
Abstract
Spinal cord injury (SCI) is a chronic condition that results in high healthcare utilization and lifetime cost across the care continuum. In the absence of a standardized model of care delivery for SCI in western countries such as Canada, a scoping review of the literature was performed to identify and summarize existing international SCI models of care delivery. Four databases were searched using key words and subject headings for concepts such as: “spinal cord injury,” “delivery of healthcare,” “model of care,” “patient care planning,” and “care pathway.” Title, abstract, and full text review were competed by two independent reviewers. A combined total of 46 peer-reviewed and gray literature articles were included. No single SCI model of care has been adopted across different countries internationally. However, optimal attributes of models of care were identified, including the importance of having multidisciplinary SCI specialty care providers along the continuum, provision of rural SCI services and outreach, integration of primary care, peer mentoring, and using a hub and spokes model of care. These findings inform the future development of an SCI model of care, which ideally would serve all geographical locations and span the continuum of care, improving the health status and quality of life of persons with SCI.
Introduction
Spinal Cord Injury (SCI) is one of the most devastating conditions affecting a person's physical, psychological, and social well-being. Based on a national prevalence estimate completed in 2010, there were approximately 86,000 persons living with SCI in Canada. 1 The annual combined incidence rate of traumatic SCI (TSCI) and non-traumatic SCI (NTSCI) in Canada was estimated to be 3675. 1 Global prevalence of TSCI was reported to be between 236.0 and 1298.0 per million, while the incidence was between 8.0 to 246.0 cases per million. 2 Despite the relatively low incidence, direct and indirect costs for SCI care are disproportionately high, largely due to the fact that SCI affects multiple organ systems acutely and chronically. The lifetime financial direct and indirect costs in Canada per individual was estimated to be $1.5 million for paraplegia and $3.0 million for tetraplegia in 2011 Canadian dollars. 2 The annual direct and indirect costs of new TSCI cases in Canada were estimated to be $2.67 billion. 2 In the United States, SCI was documented in a U.S. Veterans Affairs report as the most expensive chronic disease per capita of 29 chronic conditions, with an average annual cost of $26,735 per patient in fiscal year 1999, compared with renal failure ($22,656), stroke ($14,482), and chronic obstructive pulmonary disorder ($10,618). 3 Therefore, the healthcare utilization and the lifetime cost of persons with SCI are high across the care continuum (from acute management to rehabilitation to community reintegration). Given the high cost of care, it is imperative that an effective care delivery model for SCI, as well as the systematic evaluation of interventions and care outcomes, be designed and implemented. 4
Although accreditation standards for facilities providing acute and rehabilitation SCI care, clinical practice guidelines for SCI care, and SCI research evidence to guide care are available in Canada, there is an absence of a standardized model of SCI care at the provincial, federal, or international level to outline how healthcare services are delivered. 5 –8 Challenges with the transition between acute, rehabilitation and community care also exist. 9 While SCI needs within the community and across the care continuum following rehabilitation, have been documented, the complex needs of persons with SCI throughout their lifetime at all points of care are not well understood. 9,10 A standardized model of care for SCI would describe the care and services individuals with SCI require throughout the SCI continuum and how they are structured and implemented to ensure they receive “the right care, at the right time, by the right team and in the right place.” 11
To develop a standardized SCI model, there is a need to understand what is known internationally about models of care delivery for SCI, including the optimal attributes of how SCI care is delivered and their effectiveness. A scoping review was selected to identify existing international models of care delivery for SCI, which may be applied in other health jurisdictions. The objective of this scoping review was to determine how SCI services are delivered around the world, in particular during the rehabilitation and life-long phases of the care continuum. We aimed to identify and summarize models of rehabilitation, community, and life-long SCI care delivery, and thereafter identify current strengths and opportunities of improvement in the SCI continuum of care. Improvements to delivery of care for SCI has the potential to enhance patient outcomes by providing clinicians and healthcare administrators with the attributes of ideal or optimal care, in addition to informing policy and future research.
