-blast related deployment-acquired mild TBI (non-blast TBI) to reduce the number of nodes present in the connectome. Blast TBI demonstrated an independent effect reducing the thresholding level of connectomes. Finally, the time since most recent TBI was related to several connectome characteristics, including a reduced number of nodes and increased degree of the K-core as well as a lower number of connections in the alpha bandwidth, but higher number in the gamma bandwidth. These results demonstrate the relevance of blast TBI in understanding the effects of PTSD on functional brain connectomes and have implications for understanding the neurobiological contributions to disease presentation.
To further explore the effect of blast on functional outcomes, specific blast characteristics were examined. These analyses revealed a single main effect of blast exposure frequency on the number of connections in the theta bandwidth. There were no effects of blast severity and no interactions between these blast characteristics and deployment-acquired mild TBI on connectome metrics. This suggests that the simultaneous occurrence of blast exposure and TBI is necessary to observe changes to the functional connectome well into the chronic stage. Examining characteristics of blast exposure outside the context of TBI may not be as relevant for understanding the connectome during this timeframe.
Evidence strongly supports deployment-acquired mild TBI as a risk factor for the subsequent development of PTSD. 69,70 The current findings demonstrate that the neurophysiological presentation of PTSD differs substantially across the presence and absence of deployment-acquired TBI history, especially in the presence of blast as a mechanism of injury. This is consistent with other studies 71 -73 and raises the possibility that deployment-acquired mild TBI-induced changes in neurophysiological function may contribute to the development of symptoms of PTSD or may increase the risk of developing PTSD. Though the mechanisms through which deployment-acquired mild TBI conveys increased risk for PTSD are unclear, the changes to the functional connectome observed here may suggest one such mechanism. It should also be noted that the relationship between organization of the functional connectome with functional outcomes likely follows an inverse “U” rule, such that too little (e.g., complete randomness) or too much (e.g., complete lattice-like structure) organization results in impaired function and negative outcomes.
The observed differences in the underlying functional connectome across PTSD with and without deployment-acquired mild TBI history may have implications for the course of the disorder as well as response to treatment. For example, symptom severity is typically higher for individuals with comorbid PTSD and deployment-acquired mild TBI. 74 The comorbidity has also been associated with worse behavioral health outcomes and cognitive functioning. 75 –78 Less work has examined the effect of TBI on response to treatment for PTSD, with results suggesting that individuals with the comorbid presentation respond well to standard PTSD treatment modalities 79,80 ; however, they may respond more slowly. 81 Effects of a historical diagnosis (lifetime) of PTSD were not observed in the current study. This suggests the observed alterations do not represent pre-existing risk factors for the development of PTSD. This is in contrast to many structural differences associated with PTSD, such as differences in hippocampal volume 6,82 that have been suggested to be pre-morbid and represent risk factors for the development of the disorder. As such, the current findings hold potential diagnostic value and may serve as effective endpoints when studying interventions for comorbid PTSD and mild TBI.
The current results offer mixed support for the presence of hyperconnectivity. Although the interaction between PTSD and blast TBI was associated with increased connection strength, the main effect of blast TBI was associated with reduced connection strength. Prior MEG findings have supported the hyperconnectivity hypothesis, reporting increased strength of connectivity associated with specific frequency ranges. 33 -35 Two of these studies were conducted in the acute time frame following TBI (less than 3 months 33 and less than <24 h 35 ) and in the third, participants were an average of 16.7 months (SD = 19.7) post-injury. 34 The current study was conducted an average of 11 years post-injury. Together with the current findings, this literature suggests TBI-associated hyperconnectivity occurs primarily in the acute stage. Without longitudinal data it is not possible to reach conclusions regarding the progression of altered brain function; however, it is possible that the acute and chronic neurophysiological profiles of TBI are different, similar to symptom presentation in these time frames. This is supported by the significant effect of the time since most recent TBI on several aspects of the connectome in the current results. Prior studies did not report analyses of graph metrics so it is unclear if the alterations observed in the current study may have been present in the acute state and failed to resolve during the progression to the chronic stage. Alternatively, changes could have manifested at a later point as part of the resolution of differences in connection strength observed in the acute stage.
Limitations to this study include a lack of longitudinal data and retrospective recall of events. This approach to connectome creation focuses on areas of the brain active at rest. This differs from atlas-based approaches by creating a unique functional connectome for each participant. Benefits of this approach include identification of unique patterns of brain activity for each individual, potentially capturing the effect of compensatory mechanisms or specific injury mechanisms. This is important in the study of a heterogenous condition like mild TBI. Limitations of this approach include the inability to identify areas inactive across conditions. Methodological variability is a weakness of the broader literature. The current study is methodologically consistent with our prior work, but not completely consistent with the work of other groups. This study also has several strengths. The sample size is twice that of previous studies using MEG in this population. The study utilized well-validated interviews to determine TBI history, PTSD diagnosis, and characterize blast exposure rather than self-report measures. Participant presentation was screened using validity measures to ensure symptom exaggeration and fabrication were not present.
Conclusions
The current study characterized the effect of common post-deployment conditions including PTSD, deployment-acquired mild TBI, and blast history on the resting-state functional connectome. Results demonstrated interactive effects of PTSD and blast-related deployment-acquired TBI producing a reduced number of nodes, increased average degree, increased connection strength, and a higher threshold for inclusion of connections in the connectome. These results identify distinct neurophysiological profiles based on the presence of PTSD and blast-related deployment-acquired mild TBI that hold potential diagnostic value.
Footnotes
Acknowledgments
The authors would like to thank the veterans and service members who contributed their time and effort. We would also like to thank Mary Peoples, David J. Curry, MSW, Christine Sortino, MS, and Alana M. Higgins, MA, for their contributions.
The views, opinions and/or findings contained in this article are those of the authors and do not necessarily reflect the views of the US Government, the US Department of Veterans Affairs, or the Department of Defense, and should not be construed as an official position, policy or decision, unless so designated by other official documentation.
Funding Information
This work was supported by funding from Department of Defense, Chronic Effects of Neurotrauma Consortium (CENC) Award W81XWH-13-2-0095 and Department of Veterans Affairs CENC Award I01 CX001135, NIAAA R01 AA016852 (DWG), Wake Forest Clinical Translational Science Institute (UL1TR001420), Wake Forest Translational Alcohol Research Center (P50 AA023117). This research was supported by the Salisbury VA Medical Center, Mid-Atlantic (VISN 6) Mental Illness Research, Education, and Clinical Center (MIRECC), and the Department of Veterans Affairs Office of Academic Affiliations Advanced Program in Mental Illness, Research, and Treatment.
Author Disclosure Statement
No competing financial interests exist.