
Abstract
This systematic review provides a comprehensive, up-to-date summary of traumatic brain injury (TBI) epidemiology in Europe, describing incidence, mortality, age, and sex distribution, plus severity, mechanism of injury, and time trends. PubMed, CINAHL, EMBASE, and Web of Science were searched in January 2015 for observational, descriptive, English language studies reporting incidence, mortality, or case fatality of TBI in Europe. There were no limitations according to date, age, or TBI severity. Methodological quality was assessed using the Methodological Evaluation of Observational Research checklist. Data were presented narratively. Sixty-six studies were included in the review. Country-level data were provided in 22 studies, regional population or treatment center catchment area data were reported by 44 studies. Crude incidence rates varied widely. For all ages and TBI severities, crude incidence rates ranged from 47.3 per 100,000, to 694 per 100,000 population per year (country-level studies) and 83.3 per 100,000, to 849 per 100,000 population per year (regional-level studies). Crude mortality rates ranged from 9 to 28.10 per 100,000 population per year (country-level studies), and 3.3 to 24.4 per 100,000 population per year (regional-level studies.) The most common mechanisms of injury were traffic accidents and falls. Over time, the contribution of traffic accidents to total TBI events may be reducing. Case ascertainment and definitions of TBI are variable. Improved standardization would enable more accurate comparisons.
Editor's Note: This article is published as a Living Systematic Review. All Living Systematic Reviews will be updated at approximately three-six month intervals, with these updates published as supplementary material in the online version of the Journal of Neurotrauma (
Introduction
Traumatic brain injury (TBI) is among the most severe types of injury in terms of both case fatality 1 and long-term implications for survivors. 2 Treatment of TBI can be complex and expensive. 3 Upon clinical examination, TBI is most commonly sub-divided into mild, moderate, and severe, according to the Glasgow Coma Scale (GCS). 4,5 Such categories have been found to be predictive of a patient's long-term outcome, 6 although other measures and models also have been tested. 7,8
A previous review of the epidemiology of TBI in Europe concluded that the leading causes of TBI were road traffic collisions, and falls. 3 Consequently, in a densely populated and economically advanced area such as the European Union (EU), the potential for prevention of morbidity and mortality is great. The variability in incidence and mechanism of TBI, which may be observed on this mainly contiguous land-mass with a well-developed road network, is also of scientific interest, as it may lead to better prevention of TBI. Countries within the EU adhere to certain multi-national laws and agreements, but nonetheless retain their own law-making and enforcement responsibilities. 9 This may add further complexity to the understanding of TBI epidemiology, for example, in the contributions of varying road speed limits or the legal restrictions on the availability of firearms. More generally, the issues relating to the contemporary demographic and lifestyle characteristics of the similar countries or regions suggest that epidemiological trends from EU countries also may be applicable to other high income countries.
Considerable variability has been observed between national rates, largely attributable to significant variability in data collection, case ascertainment, and case definition. This has led to calls for standardized definitions and data collection in population-based studies, and an associated paradigm shift in studying TBI and its impact. 10 –12
In order to improve the understanding of causes of TBI and the scale of the problem, it is important to analyze the current situation and time trends, using good quality comparable observational studies. One comprehensive systematic review of the epidemiology of TBI in Europe was published nearly ten years ago. 3 A recent systematic review, 13 published as a follow-up to Tagliaferri (2006), 3 addresses similar issues but was more restrictive in dates of publication (1990–2014) and has not been set up as a “living” systematic review (i.e., it is not expected that it will be kept up-to-date as new research is published). 13
The overall objective of this systematic review was to provide a comprehensive, up-to-date summary of TBI epidemiology in Europe by reviewing all relevant observational studies. Specific aims were to determine the incidence, mortality, age, and sex distribution of TBI in Europe, along with the severity and mechanism of injury and time trends.
Methods
This review was conducted and reported in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement.
14
Details of the protocol for this systematic review were registered on PROSPERO (registration number 2014: CRD42014015517) and can be accessed at
This review was prepared as a “living systematic review” as part of the Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury (CENTER-TBI) project. CENTER-TBI is a European project aiming to improve outcomes for people with TBI through better classification, characterization, and management of this injury. 15 A living systematic review is a high quality, up-to-date online summary of health research that is updated as data from new relevant research that meets study inclusion criteria becomes available. 16 In practice, this means that the searches will be re-run frequently, any new studies incorporated into the review, and updates will be regularly published. 17
Information sources
The following databases were searched: PubMed, Web of Science, CINAHL, and EMBASE from 1960 up to January 15, 2015. For each of these, searches were performed in March and April 2014 with a combination of key words and subject headings (Appendix 1). The same searches were re-run in January 2015. To reduce the risk of publication bias, searches also were undertaken in gray literature and references of included studies.
Study selection/inclusion criteria
Retrospective and prospective descriptive studies that reported on the epidemiology of TBI in Europe were included. To be eligible for the review, studies must have been an original study (i.e., not a review or duplicate of previously published data) that measured and reported incidence, mortality, or case fatality of TBI in Europe, and was published in English. Study size was not restricted and data collected from hospitals or official statistics were eligible. There were no limitations regarding the dates of data collection, study performance or publication, participant age, or TBI severity.
For some of these terms, such as TBI, incidence, mortality, and case fatality, the definition used by authors can vary. For the purposes of this review, these terms were defined in the following ways: TBI: Defined as an injury to the head, by either blunt force or penetrative means, which causes sufficient damage that the patient suffers a change in brain function; or more recently, as an alteration in brain function, or other evidence of brain pathology, caused by an external force.
11
Ascertainment of a TBI case could be by any of the following: International Classification of Diseases (ICD) in its 8th, 9th and 10th revision codes, Abbreviated Injury Score for head injuries (AISHead or HAIS), the Glasgow Coma Scale (GCS), or clinical signs (such as loss of consciousness, post-traumatic amnesia, or pathologies found in computed tomography/magnetic resonance imaging scan). Incidence: Rate of TBIs recorded per 100,000 population per year. These were usually first-time events. Mortality: Total number of fatal TBIs in a given population per 100,000 population per year. Case fatality: Proportion of people with TBI who subsequently died due to a cause related to the TBI at certain time-points. TBI severity: Categories of severity (severe, moderate, mild), as defined by the GCS (e.g., 3–8 [mild], 9–12 [moderate], and 13–15 [severe],
5
or other classification system used by the authors.
Two authors (WP, VB) independently screened citations on titles and abstracts, excluding any obviously irrelevant or duplicate citations. Results were compared and disagreements discussed with a third author and/or with members of an expert panel. Agreed citations were retrieved in full text and screened independently by two authors (AB, VB, MM, VR, MT) using the same process. Screening was undertaken using Covidence, a not-for-profit web-based tool designed to assist in conducting systematic reviews. 18
Data collection and assessment of methodological quality
Two authors (AB, VB, MM, VR, or MT) independently extracted data and assessed methodological quality of selected studies. Any discrepancies were resolved by discussion.
The following items were extracted from each study: study authors, year of publication, study time period, type of data source, method and completeness of case ascertainment, criteria for identifying TBI, source population, number of TBI cases reported, reported data on TBI incidence, mortality, and case fatality, broken down by sex, age, severity, and mechanism of injury.
Methodological quality was assessed using the Methodological Evaluation of Observational Research (MORE) checklist, as previously used in reviews of non-therapeutic studies. 19,20 The following domains of bias or quality are assessed with the MORE checklist: funding of study, conflict of interest, study design, sampling, definition of cases, source of data, and reliability of estimates. Each domain was judged according to specific criteria and scored as “OK, Minor Flaw, Major Flaw, and Poor reporting” (Appendix 2) No studies were excluded from the review based on methodological quality.
