
Abstract
Traumatic brain injury (TBI) often results in chronic psychiatric-like symptoms. In a condition with few therapeutic options, neuromodulation has emerged as a promising potential treatment avenue for these individuals. The goal of the current study was to determine if transcranial direct-current stimulation (tDCS) could treat deficits of impulsivity and attention in rats. This could then be used as a model to investigate treatment parameters and the mechanism of action underlying therapeutic effects. Rats were trained on a task to measure attention and motor impulsivity (five-choice serial reaction time task), then given a frontal, controlled cortical impact injury. After rats recovered to a new baseline, tDCS (cathodal, 10 min, 800 μA) was delivered daily prior to testing in a counterbalanced, cross-over design. Treatment with tDCS selectively reduced impulsivity in the TBI group, and the greatest recovery occurred in the rats with the largest deficits. With these data, we have established a rat model for studying the effects of tDCS on psychiatric-like dysfunction. More research is needed to determine the mechanism of action by which tDCS-related gains occur.
Traumatic brain injury (TBI)-induced cognitive and psychiatric-like dysfunction significantly impairs quality of life for a growing population. 1,2 Despite this, treatments have been difficult to identify. Changes to monoaminergic function have received considerable attention 3,4 with dopamine (DA) abnormalities emerging as a potential contributor to cognitive impairments. 5 –7 A recent study in rats demonstrated that cathodal transcranial direct-current stimulation (tDCS) raises striatal levels of DA, 8 suggesting it could have efficacy in treating DA-related cognitive deficits in patients with TBI. In fact, recent studies in TBI populations have shown efficacy of tDCS in treating working memory, attention, and risky decision-making. 9 –11
To fully understand how tDCS may improve function, animal models of chronic psychiatric-like dysfunction after TBI are needed. Our lab has demonstrated long-lasting deficits in attention, impulsivity, and risky decision-making in a rat model of TBI. 12,13 In the current study, we sought to determine whether tDCS stimulation could effectively treat chronic psychiatric-like symptoms such as impulsivity and attentional impairments after a brain injury in rats. The goal was to establish a model that could be used to further investigate treatment parameters and mechanisms of action for tDCS in recovery of cognitive function.
Male Long-Evans rats were trained on the five-choice serial reaction time task, a behavior designed to measure motor impulsivity and attention. 13 Rats are required to respond to a briefly displayed visual stimulus in one of five holes. Because the presentation is so brief, this sets up a prepotent motor response that must be inhibited for a set amount of time (5 sec), yielding a measure of both attention and motor impulsivity. Rats were trained to stability (50 sessions), then given a bilateral, frontal, controlled cortical impact TBI (n = 10; 5-mm impact centered at AP/ML +3.0/0.0, DV −2.5 @ 3 m/sec, corresponding to severe injury) or sham procedures (n = 10), as previously described, with a Leica impactor (Leica Biosystems, Buffalo Grove, IL) and 1 week of recovery. 13
After 6 weeks of post-injury testing to allow rats to recover to a new baseline, tDCS sessions began. Stimulation was carried out according to parameters from a previous study in which ventral striatal DA levels were increased
8
and was delivered in a within-subjects cross-over design. Under isoflurane anesthesia, seven sessions of current (cathodal, 10 min, 800 μA, 7.08 A/m2) or sham stimulation were given using commercially available Ag/AgCl hydrogel electrodes (The Electrode Store, Enumclaw, WA) placed on shaved skin in front of bregma (cathode) and between the scalpulae (anode), followed by 5 days of washout, with testing at 2 h after stimulation. Thus, the study timeline was: Training (10 weeks) → Injury & Recovery (1 week) → Post-injury baseline (6 weeks) → tDCS/Sham stimulation (7 days) → Washout (5 days) → Sham/tDCS stimulation (7 days; condition reversed from prior) → Washout (5 days) → Post-stimulation baseline (1 week) → Perfusion.
At the conclusion, rats were transcardially perfused and brains were sliced and examined to verify injury. Data were transformed as necessary to normalize distributions and analyzed via linear mixed-effects regression in R (Fixed effects: Injury Group × Week; Injury Group × Session × Stimulation + baseline; Random effects: Subject intercept).