Methods
Study design
A scoping review was selected to inform a broad research question to provide a comprehensive overview of the existing literature on a given topic. 12 It has the advantage over a systematic review to best map the literature that exists on a topic of which not a lot is known. 12,13 Our process was guided by Arksey and O'Malley's framework for conducting scoping reviews. 14,15 The six stages of the framework adhered to were: 1) identify a research question; 2) identify studies relevant to the research question; 3) select relevant studies; 4) extract data from selected studies; 5) combine, summarize, and report the results of the review; and 6) consult with stakeholders. 14,15
Research question and objective
The research question was: What models of service delivery, specific to the rehabilitation and lifelong care of persons with SCI exist internationally? The objective of the scoping review was to describe the types of services and identify how services are delivered to persons with SCI during the rehabilitation and community phases of care around the world.
Search strategy
Search terms were selected based on the literature and clinical expertise. Models of care were defined as pathways by which healthcare services were systematically delivered to persons with SCI. We searched the following databases using subject terms and key words related to models of care for SCI, with all searches limited to articles published between January 1,1995, and January 14, 2020: MEDLINE (via the Ovid platform), EMBASE (via the Ovid platform), CINAHL (via the EBSCO platform), and ProQuest Dissertations and Theses Global. This time frame was chosen so that the literature would be more recent and applicable to the current health systems. The complete MEDLINE search strategy, which was adapted to search the other databases, is reported in Supplementary Appendix A. Since an aim of this paper is to better understand international models of care to inform care in Canada, a gray literature search of countries that were economically similar to Canada was completed. Seventy-nine high-income countries and their associated websites (e.g., government, ministry of health, health authority) were included. A total of ninety-seven government websites were searched using similar search terms identified in Supplementary Appendix SA. Economic income groups of countries were based on the World Bank definition of high-, middle-, and low-income countries. 16 Non-English literature was excluded.
Literature selection
Limits were not placed on the study design; however, at the level of full text review, all included studies were limited to those published in the English language. At least two reviewers screened at the level of title and abstract. Articles included at the level of abstract, as agreed upon by both reviewers, were included for full text review. Any discrepancies in articles included at the level of abstract were discussed until an agreement was reached. Study inclusion at the level of full text was determined upon agreement by two independent reviewers. Any discrepancies were resolved by discussing the article within the context of the inclusion and exclusion criteria (Supplementary Appendix SB) until an agreement was reached. Any disagreements were resolved by consulting with a third reviewer, who is a senior member of the team.
Included studies described how rehabilitative, primary, or community care was delivered in a specific setting, and/or outlined a care delivery pathway or model of care for adults with TSCI or NTSCI at any stage of injury spanning more than one phase of care (e.g., transition from rehabilitation to community). 17 Care delivery pathways focus on interventions that aim to enhance the quality of care across the continuum. 18 Articles that outlined the formation of a care plan, the lifelong management of SCI, community integration tactics, or community mentoring and transition programs in relation to SCI service delivery were included.
Articles that described clinical practices such as clinical care pathways or guidelines were excluded. Clinical care pathways were defined as interventions that were a part of a structured care plan that enacted a guideline, detailed the steps of an action, were criteria-based progression, and/or aimed to standardize care for specific rehabilitation best practices (e.g., respiratory management following SCI). 17
Data extraction
Endnote was used to track peer reviewed literature (title and abstract), while gray literature screening was documented by taking screenshots of website search results. All literature that was included past the point of title and abstract review was reviewed in full text. An Excel spreadsheet was used to enter the data extracted from the peer reviewed and gray literature articles that met the inclusion criteria at full text review. One reviewer compiled and entered data from the included articles into the data extraction spreadsheet, which collected data on whether the article focused on TSCI or NTSCI, the care delivery pathway or model of care identified, the phase or setting (i.e., acute care, inpatient rehabilitation, ambulatory care or community) in which SCI services were delivered, the aim of the article, the population characteristics, and the conclusions.
Results
Study selection
Following the removal of duplicates, a total of 10,085 articles were returned from the peer-reviewed database search. Of the 10,085 articles, 184 were reviewed in full text. A total of 40 peer-reviewed and six gray literature articles were included in the review. Figure 1 illustrates the literature review process from the initial search, through to the final study selection, including gray literature. The majority of articles that were excluded during full text review either did not describe the delivery of care or described the delivery of care during only one phase of care (n = 77), or described a clinical guideline or pathway (n = 41). Of the ninety-seven government websites searched for the gray literature search, a majority of these websites yielded no relevant results (n = 49) or were unavailable in English (n = 32). Other websites were inaccessible or unavailable (n = 4). From the available websites, eight articles were returned and reviewed in full. Two were then found to be not specific to SCI; therefore, six gray literature articles were included.