Data synthesis
To facilitate appropriate comparisons, studies were first grouped according to whether they reported country-level data (derived from national hospital or mortality registries) or regional-level data, denoting smaller populations within studies (derived from regional/country or hospital catchment areas). Other stratifications–for example, by study design and retrospective/prospective data collection–were considered, but the strata generated by this means were too small to make meaningful comparisons.
Findings are described overall, and also broken down according to age, sex, severity of TBI, and mechanism of injury. Time trends of incidence and mortality of TBI also are described.
Statistical analysis
Data are presented in tables and figures. Meta-analysis of incidence and mortality rates was not possible, as too few studies reported age-adjusted data and it was not possible to obtain the raw data from study authors to perform standardization. A funnel plot was generated to consider small study effects in regional-level studies; the country-level studies were not plotted as there were too few studies (fewer than 10).
Results
Description of studies
A total of 4289 citations were identified. After removing duplicates, 4232 were screened on citation and abstract and 4011 were excluded. As such, 221 papers were screened for eligibility, with 66 included as full-text (Fig. 1).
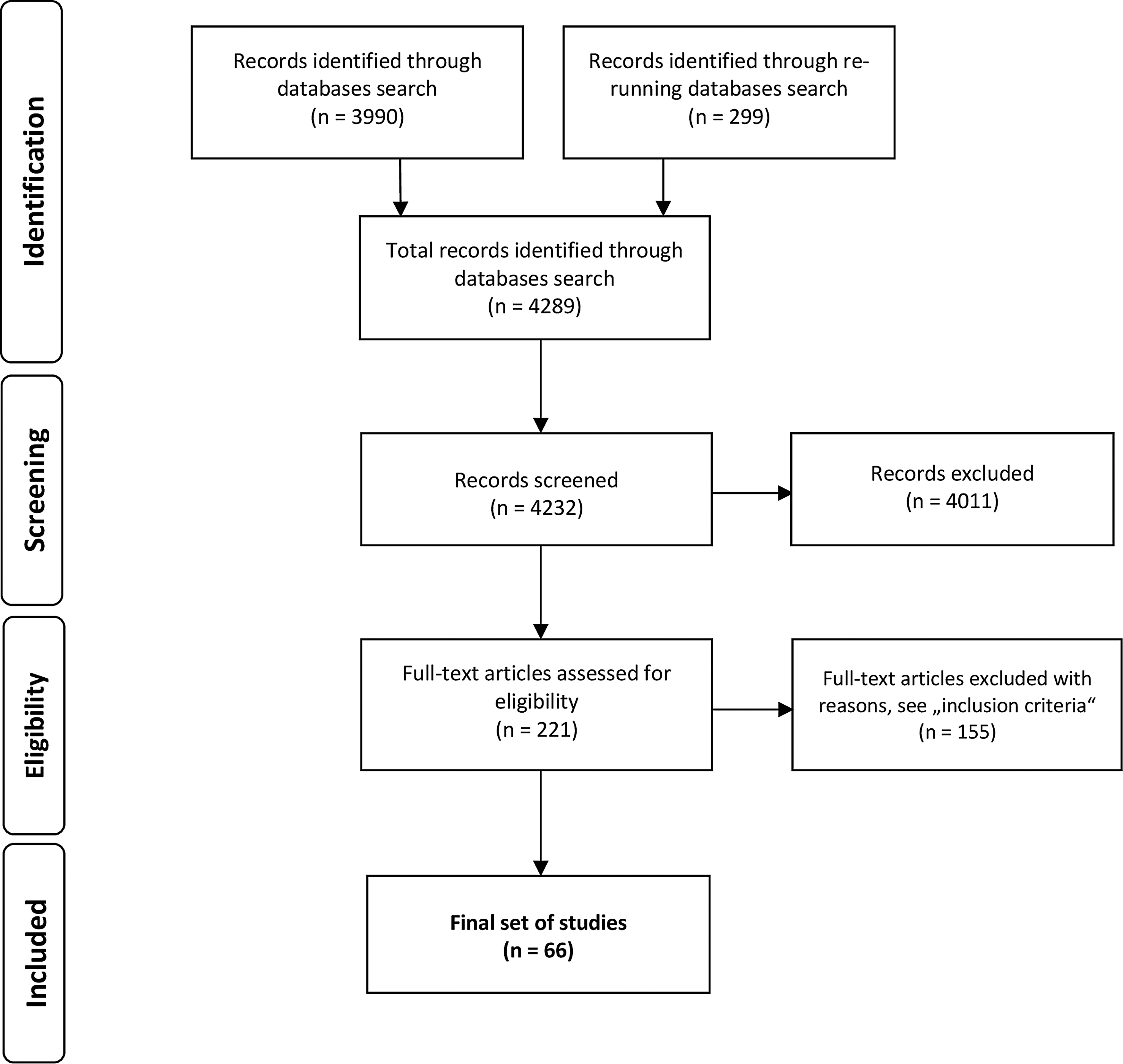
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart of the study selection process.
Characteristics of included studies
Of the 66 included studies, 22 provided country-level data from Finland (n = 4); Austria (n = 4); Denmark (n = 3); the Netherlands (n = 2); Norway (n = 2); Sweden (n = 2); and Scotland, Germany, Great Britain, Spain, Portugal, Switzerland, and the Republic of San Marino, (n = 1, each). A further 44 reported on either a regional population (one or more country regions, counties or provinces) or the catchment area of one or more treatment centers. All studies together represented 23 European countries–those mentioned above and Italy, France, Iceland, Ireland, United Kingdom, Bosnia, Croatia, Macedonia, Slovak Republic, Estonia, and Greece.
The majority of studies (n = 25) had study periods of 1 or 2 years, with a further 17 reporting data over 10 years or more. The remaining studies reported a time period of 3 – 10 years. The number of included cases ranged from 10121 (included severe TBI only) to 208,195. 22 Tables 1 and 2 present the characteristics of included studies.
Characteristics of Studies With Country-Level Population
% if clearly stated.
M, males; F, females; TBI, traumatic brain injury; ICD, International Classification of Diseases; NR, not reported; T, traffic related; F, falls; Su, suicide; ISS, Injury Severity Score; HAIS, Head Abbreviated Injury Scale; GCS, Glasgow Coma Scale.
Characteristics of Studies With Regional-Level Population
% if clearly stated.
M, males; F, females; TBI, traumatic brain injury; ICD, International Classification of Diseases; NR, not reported; T, traffic related; F, falls; H, accidents at home; ICU, intensive care unit; GCS, Glasgow Coma Scale; S, sport; W, accidents at work/industrial accidents; AISHead, Abbreviated Injury Score for head injuries; ACRM, American Congress of Rehabilitation Medicine; HISS, Head Injury Severity Scale; V, violence; HAIS, Head Abbreviated Injury Scale; TRISS, Trauma and Injury Severity Score.
Inclusion criteria, case ascertainment, and case definition varied markedly across studies. Most had data from hospital registries, either directly from participating centers or from regional/national registries to which the hospitals reported. Some studies also used mortality registries, either hospital-based or regional/national mortality databases. Our review found a wide variety of definitions of the injury itself. A summary of the inclusion criteria, case ascertainment, and classification of TBI in individual studies is presented in Tables 3 and 4.
Case Ascertainment in Studies With Country-Level Population
all ages and all severity if not specified otherwise; **presented terminology is the same as in the original study.
TBI, traumatic brain injury; ICD, International Classification of Diseases.