The TBI group had significantly reduced accuracy (β = −0.07, t = 2.82, p = 0.005) and increased impulsivity (β = 1.19, t = 7.87, p < 0.001) that did not recover over the 6-week post-injury period (Fig 1A,B). Stimulation slightly decreased accuracy (β = −0.08, t = 2.10, p = 0.037; Fig 1C,D), and significantly reduced impulsivity (β = −0.43, t = 3.40, p = 0.001; Fig 1E,F) in TBI rats. There was a significant relationship between magnitude of impairment and tDCS-induced recovery on impulsivity (b = −0.62, t = 2.72, p = 0.035, AdjR 2 = 0.61; Fig 1G,H), even when the size of the lesion was factored in.
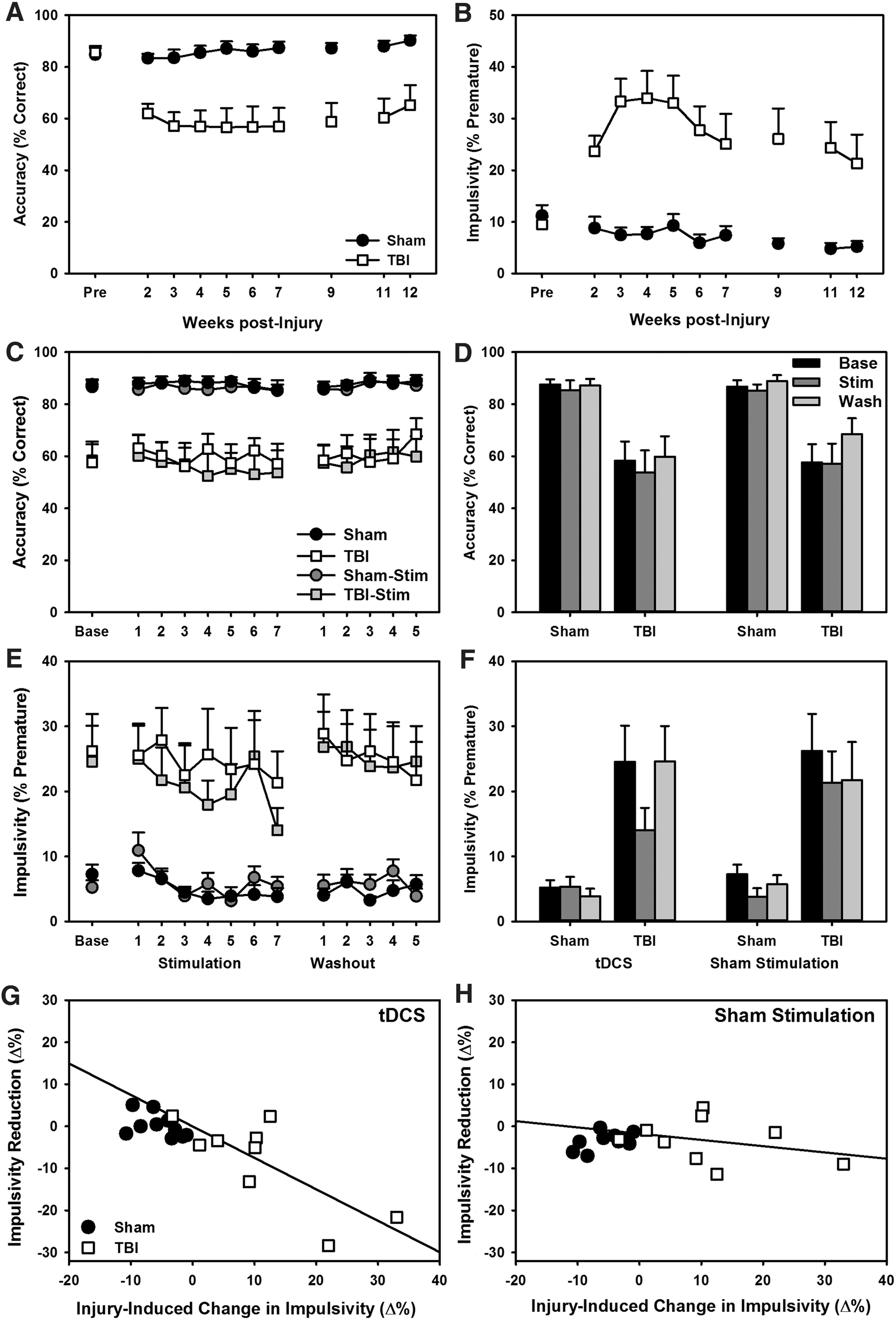
Effects of TBI and tDCS on attention and impulsivity. All data are means + SEM.