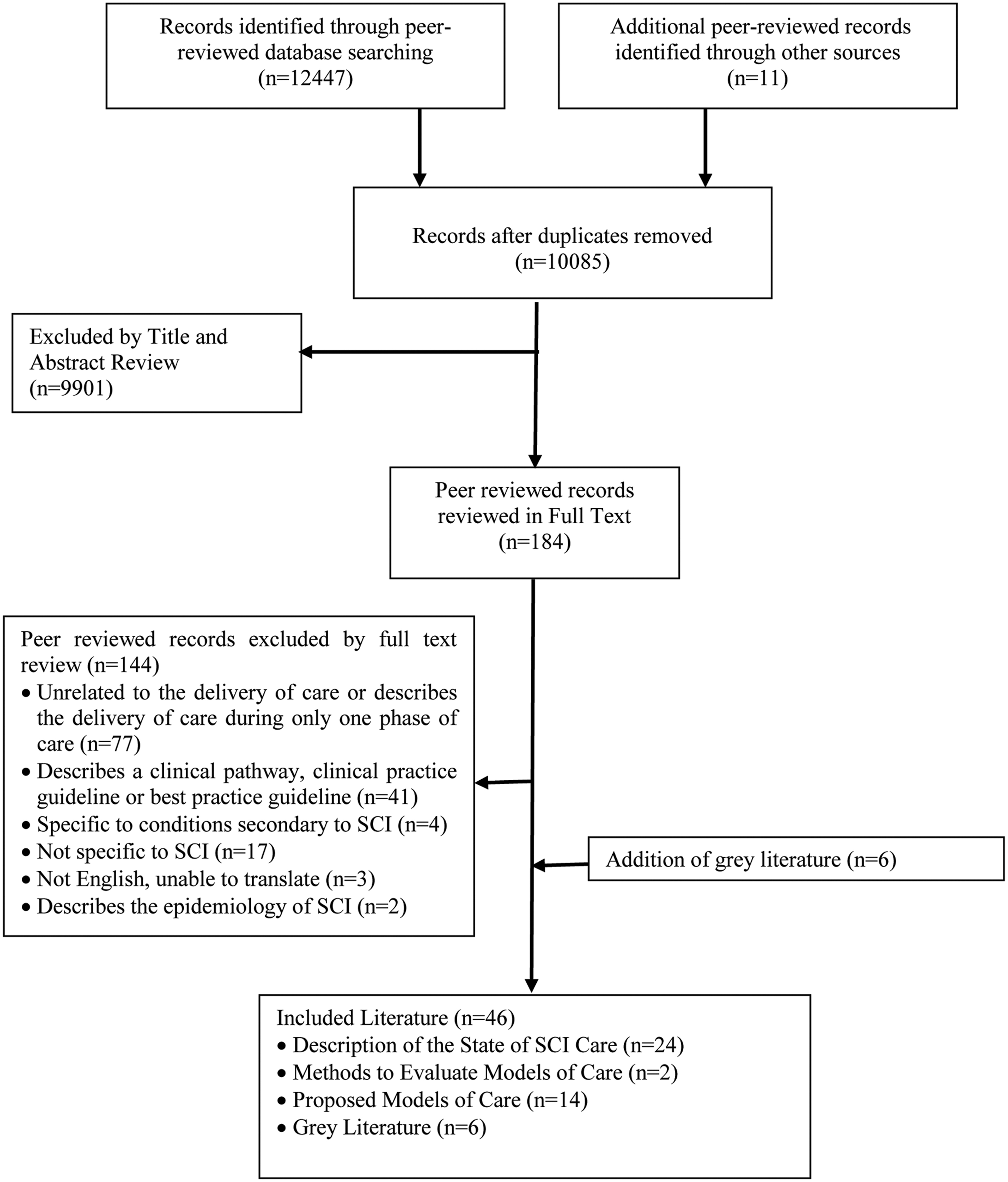
Flow diagram of scoping review process.