Case Ascertainment in Studies With Regional-Level Population
all ages and all severity if not specified otherwise; **presented terminology is the same as in the original study.
TBI, traumatic brain injury; ICD, International Classification of Diseases; CT, computed tomography; EEG, electroencephalogram; GCS, Glasgow Coma Scale; AISHead, Abbreviated Injury Score for head injuries; HAIS, Head Abbreviated Injury Scale; ED, emergency department; ISS, Injury Severity Score; ICU, intensive care unit.
More recent studies commonly, although not exclusively, use the ICD 9 and ICD 10 coding systems. Some early studies used ICD 8 (e.g., Engberg and Teasdale [1998]). 23 Other standardized coding schemes, such as the Abbreviated Injury Score for head injuries (AISHead or HAIS) as in Walder and colleagues (2013), 24 and the Glasgow Coma Scale (GCS) as in Boto and colleagues (2009), 25 also were used occasionally. In summary, 31 studies used ICD (8th, 9th, or 10th revision), and 20 studies used GCS or GCS and/or other criteria (usually AIS).
Older studies (from the 1980s and 1990s) tended to use definitions of TBI based on clinical signs, such as “[Head/brain injury with] a) loss of consciousness; b) skull fracture; c) objective neurologic findings which could be reasonably attributed to the head injury,” as in Vazquez-Barquero and colleagues (1992). 26
Severity of TBI was measured mainly by GCS, although other scales such as AISHead also were seen, along with non-standardized clinical definitions, for example, based on duration of lost consciousness.
Of the 66 included studies, 15 presented information on severe TBI only, two on moderate and severe, and two on mild TBI only. The rest of the studies presented information on all TBI severities.
Methodological quality
General markers of study rigor, such as a clearly specified research design and the reporting of ethical clearance, funding sources, or potential conflicts of interest were more complete in more recent papers, but rarely found in older papers (see Table 5 for summary assessment).
Quality Assessment of Included Studies Using MORE Checklist–Summary Results
MORE, Methodological Evaluation of Observational Research checklist; TBI, traumatic brain injury.
The quality of reporting in the final set of studies was found to be mixed. Some items were generally well reported, for example, the criteria used to define TBI and the data source use of either hospital records or national statistics to calculate incidence.
Incidence
Fifty-one studies reported a measure of TBI incidence, albeit with significant variation around the definition of case ascertainment and case definition (Tables 3, 4, 6, 7). Only eight studies reported the use of age-standardization of incidence rates or confidence intervals around these figures.
Outcomes in Studies With Country-Level Population
All ages, if not specified otherwise; **crude rates, if not specified otherwise; ***hospital, if not specified otherwise; st.standardized; amedian for all countries; baverage during 15 years.
NR, not reported; En, England; W, Wales; Scot, Scotland; M, males; F, females; DE, Denmark; FI, Finland; NO, Norway; SE, Sweden.
Outcomes in Studies With Regional-Level Population
All ages, if not specified otherwise; **crude rates, if not specified otherwise; ***hospital, if not specified otherwise; st.standardized; amedian for all countries; baverage during 15 years.
NR, not reported; CI, confidence interval; HI, high income; UMI, upper middle income; LMI, lower middle income.
Of the 22 country-level studies (Table 6), 12 reported on the incidence of TBI across all severities and of these, 11 included subjects of all ages. Two studies reported on fall-related TBIs only, while the majority of studies reported two or more types of mechanism of injury.
In the group of country-level studies, the range of reported crude incidence rates is as follows: the lowest reported incidence rate is by Pérez and colleagues (2012) in Spain (study period 2000–2009; 47.3 per 100,000 population per year) 27 ; the highest is reported by Servadei and colleagues (1985) for the Republic of San Marino (study period 1981–1982; 694 per 100,000 population per year). 28 Crude incidence and mortality rates of all country-level studies that include all ages and all severities of injury are presented in Figure 2 in chronological order by study period.
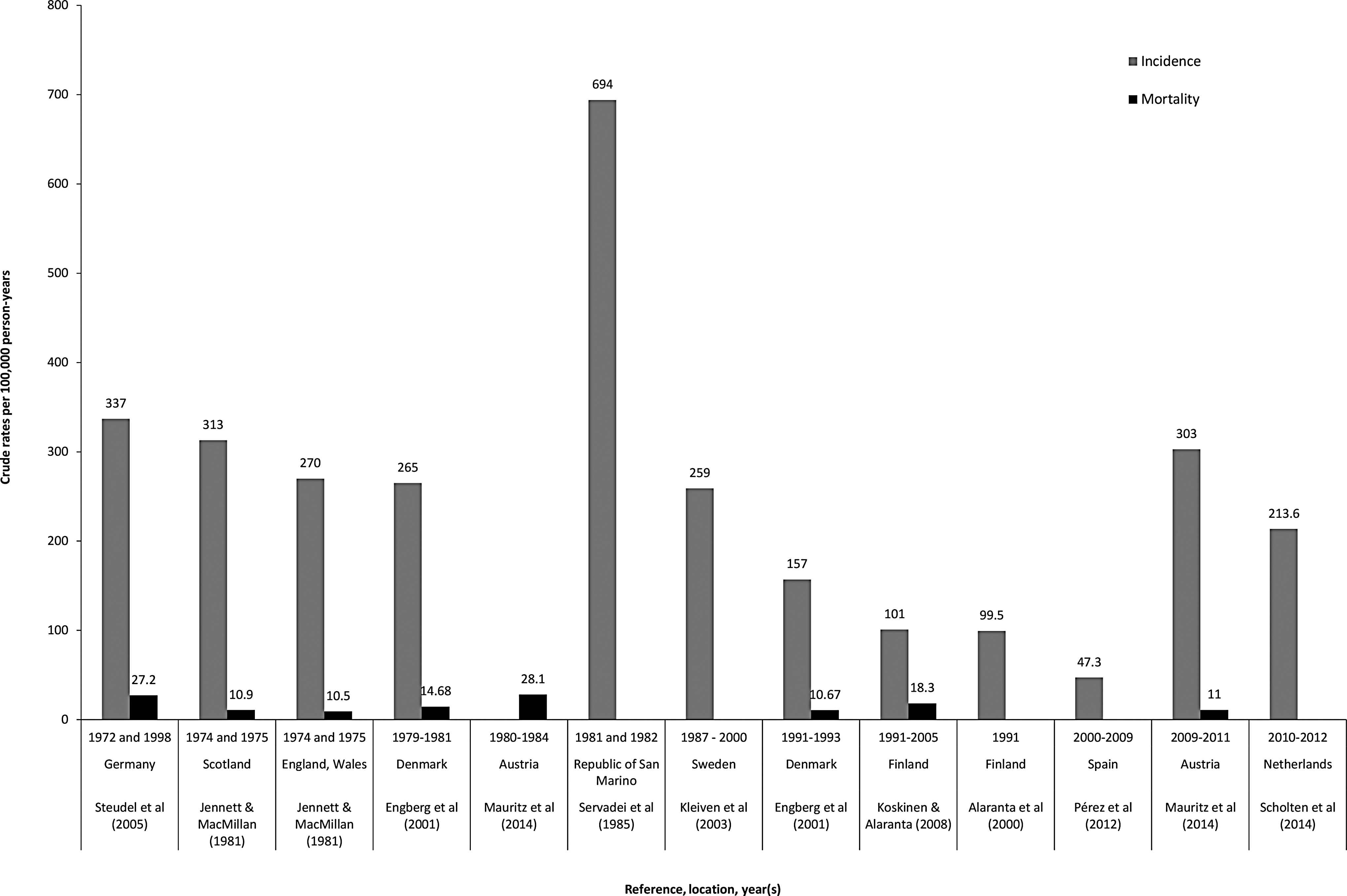
Traumatic brain injury incidence and mortality rates (crude) per 100,000 population per year in country-level studies.