The treatment of chronic brain injury is a difficult task, and will likely require multi-modal therapies including rehabilitative, pharmacological, and potentially, neuromodulatory approaches. With the increased prevalence of deep brain implants, neuromodulation has emerged as a major field with numerous promising applications. There is a proven track record of neuromodulatory techniques in motor disorders, 14 and new evidence is emerging for efficacy in other “cognitive” diseases, such as addiction. 15,16 In the current study, we provide additional evidence for the use of tDCS in the treatment of psychiatric-like dysfunction in the chronic post-TBI period and establish an animal model for exploring the mechanisms by which stimulation may reduce impulsivity. Prior studies of neuromodulation in long-term dysfunction after TBI have been limited, but one demonstrated considerable recovery when direct cortical annodal alternating current was performed concomitant with motor training. 17 Another study observed dramatic improvement in motor outcomes when tDCS was delivered immediately prior to behavior, but failed to translate these findings to measures of working memory. 18 Future studies should explore whether combining stimulation with cognitive training may further augment recovery. In addition, the effect of location and modality of injury on neuromodulatory treatments remain to be investigated.
The precise mechanisms by which tDCS exerts its effects are varied and may include alterations to individual neuronal firing, disruption of circuits (including those involved in long-term potentiation), and generation of plasticity-related factors such as brain-derived neurotrophic factor (BDNF). 19 However, in the current study, we observed no lingering effects of stimulation—benefits disappeared as soon as stimulation was stopped—suggesting a more acute mechanism as opposed to long-term changes. This is somewhat perplexing when compared with the general literature on neurmodulation and plasticity.
However, whereas a prior study of tDCS in experimental TBI found a correlation between BDNF expression in perilesional cortex and memory function, 20 these gains were also transient in nature, making it difficult to determine whether BDNF expression truly affected function. This suggests there may be some fundamental differences in the injured brain that may limit generalized interpretation from neuromodulation in intact populations. In addition, a majority of experimental studies have used anodal tDCS as opposed to the cathodal stimulation employed in the current study. This may be of relevance given prior evidence that cathodal, but not anodal, stimulation facilitates increased DA release 8 and may explain why there were cognitive improvements shown in the current study data although prior TBI studies were limited to motor effects. Further understanding of the mechanisms by which tDCS may confer beneficial effects will need to compare anodal and cathodal stimulation to dissociate acute dopaminergic mechanisms from long-term growth factor-related or synaptic mechanisms and determine how these processes are altered in the injured cortex.
A particular finding from the current study that may be of importance is the relationship between the magnitude of impulsive deficit and degree of tDCS-induced recovery. These results suggest that the most severely impaired may benefit the most from neuromodulation. These findings may also be reflected in clinical studies. In a recent study examining effects of tDCS on risky decision-making, the TBI sample was considered to be clinically/significantly impulsive and were treatment-seeking. 11 However, whereas a reduction in impulsivity would be considered beneficial, it should be noted that we also observed a small decrease in attention during stimulation. If this effect replicates, this may temper enthusiasm for tDCS as a treatment in TBI populations. Additionally, given the relationship with injury severity observed here, future studies will need to determine whether neuromodulatory approaches may be beneficial in milder or concussive injury. Moreover, although tDCS has been the focus of this study, there has been a surge of interest in other neuromodulatory techniques for TBI. This potential has been reviewed recently, 21 –23 along with several experimental studies in animals exploring everything from extremely focal (e.g., deep brain stimulation) to decidedly broad (e.g., pulsed ultrasound). 24 –26 Going forward, it will be important to identify common and disparate mechanisms between these neuromodulatory techniques that contribute to recovery of function.
The data presented here strongly map on to observations within TBI clinics and highlight the translational nature of the rat as a model for chronic TBI-related dysfunction. The use of sophisticated, long-term cognitive testing should open a window into the study of TBI recovery and enable investigation into parameters and mechanisms of neuromodulatory techniques such as tDCS.
Footnotes
Acknowledgments
We thank Gabrielle Portillo, Trinity Shaver, Michelle Frankot, and other members of the Vonder Haar lab for their assistance with performing behavioral and histological analyses. Funding for this project was provided by grants from the National Institute of General Medical Sciences (NIGMS; 5P20GM109098-04) and West Virginia University.
Author Disclosure Statement
No conflicting financial interests exist.