
Abstract
Although existing guidelines support the utilization of intracranial pressure (ICP) monitoring in patients with traumatic brain injury (TBI), the evidence suggesting benefit is limited. To evaluate the impact on outcome, we determined the relationship between ICP monitoring and mortality in centers participating in the American College of Surgeons Trauma Quality Improvement Program (TQIP). Data on 10,628 adults with severe TBI were derived from 155 TQIP centers over 2009–2011. Random-intercept multilevel modeling was used to evaluate the association between ICP monitoring and mortality after adjusting for important confounders. We evaluated this relationship at the patient level and at the institutional level. Overall mortality (n=3769) was 35%. Only 1874 (17.6%) patients underwent ICP monitoring, with a mortality of 32%. The adjusted odds ratio (OR) for mortality was 0.44 [95% confidence interval (CI), 0.31–0.63], when comparing patients with ICP monitoring to those without. It is plausible that patients receiving ICP monitoring were selected because of an anticipated favorable outcome. To overcome this limitation, we stratified hospitals into quartiles based on ICP monitoring utilization. Hospitals with higher rates of ICP monitoring use were associated with lower mortality: The adjusted OR of death was 0.52 (95% CI, 0.35–0.78) in the quartile of hospitals with highest use, compared to the lowest. ICP monitoring utilization rates explained only 9.9% of variation in mortality across centers. Results were comparable irrespective of the method of case-mix adjustment. In this observational study, ICP monitoring utilization was associated with lower mortality. However, variability in ICP monitoring rates contributed only modestly to variability in institutional mortality rates. Identifying other institutional practices that impact on mortality is an important area for future research.
Introduction
T
After the initial injury, mass lesions, an increase in brain-water content (edema), and an increase in blood volume, can result in rising pressure in the rigid skull, which may lead to brain tissue herniation, impaired cerebral perfusion, and, without intervention, further damage to the brain. 5 Among those who die from TBI, the majority die because of uncontrolled rise of intracranial pressure (ICP), mostly within the first 48 hours of injury. 6,7 After a severe TBI, efforts are focused on prevention of further damage through intensive monitoring and prompt intervention. In 1951, Guillaume and Janny first described continuous ICP monitoring using an electronic magnetic transducer to measure changes in ventricular fluid pressure. 8,9 Since then, invasive ICP monitoring has become an increasingly employed tool to care for patients with severe TBI and has been adopted as part of the Brain Trauma Foundation (BTF) guidelines for the management of severe TBI, based on indirect evidence in which observational studies linked increased ICP with worse outcomes. 10 –13
Despite its use, the effectiveness of ICP monitoring technology has not been well established. 9,12 Moreover, several recent studies examining the relationship between utilization of ICP monitors and outcome have questioned the benefit of ICP monitors in severe TBI. 14 –19 In practice, there appears to be a low level of confidence among clinicians that ICP monitoring confers a benefit to TBI patients. According to a survey of practicing neurosurgeons in Canada, only 20% are highly confident that the routine use of ICP in severe TBI improves outcome. 20 The increasing number of studies that challenge the benefit of invasive ICP monitoring and the limited confidence in its utility might explain the reported wide variability in the utilization of ICP monitoring across centers. 14,21,22 Further, this variability might, in part, account for wide differences in institutional TBI-related mortality. 23 –25
In this context, we conducted a retrospective cohort study using data derived from the American College of Surgeons (ACS) Trauma Quality Improvement Program (TQIP). The objectives of this study were to (1) determine the association between ICP monitoring and mortality after a severe TBI, (2) determine the association between rate of ICP monitoring at the institutional level and hospital TBI-related mortality, and (3) describe the extent and determinants of interhospital variation observed in TBI mortality.
Methods
Study design
This was an observational cohort study, with the exposure of interest being invasive ICP monitoring in patients with severe TBI. The main aim of this study was to examine the relationship between ICP monitoring and in-hospital mortality. We used two analytic approaches to assess this relationship. First, we used ICP monitoring as a patient-level variable to determine the association between ICP monitoring and mortality. Second, because it is plausible that physicians elected to place ICP monitors because of an anticipated favorable or unfavorable outcome and the likelihood of similar distribution of unmeasured confounders within hospitals, we defined a hospital-level ICP monitoring utilization rate and evaluated this factor as a determinant of hospital TBI-related mortality.
Data source
We used data derived from The ACS TQIP. The TQIP was created to provide an opportunity for trauma centers to compare their processes of care- and risk-adjusted outcomes with their peer centers. 26 As of late 2011, the TQIP includes 155 ACS-verified level I and II trauma centers across the United States and Canada. More than 100 patient and institutional variables are recorded by trained abstractors, including patient demographics, comorbid conditions, type and mechanism of injury, injury severity, prehospital and emergency department (ED) physiological variables, in-hospital procedures and complications, and outcome information, including in-hospital mortality and discharge disposition. 26 Reliability of the data is ensured through intensive training mechanisms for the abstractors and interrater reliability audits of the participating sites. 27
The inclusion criteria for entry into TQIP require at least one valid trauma International Statistical Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) code in the range of 800–959, excluding the late effects of trauma (905–909). 26 Although the ACS administers the program, the authors of this study are solely responsible for the analyses and conclusions presented here. The study was approved by the research ethics board of Sunnybrook Health Sciences Center (Toronto, Ontario, Canada).
Assembly of the study cohort
We identified patients 16 years of age or older, who were admitted between January 2009 and December 2011, to a TQIP hospital with an Abbreviated Injury Score (AIS) for the body region head≥3. For the purpose of this study, we selected those patients who met the BTF level II recommendation for ICP monitoring: those with an acute intracranial lesion and severe TBI [defined as a total Glasgow Coma Scale Score (GCS) in ED ≤8]. Exclusion criteria were as follows: other severe injuries (AIS>2) in any other body region, penetrating TBI, “nonsurvivable” TBI (head AIS=6), dead on arrival, and prior advanced directives to withhold life-sustaining interventions.