Of 44 regional-level area studies (Table 7), 14 reported incidence rates for all ages and all severities. Two studies reported on only one mechanism of injury–traffic accidents. Figure 3 shows the crude incidence and mortality rates of these studies that include all ages and all TBI severity in chronological order by study period. The range is even larger here than in the group of country-level studies (Fig. 2): the lowest is reported by Andelic and colleagues (2008) for Norway (83.3 per 100,000 population per year) 29 ; and the largest is reported by Servadei and colleagues (1988) for Italy (849 per 100,000 population per year). 30
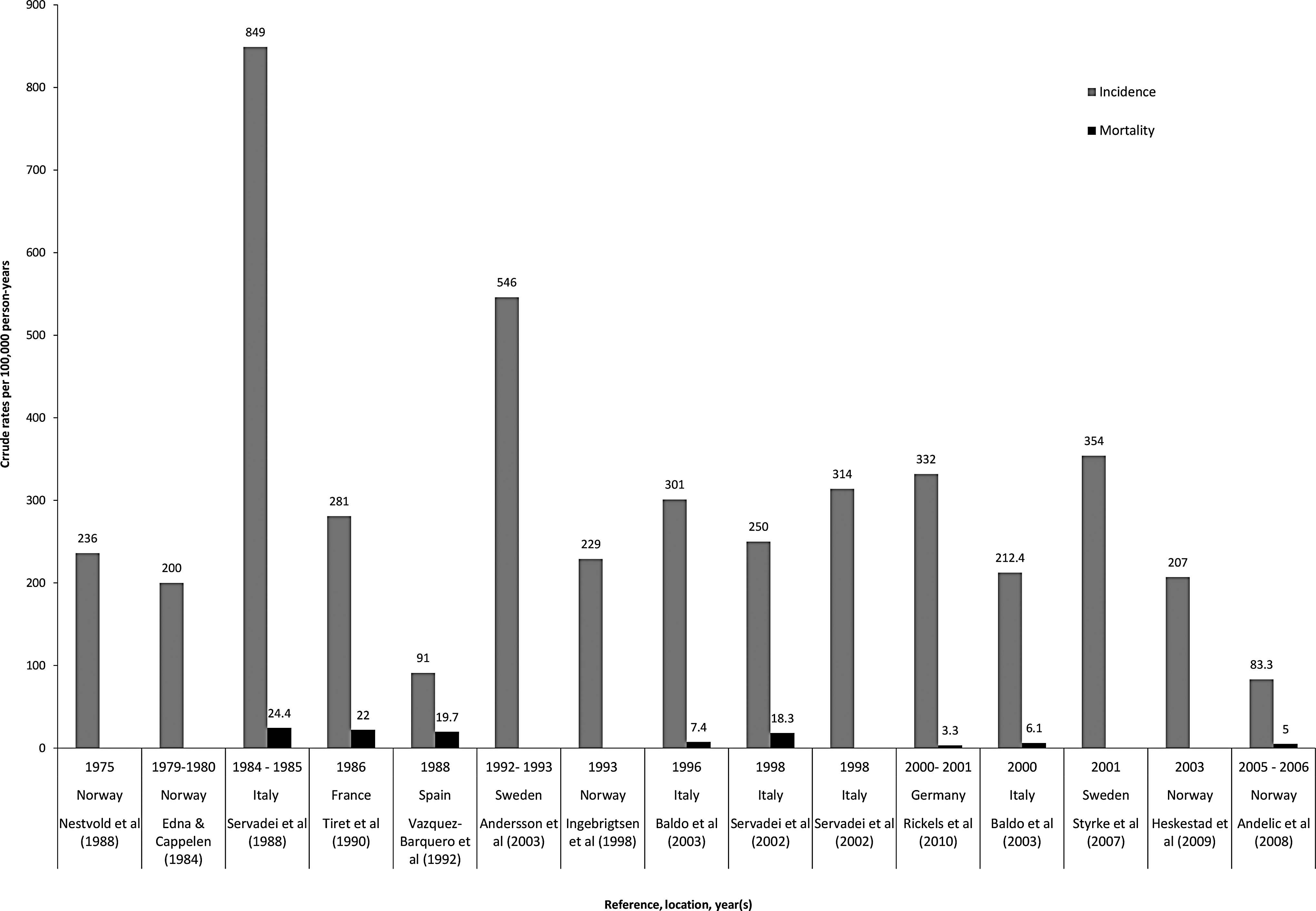
Traumatic brain injury incidence and mortality (crude) rates per 100,000 population per year in regional-level studies.
The range of crude incidence rates with confidence intervals in two sets of studies – nine country-level studies and 14 regional-level studies is shown in Figure 4 and 5, respectively. In order to make the fairest assessment, the figures include only studies reporting on all ages and all TBI severities.
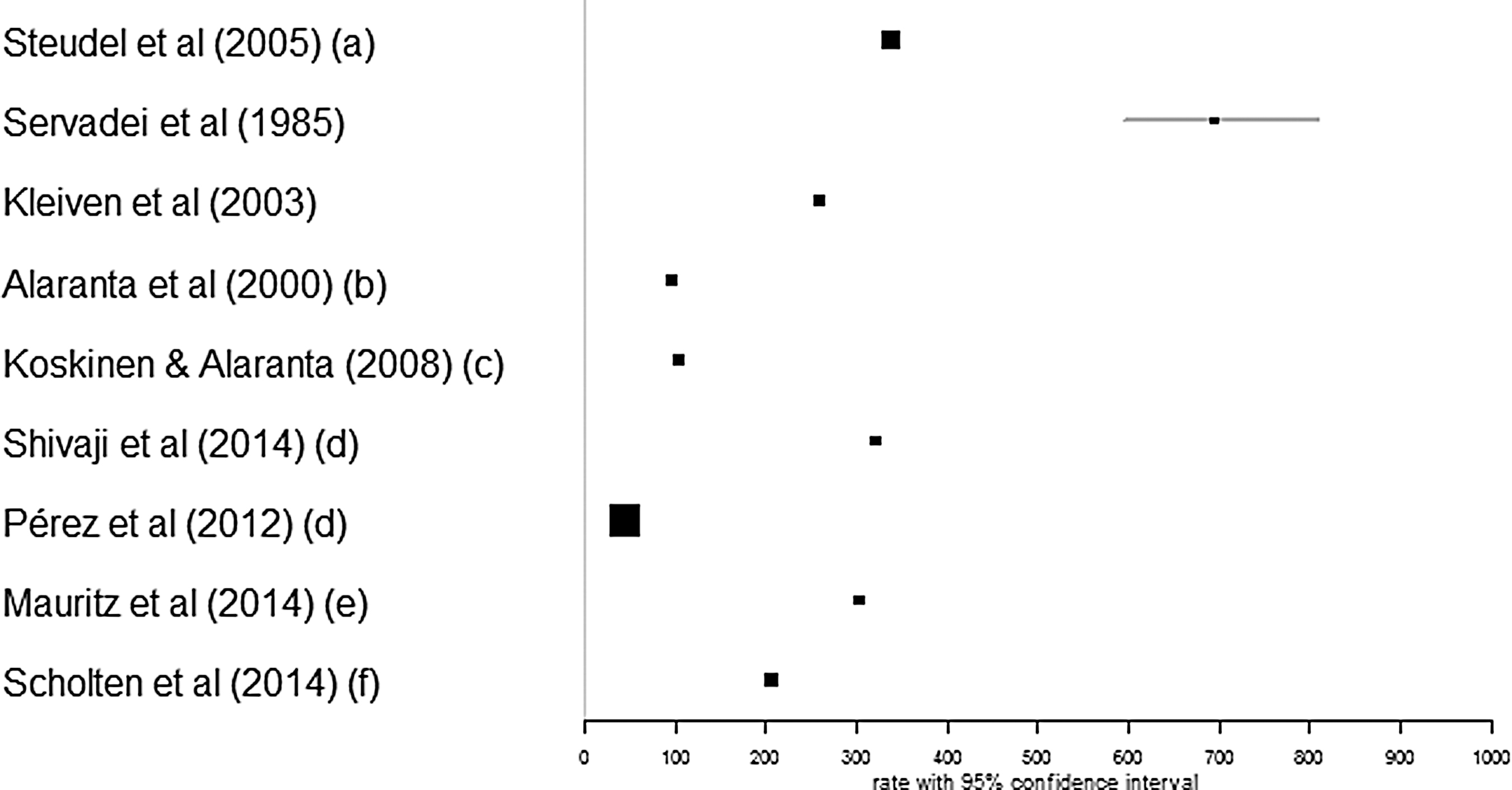
Traumatic brain injury (TBI) incidence rates (crude) per 100,000 population per year in country-level studies. Studies reporting on all ages and all TBI severity were used. The size of the boxes depicts the weight (relative to other studies in the analysis) that the study has in relation to the summary measure of the meta-analysis; larger boxes depict higher weight. (a), 1998 data; (b), average for 5-year period (1991–1995); (c), 2001–2005 data; (d), 2009 data; (e), average for 2009–2011; (f), average for 2010–2012.