Study characteristics
From the included literature, information relevant to the delivery of care for persons with SCI was extracted. As seen in Table 1, the included studies were categorized into four main groups: Descriptions of the State of SCI Care (n = 24), Methods to Evaluate Models of Care (n = 2), Proposed Models of Care (n = 14), and Gray Literature (n = 6), such as the United States Department of Veterans Affairs' Handbook on the SCI and Disorders System of Care. 19 The study aim, setting, population characteristics, services provided, and main study conclusions were summarized (Table 1). The gray literature search yielded varying levels of publicly available general health information and information on models of SCI care. Of the 21 countries identified from the included peer-reviewed and gray literature (Fig. 2), Australia was the most frequently identified country (n = 9, 19.6%) followed by the United States (n = 8, 17.4%), Canada (n = 6, 13.0%), and the Netherlands (n = 3, 6.5%).

World map of the countries searched and identified from the peer-reviewed and gray literature scoping review.
Study Aim, Setting, Population Characteristics, Services Provided, and Conclusions of the Included Peer-Reviewed and Gray Literature
SCI, spinal cord injury; NTSCI, non-traumatic spinal cord injury; N/A, not applicable; ICU, intensive care unit.
Descriptions of the state of SCI care
The International SCI Community Survey articles included in this review were conducted in the following countries: Spain, 20 Italy, 21 Germany, 22 Portugal, 23 Malaysia, 24 Switzerland, 25 Korea, 26 South Africa, 27 Lithuania, 28 Thailand, 29 the Netherlands, 30 Greece, 31 China, 32 United States of America, 33 Norway, 34 Poland, 35 Indonesia, 36 New Zealand, 37 and Israel. 38 By participating in the survey, each country described the epidemiology of SCI, the person with SCI's journey through the continuum of care, living with SCI, the health and rehabilitation system, the state of specialized care, and the societal response to SCI. The main themes identified in these articles included: a desire to understand and improve health and social needs, participation and community reintegration, and the return-to-work process; a need for the development or improvement of vocational rehabilitation; and the absence of specialized units for SCI. More specifically, the health and social needs of persons with SCI were discussed in the majority of the International SCI Community Survey articles. Across these studies, there was a want and a need to improve health and social services that can be accessed by and are delivered to persons with SCI. Participation and community reintegration also was identified as a main theme and an area that requires improvement for persons with SCI.
Some suggestions for improving participation and community reintegration include support provided by social workers or non-profit organizations that focuses on real life situations (finances, leisure, housing, etc.), community care that is specific to those with SCI, and a platform for sharing and exchanging information. The importance of improving the return-to-work process was identified in several of the International SCI Community Survey articles. The main recommendation for improving this process was to develop laws or regulations that facilitate return to work for persons with disabilities. Ultimately, the reports summarized the country's current model of care for persons with SCI, highlighted gaps in the models of care, and provided recommendations for future research or changes to care. 20 –38
The scope of the challenges persons with SCI encounter in accessing timely and appropriate healthcare services, specifically through primary care and challenges with payment for health services in the context of the U.S. were described in one article. 39 Three mutually reinforcing solutions with the potential to better meet the post-rehabilitation needs of persons with SCI included patient education and health behavior change (e.g., self-management and peer support), smoother transitions into community healthcare, and customized care delivery. 39 To meet the post-rehabilitation needs of persons with SCI it was proposed that an integrated system of healthcare that extends into the community and focuses on greater integration during post-rehabilitation care must be developed. 39 Other articles described the role and importance of primary care 40 –43 and the patient-centered medical home concept 44,45 in the delivery of SCI care in the community. Taking a patient-centered delivery of care approach, two articles described patients being active and informed partners in their care planning and independently manage their own care based on their unique needs and individual preferences. 44,45
Methods to evaluate models of care
Two articles outlined methods to evaluate or simulate patient care across the care continuum and described how the impact of interventions or innovations across the continuum of care could be predicted or evaluated before they are implemented. 46,47 Both articles were part of the Access to Care and Timing (ACT) project in Canada, which aimed to model the systems of delivery and simulate, predict, and evaluate interventions. While one article detailed the methodology and implications of simulating care across the continuum in Canada, the other described the value of the simulation tool in decision making.