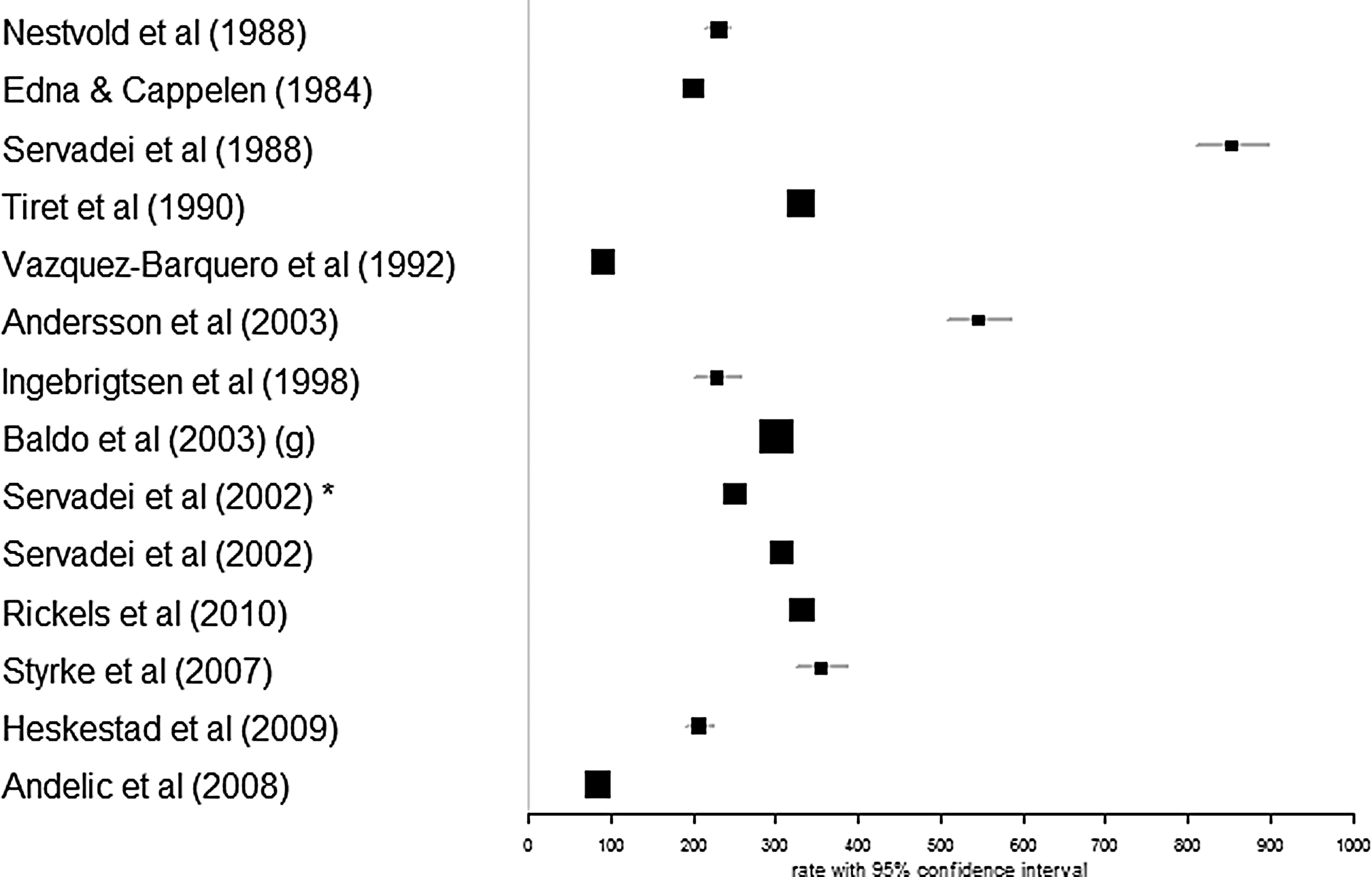
Traumatic brain injury (TBI) incidence rates (crude) per 100,000 population per year in regional-level studies. Studies reporting on all ages and all TBI severity were used. The size of the boxes depicts the weight (relative to other studies in the analysis) that the study has in relation to the summary measure of the meta-analysis; larger boxes depict higher weight. *ref. no. 80; (g), 1996 data.
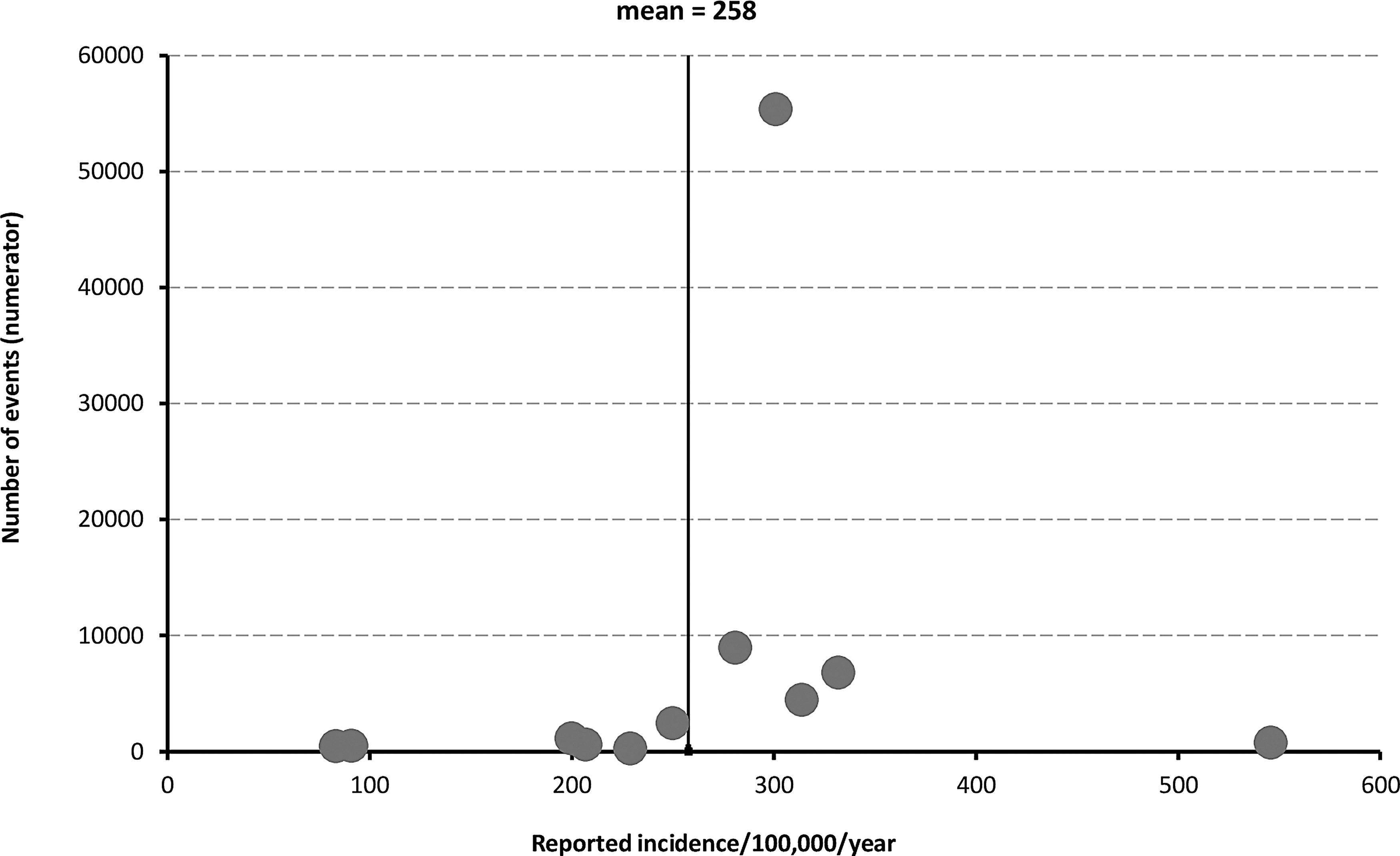
The funnel plot of incidence rates of regional-level studies, shown in Figure 6, suggests there is little indication of missing or selectively unpublished data. The plot shows a wider variability in incidence estimates in smaller studies, with a more stable incidence rate in larger studies, close to the mean value of 258 per 100,000 population per year. There were insufficient studies at national level reporting enough detail to produce a funnel plot for country-level studies.
Funnel plot of traumatic brain injury incidence in regional-level studies.
Mortality and case fatality rates
Of the 27 studies reporting mortality rates, 14 reported mortality across ages and severities (Tables 6 and 7). Mortality rates of studies including all ages and all severities are presented together, with incidence rates in Figure 2 for country-level studies, and Figure 3 for regional-level area studies. As with incidence, range of reported crude mortality rates is quite large–from 9 per 100,000 population per year (Steudel and colleagues [2005]) 37 to 28.10 per 100,000 population per year (Mauritz and colleagues [2014]) 38 in country-level studies, and from 3.3 per 100,000 population per year (Rickels and colleagues [2010]) 39 to 24.4 per 100,000 population per year (Servadei and colleagues [1988]) 36 in regional-level studies.
Age and sex
Age and sex breakdown was reported in the majority of studies. It is difficult to compare distribution of TBI across populations, as many studies report only on part of the population (children or older adults, or adults only, etc.). Mean (or median) age was stated in 32 studies. In studies of all ages, all TBI severities, and all mechanisms, the lowest reported mean age was 26.7 in the Republic of San Marino (Servadei and colleagues [1985]), 28 the highest was 44.5 in Austria in 2009–2011. 32 The reported proportion of males was always greater than that of females (irrespective of age, severity and mechanism of injury), ranging from 55% in Sweden in 200134 to 80% in Ireland in 2005–2007. 35
Mechanism of injury
A total of 57 studies recorded the mechanisms of injury; of these, 16 were studies that reported on TBI across country-level populations and a further 41 studies reported on specific mechanisms of injury from regional-level populations. Across ages and severities, the three most common mechanisms (or two if only two mechanisms were reported) of injury for each sample are presented in the Figures 7 and 8.
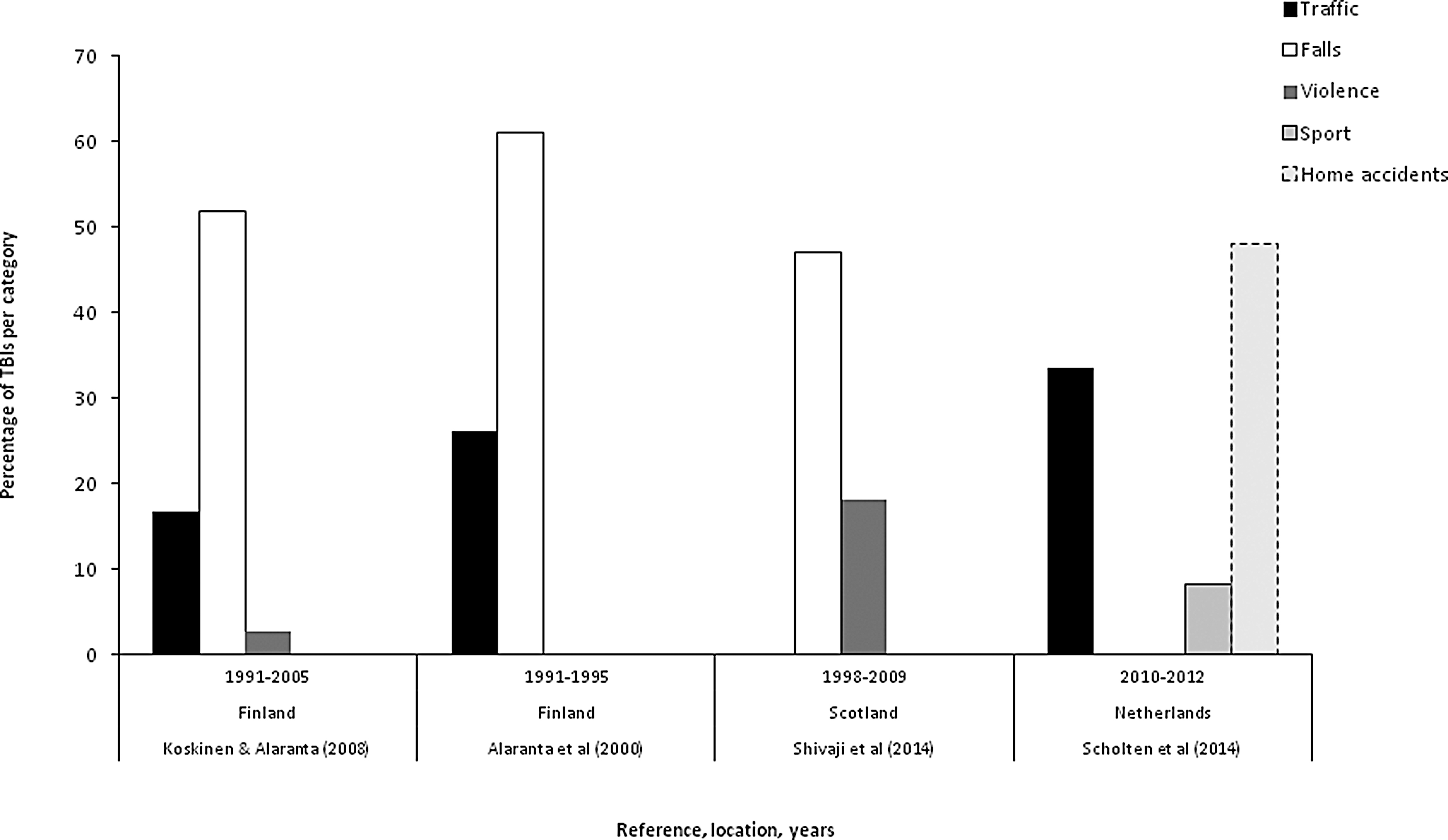
The most common mechanisms of injury in country-level studies.