Current and proposed models of care
Of the included peer-reviewed literature, 14 articles described or proposed models of care for persons with SCI. The different types of models of care included in the scoping review were the: transitional rehabilitation model (n = 2), an independent-living model compared with an agency care model, specialized home-based care, and the inclusion of additional team members such as a liaison nurse and peers as part of the interdisciplinary team.
The two transitional rehabilitation models identified in the review aim to improve continuity of care and service delivery for persons with SCI living in Australia. 48,49 More specifically, the home-based transitional rehabilitation model targets persons with SCI living in rural or regional locations who have been discharged from inpatient rehabilitation, 48 whereas the second transitional rehabilitation model targets persons with SCI during the end stages of primary rehabilitation services transitioning into community-based rehabilitation services. 49 Both of these models use a multidisciplinary team to facilitate the person's transition from inpatient rehabilitation into the community. 48,49
A study conducted in the United States compared two models of long-term care: the independent living model and the agency care model. 50 The independent living model (self-managed care) was developed because persons with disabilities wanted to remove environmental and social barriers in their community; thus, the individual is responsible for recruiting, selecting, managing, directing, and reimbursing their care provider. While within the agency care model, caregiving is delegated to healthcare professionals. When comparing the two different models of long-term personal assistance care, it was found that the group that used self-managed care received more hours of paid assistance and experienced more positive outcomes such as better life satisfaction, better health outcomes, and lower costs. 50 Recognizing the complexity of the medical issues related to SCI, specialized home-based models of care have been reported in order to decrease hospital readmission and emergency department visits, 45 and to allow for early discharge and prevent re-admission. 51
A number of articles have proposed the inclusion of additional team members, such as peer mentors, as part of this multidisciplinary team structure, as evidenced by their benefits. 52 –56 The inclusion of a transmural nurse as a part of the clinical rehabilitation team who acts as a liaison between community-dwelling persons with SCI, primary care professionals, and the rehabilitation center has been described by two articles from the Netherlands. 57,58 This aims to reduce both the number and severity of health problems as well as improve the continuity of care among persons with SCI. 57
Of note, there are several articles describing programs or services that facilitated SCI models of care. Telehealth uses telecommunication technologies to deliver services at a distance. 59 Its use in Australia promotes improved engagement of persons with SCI with local service providers to enhance equity of access and reduce travel for persons living in rural or regional locations. Service providers that delivered tele-healthcare were general practitioners, nurse practitioners, and allied health professionals. The local support model facilitates both communication and coordination between services in order to improve health outcomes. 60 More specifically, it aims to facilitate the development of sustainable spinal networks between rural health professionals and metropolitan specialized SCI services in Australia. The network of persons includes the individual with SCI, their caregivers, and health professionals (e.g., general practitioner).
Gray literature
Through a search of gray literature, six articles were identified for inclusion in the review. These articles provided the most comprehensive descriptions of systems of care for SCI along the continuum, much more so than peer-reviewed literature. They included New Zealand's Spinal Cord Impairment Action Plan, 61 the United States Veteran's Health Administration Directive 1176(2) - Spinal Cord Injury and Disorders System of Care, 19 the Queensland Spinal Cord Injuries Service Model of Care in Australia, 62 the Model of Rehabilitation for Spinal Cord Injury in South Australia, 63 the Spinal Cord Injury Model of Care Diagnostic Report from New South Wales, Australia, 64 and the United Kingdom National Health Service's Spinal Cord Injury Services. 65
New Zealand's Action Plan aims to improve the health outcomes, quality of life, and well-being of persons with SCI, as well as lifetime costs by promoting community participation and independence and supporting the families who assist in caring for persons with SCI. 61 Similarly, the Veteran's Health Administration Handbook 1176(2) (2019) 19 describes the System of Care, which focuses on self-management in order to support, promote and maintain the health, independence, productivity, and quality of life among persons with SCI. The System of Care emphasizes the importance of ongoing communication among providers, rehabilitation, and a comprehensive continuum of care to meet the needs to veterans with SCI. Of note, it integrates primary care into the system of care, which also provides life-long follow-up and specialty care at the SCI centers. 19 The Model of Rehabilitation for Spinal Cord Injury in South Australia aims to develop a model of rehabilitation for persons with SCI that achieves consistency of services across the care continuum, presently and in the future. This model will inform regional implementation planning and optimize patient care. 63
The Queensland Spinal Cord Injuries Services Model of Care (2018) provides comprehensive, patient-centered care, with a unique emphasis on transition from rehabilitation to the community, as well as an active outreach program for people with SCI in rural areas. 62 The United Kingdom National Health Service's Spinal Cord Injury Service provides comprehensive guidelines for the provision of SCI services for adults and children in the eight SCI centers in England. The most noteworthy features of this service include outreach services to newly injured patients with SCI in other settings for clinical assessment, patient and staff support, and also to those in the community. 65 Similar to the United States Veterans Health Administration Spinal Cord Injury System of Care, it provides lifelong follow-up and inpatient specialty services for SCI related complications and conditions. 19
Though the New South Wales State Spinal Cord Injury Model of Care in Australia is currently developing a new model, hence the lack of a published report, it produced a “Diagnostic Report” (2017), 64 which describes the current state and the principles for the new model of care. It also emphasizes the importance of the provision of life-time, comprehensive care.
Discussion
Understanding attributes of successful models of care and lessons learned during model development and implementation can assist countries aiming to improve care delivery. We conducted a scoping review to understand what is known in the literature about models of care for SCI. The 14 articles that described and proposed SCI models of care highlight several benefits, with the core benefits (benefits identified in more than one evaluated model) displayed in Figure 3. With an understanding of existing models of care for SCI, we identified areas that need improvement within the delivery of SCI care across the continuum to create an evidence-based standardized model of care for SCI.
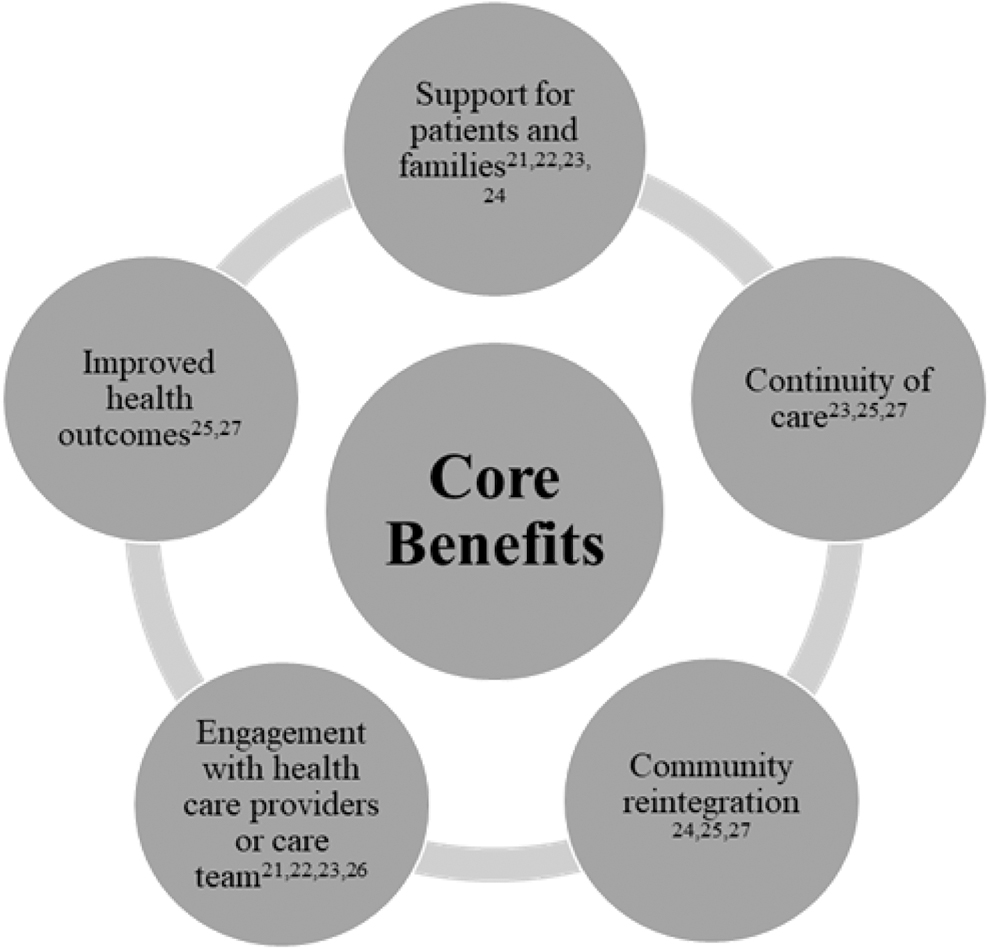
Core benefits identified from the articles describing models of care.