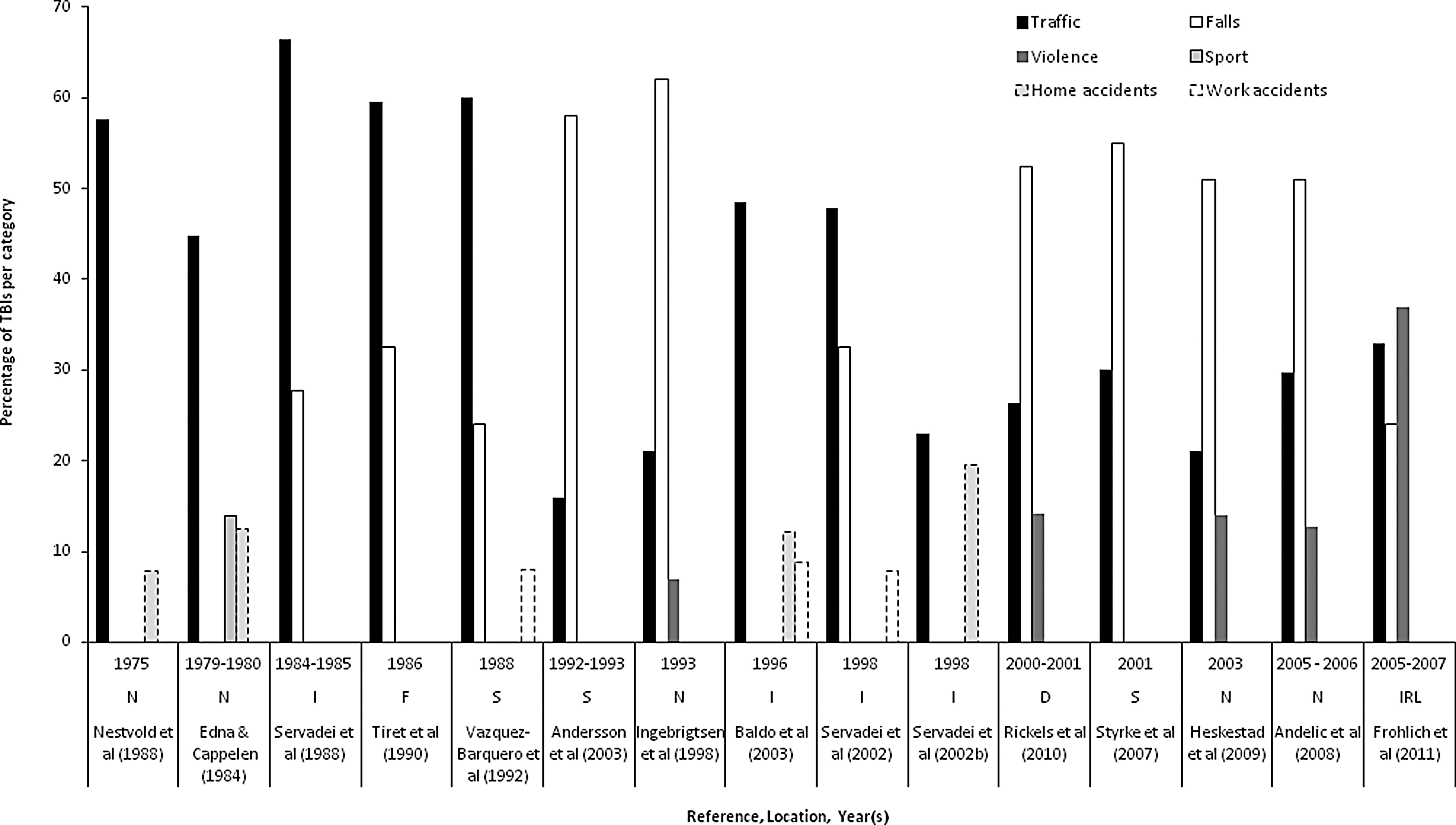
The most common mechanisms of injury in regional-level studies.
These seven distinct injury mechanisms include traffic-related, falls, violence, sports-related, accidents in the home or at work, and suicides or suicide attempts. Some studies also reported “struck by object” as a separate mechanism 36,37 ; however, this is not reported in the graphs as it was felt that it may overlap with other more specific causes, such as violence, sports, or domestic accident. One study noted that the mechanism of “accidents in the home” may include instances of domestic violence. 38
Time trends
Although no formal test or meta-analysis has been carried out, it is possible to observe an apparent slight downwards trend in incidence of TBI over time, in both country-level (Fig. 2) and regional-level graphs (Fig. 3). However, if the highest outliers on each graph are ignored (Servadei and colleagues [1985] 28 and Servadei and colleagues [1988], 30 respectively), the reduction over time is much less apparent. There is little or no indication of a change over time in the mortality rates at either country- or regional-level.
When examining mechanisms, the proportion of TBIs caused by traffic collisions has been lower in recent years, and correspondingly there is an increase in the proportion of cases attributed to falls. This pattern appears in the studies of mechanisms of injury at a regional level. Country-level studies–which included all severities of injury and all age groups, and reported on mechanism of injury–number only four, and three of these describe overlapping time periods; it is not possible to make any inferences regarding time trends among this small sub-group.
Discussion
The aim of this work was to produce a comprehensive and up-to-date review of incidence, mortality, and mechanisms of TBI across Europe. In accordance with the geographical scope of the over-arching CENTER-TBI project, the aim of this study was to review TBI patterns in Europe. A wide range of rates of incidence and mortality were reported. For all ages, all TBI severity studies, the lowest reported crude incidence rate was 47.3 per 100,000 population per year; the highest was 849 per 100,000 population per year. The reported crude mortality rates ranged from 3.3 to 28.10 per 100,000 population per year. These rates are broadly similar to those seen in the 2006 review. 3 The most common mechanism of injury in studies within our review appears to be shifting in Europe from road traffic incidents to falls in more recent studies (Fig. 7 and Fig. 8).
Distribution of TBI in European populations is widely researched and presented in numerous published studies. However, it is difficult to produce informative comparisons of these presented data, as the studies vary greatly in TBI definition and case ascertainment methods. Comparison is also difficult due to the fact the reviewed data were not standardized. This should be improved in the future by standardized data collection and coding. 10 For the time being, it is important to make the best use the existing data, and we believe the systematic review presented here provides the most useful opportunity to compare results with those of Tagliaferri and colleagues published a decade ago 53 and Peeters and colleagues published recently. 13 The incidence is changing only slightly over time and it may be contributed by the reporting variations during the period under investigation..