Included literature focused on the delivery of services and/or models of care during the rehabilitation, community, or life-long phases of care. While the lifespan of an individual with SCI approaches that of an individual without SCI, 66 world-wide implementation of SCI-specific care models has the potential to help close this gap.
From the results of this scoping review, there did not appear to be any single model of care for SCI that has been utilized and shared internationally. In fact, the literature that focused on the state of SCI care internationally indicated that there were common challenges and gaps in service delivery for SCI care, especially with care in the rural areas, provision of rehabilitation services in the community, vocational services, and community reintegration, all of which can be affected by payor source. Nevertheless, we were able to identify the following optimal attributes of models of care delivery for SCI that exist internationally:
Importance and composition of multidisciplinary SCI specialty care providers
The returned literature established the importance of an SCI network and specialized SCI services provided by qualified persons in the delivery of care. 57 –60,67 Examples of such included multidisciplinary team involvement, remotely available specialized SCI consultation teams, and the transmural care model in the Netherlands, which utilizes a liaison nurse to offer a number of benefits including support for persons with SCI and families after discharge, support for and communication with primary care professionals and the rehabilitation team, and activities that promote continuity of care and feedback to the care team based on the person's experiences. 57,58 While the concept of having a multidisciplinary team of clinicians in the care delivery for SCI appears to be universally endorsed in the literature, there is also growing evidence that the inclusion of peers as part of the multidisciplinary team for support and mentoring is beneficial and should be considered. 54 Of note, inclusion of peer-mentors in the rehabilitation team is more successful where there is an existing organizational culture and support of patient-centered approach in care. 54 Literature outlining who is involved in the delivery of services, their training and scope will be important in developing models of care.
Provision of ongoing SCI specialty care at the SCI centers
Several systems of care have specified the utilization of SCI centers for the management of secondary complications following SCI (U.S. Veterans Affairs; United Kingdom; Queensland, Australia), so that those requiring complex SCI care needs will be treated where the staff are SCI-trained. While there is no study to verify that this improves the outcomes, it makes intuitive sense, especially from a patient-centered and continuity of care perspective. This requires the establishment of a spinal injury unit or center where the mandate is to provide lifelong care rather than episodic rehabilitative care only. In many SCI programs without such a mandate, this will require a major change in structure and focus of care.
Rural SCI services, transitions, and outreach
The delivery of SCI services to persons in the community requires both specialized SCI services as well as ambulatory service providers and local care providers to have the capacity to deliver SCI services. This is particularly challenging in rural areas. The majority of literature on remote SCI service delivery and outreach originated from the Australian states of Queensland, New South Wales, and South Australia. Australia is a large country with major urban centers and a vast amount of rural and remote areas. The aim of the Australian models is to bridge the gap that exists in service delivery to persons with SCI in rural and remote locations using transitional rehabilitation and telehealth programs to ensure the delivery of rehabilitation and lifelong care services to persons with SCI in the community, and to engage local healthcare providers. 48,59
The transitional rehabilitation program reduces the amount of time spent in hospital, offers education and coordination of local care providers, involves the family in the rehabilitation process, promotes community care by utilizing social supports, provides specialist support and teaches transferrable skills that persons with SCI can utilize in the community. In order to build capacity, local care providers were given the opportunity to ask questions, develop a care and service plan with transitional rehabilitation staff, have telephone contact with transitional rehabilitation services, and receive specialist training and support. 48,49 Services supplemented by telehealth include multidisciplinary Spinal Outreach Team (SPOT) and Spinal Injuries Unit specialist outpatient clinics, which has demonstrated benefits for persons with SCI because it allows for the substitution of face-to-face outpatient appointments with video consultations, promotes engagement with service providers, and reduces the amount of travel, 59 which can be challenging for persons with SCI. As a result, SCI specialty services are made accessible to persons with SCI in the rural areas without long distance travel.
Hub and spokes model of care
In addition to the models of care identified in the peer-reviewed literature, the “hub and spokes” model of care within the U.S. Department of Veterans Affairs SCI System of Care oversees the delivery of care to persons with SCI throughout care networks. It is the largest system of care for SCI in the world, integrating both specialty and primary care for veterans with SCI and disorders, covering the vast geographical areas in the United States. This model is described in the VHA Handbook 1176. 19 outlining the specific roles and organizational requirements of the 24 hubs and their corresponding spoke sites. Emphasis is placed on transition between the hub and spoke sites, as well as lifelong care across the care continuum. Despite its long history and strong reputation, there has not been any published study on its effectiveness.
The role of primary care in SCI management
The importance of primary care integration is highlighted in the United States Department of Veterans Affairs SCI System of Care cited above. There is also growing evidence that primary care in the community can play an important role in providing continuity of care to persons with SCI, especially in conjunction with the SCI specialists. 68 Therefore, the integration of primary care in SCI models of care should be considered and a recent Canadian summit outlined plans to advance primary and community care following SCI. 69
Vocational rehabilitation needs
The International SCI Community Survey has several articles with a common theme – the identification of the support for vocational rehabilitation as a gap for the current SCI models of care. In fact, it is well-known that the return-to-work rate after SCI has been low. 70,71 Therefore, while this has not been identified as an optimal attribute to existing models of care internationally, future development of SCI models of care should include support for vocational rehabilitation as an area of focus.
While they are not directly addressing the SCI model of care, foundational initiatives such as the development and implementation of the Rick Hansen Spinal Cord Injury Registry and the Access to Care and Timing (ACT) project supported by the Praxis Spinal Cord Institute have begun to help develop and implement an optimal care model in Canada. 72 To implement and test the effectiveness of a model of care and transitions between phases of care, appropriate tools and capacity to test, monitor and evaluate an intervention are needed. Articles describing the ACT Simulation Model, which uses Canadian data, may be used in the future to examine methods of service delivery implemented across the care continuum. Such models can inform the development of an effective model of care. 46,47
Future research directions
Given an aging population and an anticipated increase in the prevalence of NTSCI, future consideration such as the inclusion of geriatric expertise in SCI will be needed. 1,73 –75 In this review, there was a lack of models specific to NTSCI identified and future studies should consider additional factors of importance. Future research should also consider the pre-hospital and acute phases of care as well as special populations such as pediatrics transitioning into an adult SCI model of care. Additionally, this review is limited to high-income countries only—future reviews may include the special considerations for low- to middle-income countries.
Limitations
In this scoping review, the quality of the included peer-reviewed and gray literature was not assessed and literature relevant to the research question may have been missed. The methods of service delivery or models of care identified from the literature may not have an identical application in other jurisdictions given the differences in population demographics, healthcare systems, funding models and existing services. Future studies, such as a systematic review with a specific research question informed by the findings of this scoping review, could be completed as a next step in determining the attributes of existing models of care delivery for SCI that may be applicable in different countries. Evidence from existing models of care could inform healthcare accreditation standards for a model of service delivery for SCI, which already exist for TSCI in some countries, but require additional work for NTSCI. In the future, a better understanding of how to develop local, regional and countrywide SCI care delivery models that meet the requirements of all geographical locations, clarify the types of injuries that require specialized care, and the delivery of the appropriate timing of care must be achieved.
Conclusion
This scoping review identified several international healthcare systems with clearly defined models of care specific to the rehabilitation and lifelong care of persons with SCI for a high-income country such as Canada. Despite the lack of international uniformity in the SCI model of care, positive attributes from the various models have been identified. By understanding these attributes, we are better equipped to identify gaps and opportunities for SCI service delivery across the SCI continuum, hence improving care to persons with SCI.
Footnotes
Acknowledgments
We would like to thank University of Calgary W21C, the Praxis Spinal Cord Institute, and Dana Hunter, clinical research assistant, University of Calgary.
Funding Information
CH is supported by the University of Alberta Spinal Cord Injury Research Chair endowment funds, the Alberta Paraplegic Foundation, and the Canadian Institutes of Health Research Team Grant for Transitions in Care.
SJTG is supported by a Canadian Institutes of Health Research Embedded Clinician Scientist Salary Award on Transitions in Care working with Ontario Health (Quality).
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Appendix SA
Supplementary Appendix SB
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.