The recently-published systematic review of traumatic brain injury in Europe–set up as an update to Tagliaferri and colleagues' 2006 review, 3 presenting data for the period 1990-2014–had broadly similar findings and conclusions to our review, (i.e., no decreasing trend of TBI incidence in Europe). This review, like ours, found large variations in inclusion criteria, case ascertainment and case definitions. The incidence of TBI is thus difficult to compare between included studies, as well as between this and other reviews. In Peeters and colleagues' report, the incidence of TBI ranged between 47.3 and 546 per 100,000 population per year. 13 Given our broader time scale (no time limit), we found an even larger range–the incidence range in combined country- and regional-level studies was 47.3 to 849 per 100,000 population per year.
While some countries may be seeing a reduction in TBI (or a subgroup of TBI) incidence, 39 –41 our review suggests that across the continent of Europe, mean incidence rates remain broadly the same as in the 2006 review. 3 These findings from Europe are similar to the incidence rates in the United States (180 to 250 per 100,000 population per year), 42 but considerably lower than in a recent study in New Zealand, which found an incidence in excess of 700 per 100,000 person-years. 43
Worldwide, TBI incidence may be increasing still due to the wider use of motor vehicles in low-middle income countries and an increase in falls among older people in high-income countries. 41,44
The main methodological weaknesses observed in studies included in our review concerned poor reporting of funding, ethical approval, and study design. Very few studies were performed well according to the MORE assessment criteria. This may be in part because of the differing objectives of the included studies (some set out to study incidence and/or mortality, but others focused on mechanisms). However, it might have been expected that more of the studies focusing on incidence would perform well on this checklist. This again highlights the need for standardization of definitions and reporting if published studies are to be more comparable and informative.
It is also important to note that in this systematic review, which set out to review the available studies from all of Europe, suitable nationally-representative data were only found for 13 countries. These countries were principally members of the EU, plus Switzerland and Norway. Given that the EU currently comprises 28 countries and Europe as a whole includes almost 50 countries, it is apparent that there is a lack of good quality data collection and publication in many states. This limits the completeness of any attempt to describe European TBI incidence and mortality.
The reported crude incidence rates in regional populations or hospital catchment areas were found to be slightly higher than national surveys. It may be that studies of smaller regions or in a few nominated hospitals were conducted there because that region or hospital contains a specialist center, to which TBI cases are more frequently referred. International transfers of patients are assumed to be rarer, so national incidence data may be more complete.
When regional data were examined in a funnel plot, publication bias appeared unlikely.
There was some variability in the way relevant scientific terms have been used in different studies. In this review, incidence is defined as the rate of TBIs recorded in the original studies per 100,000 population per year. Using this measure, the majority of included studies reported actual hospital admission rate of participating treatment centers (or all hospitals in case of country-level studies). This is a slightly different measure to population incidence, in which all cases would have been traced, rather than just those arriving in a hospital. Again this limits the completeness of this review and implies that true population incidences are likely to be higher than the rates reported here.
Although the lack of age-adjusted figures make it difficult to draw direct comparisons, certain trends can be observed. Mortality rates in studies, including TBIs of all severities, vary many-fold; however, there was little indication of a trend towards increase or decrease over time. Some studies stated that they excluded patients who were dead on arrival at hospital (e.g., Rusnak and colleagues [2007], Vazquez-Barquero and colleagues [1992]). 26,45 As such, mortality rates shown in national data, rather than hospital records, may present a more complete picture.
In every study reporting sex ratios, there are more male patients recorded as having TBI than female patients. This may reflect the fact that some of the major causes of TBI, such as traffic incidents, violence, and sporting injuries, are related to more male-dominated activities. But the proportion of men in TBI studies decreased with age. In studies of older patients, with more women, the prevailing mechanism of TBI in older cases is falls. 46 However, a lack of age-adjusted results makes it impossible to draw firm conclusions about any difference in sex distributions of TBI.
There appears to be a changing pattern of mechanisms of injury over time, as the number of TBIs occurring in traffic incidents reduces, and conversely the contribution of falls becomes relatively greater in recent studies. This trend already has been described in studies in high-income countries. 44 This may relate to improved road infrastructure and traffic discipline and therefore declining traffic-related TBI incidence, as well as demographic trend of population aging. Few studies have attempted to look at epidemiological causes “upstream” of the immediate injury event; however, alcohol is considered a possible risk factor contributing to traffic or personal violence incidents. 47 This topic warrants further investigation.
Strengths and limitations
This review follows contemporary best practice in systematic review methods, with a comprehensive search strategy specified a priori, and a clear indication of why studies were included or excluded. It is likely that this search strategy, which was re-run as close as possible to the time of publication, has captured the vast majority of relevant published results.
It is likely that the figures shown here represent a relatively complete picture of the existing research on the burden of TBI in Europe. It is possible that mild TBIs may be under-diagnosed when a patient is admitted with multiple trauma or other injuries in addition to TBI. However, it seems unlikely that many TBI sufferers would be treated at home without the attention of medical professionals. The legal requirements for recording of fatal traumatic injuries vary across Europe but are usually strict. The gradual acceptance of systematic classification of injuries, such as ICD 10, means that, especially in more recent studies, data can be easily sorted to analyze events such as TBI.
Many studies stated that their incidence rates excluded non-residents who suffered TBI in the area. Hence, it is possible that some cases may not have been normally resident in the population used as the denominator in incidence calculations, leading to a small bias toward increased rates in places such as holiday destinations.
In summarizing the studies of TBI here, all papers that include an incidence, mortality or case-fatality rate for TBI are presented, regardless of how the authors defined the actual injury. In recent studies the ICD 9 or 10 coding systems were widely used and specifically described; however, in older papers, there were several different non-standard descriptions used based on external signs of injury and/or assessment of brain function. Thus, it is possible that there will be some variability in those deemed eligible, which may reduce the relevance of comparisons between different papers. The same can be said for classifications according to severity, where GCS is now a widely-accepted standard but alternative classifications, such as duration of lost consciousness, have been used at times.
No attempts were made to identify or translate non-English language publications. This is a weakness and it is possible that some relevant studies have been omitted due to this.
No attempt was made to verify the methods used by different research groups to ascertain mechanism of injury. Whereas some events may be unlikely to be misclassified (e.g., a traffic accident will often be associated with police reports of the event), others may possibly be confused, such falls and (attempted) suicides. One paper mentioned the likelihood that some acts of inter-personal violence (i.e., domestic abuse) are sometimes recorded as home accidents. 38 Further, the different countries included at different time-points may also exhibit other characteristics that would affect the likelihood of a particular mechanism of injury (e.g., variation in the laws or conventions of driving certain classes of vehicle). Hence, no causal conclusions are drawn about changing mechanisms, but the general trend of reduction in the proportion of traffic-related injury is consistent with the findings of other recent research.
Conclusions and Recommendations
This review found that large variations of TBI incidence and mortality rates exist between different countries and populations. There is some evidence of a changing pattern of mechanisms over time, which may indicate success of previous public health initiatives to reduce traffic-related injuries, but also highlight the contemporary need to understand fall-related injuries, especially among the elderly. The higher rates observed in these studies present opportunities for public health policy and evidence-based clinical guidelines to reduce the suffering caused by this serious injury.
We have highlighted above the variable nature of the definitions of TBI, and the thresholds applied to classify such injuries as mild, moderate, or severe. We concur with other research groups (Maas and colleagues; Feigin and colleagues) 10,43 who have argued that the comparability of research outputs and the opportunities to exploit collaborative research can only benefit from improved levels of standardization of case ascertainment and definitions of grades of injury.
Footnotes
Acknowledgments
This study was funded by the European Union FP 7th Framework program (grant 602150).
Author Disclosure Statement
No competing financial interests exist.
Appendix 1. Database Search Algorithms and Key Words
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.