Identification of exposure
Patients undergoing ICP monitoring were identified by the presence of any one of the following ICD-9-CM procedure codes: 01.10 (insertion of catheter or probe for ICP monitoring); 01.16 (insertion of catheter or probe for monitoring partial pressure of brain oxygen); 01.17 (insertion of catheter or probe for monitoring brain temperature); or 02.2 (ventriculostomy).
Patient-level covariates
The following patient-level covariates were considered for inclusion into adjusted analyses: age; gender; race; comorbid illnesses; injury mechanism and severity; vital signs in the ED, including GCS motor and total scores; type of intracranial lesion; and insurance status. To identify acute intracranial lesions, we used the AIS predot codes (1998 version) that reflect injuries to the intracranial structures (Supplementary Appendix Table 1) (see online supplementary material at
Hospital-level covariates
To characterize hospital environment that might influence TBI process of care and outcome, we classified centers based on the following factors: volume of TBI patients per center during the study period (divided into quartiles); teaching status; number of hospital beds; hospital type (nonprofit vs. for profit); and ACS or state trauma center designation level.
Outcome measure
The primary endpoint for this study was the odds of in-hospital death after TBI.
Statistical analysis
We calculated standardized differences to compare baseline characteristics between those who underwent ICP monitoring and those who did not. 28,29 Standardized differences greater than 0.1 were considered meaningful. 28 Two random-intercept multilevel logistic regression models were used to examine the adjusted association of patient- and hospital-level variables with in-hospital mortality after accounting for clustering of patients within centers. The main exposure for the first model was ICP monitoring as a patient-level factor. For the second model, the hospital-specific ICP utilization rate (categorized into quartiles), as a hospital-level factor, was the main exposure. Random-intercept regression models are standard multivariable regression models that include an extra term to account for the random differences in TBI mortality between the various hospitals. Covariate selection for both models was performed using the change-in-estimate approach described by Mickey and Greenland. 30 The final models included patient- and hospital-level covariates (described below), in addition to clinically meaningful interaction terms that changed the estimate of the main exposure by>10% in either direction. We checked for multi-collinearity within each model using the tolerance statistic and variance inflation factor.
For both of the models, discrimination was estimated using the c-statistic, and calibration was assessed using observed-versus-predicted outcome plots. In addition, we used the squared Pearson correlation between the observed and expected outcomes to measure the proportion of explained variation by each model. 31
To quantify variability between hospitals in TBI mortality, we used the median odds ratio (MOR), instead of the intraclass correlation coefficient (ICC), because of the interpretational difficulty of ICC with multi-level logistic regression models.
32,33
The MOR corresponds to the median value obtained when comparing the adjusted odds of dying after TBI if the same patient was admitted to two different randomly selected hospitals.
32,33
It estimates unexplained heterogeneity across different hospitals after adjusting for patient-level covariates.
34
In contrast to the ICC, the MOR is statistically independent of the prevalence of the outcome of interest.
32
In addition, it is easy to interpret because its magnitude can be directly compared with the odds ratios (ORs) of the patient-level variables.
34
The proportion of interhospital variance in mortality that can be explained by hospital-specific ICP monitoring rate was calculated using the proportional change in variance (PCV).
35
PCV can be calculated as per the following equation:
where V1 is the interhospital variance in a multilevel model that lacks the ICP-monitoring rate as a hospital-level factor, and V2 is the interhospital variance in the same model after adding hospital-specific ICP-monitoring rate. 32,35
Multiple sensitivity analyses were performed and are detailed in the Supplementary Appendix (see online supplementary material at
All of the statistical analyses were performed using SAS software (version 9.3; SAS Institute, Cary, NC), and statistical significance was defined by a two-tailed p value<0.05.
Results
The study cohort consisted of 10,628 patients with severe TBI with an acute intracranial lesion who were admitted to 155 level I and II trauma centers across the United States and Canada between January 2009 and December 2011. Overall mortality (n=3769) was 35.5%. Only 1874 (17.6%) patients underwent ICP monitoring, with a mortality of 31.6%. Median time from ED presentation to ICP monitor insertion was 3.1 hours [interquartile range (IQR), 1.85–7.25]. In contrast to the patients managed without ICP monitoring, the ICP-monitored group were younger, presented with fewer comorbid illnesses, suffered more-severe TBIs (as measured by head AIS), and were more likely to have traumatic subarachnoid hemorrhage, compressed/absent basal cisterns, brainstem, cerebellar or intracerebral mass lesion, epidural hematoma, or subdural hematoma (Table 1). Conversely, patients managed without ICP monitors were more likely to have experienced fall-related injuries, presented with hypotension [systolic blood pressure (SBP)<90 mmHg], were without commercial insurance, and were cared for at nonteaching hospitals. There was no significant difference between the two groups in either the total or motor GCS scores in the ED (Table 1).
ICP, intracranial pressure; IQR, interquartile range; CVA, cerebrovascular accident; AIS, Abbreviated Injury Scale; SBP, systolic blood pressure; GCS, Glasgow Coma Scale; TBI, traumatic brain injury.
When the 155 hospitals were ranked into quartiles based on their rate of ICP monitoring, there was considerable interhospital variation in ICP monitoring, with a median utilization rate of 16% (IQR: 8–26%). This large variation was accompanied by differences in the patient and hospital characteristics across the four quartiles (Table 2). In quartile 4 (highest ICP monitoring rate), patients had more-severe injuries (as measured by head AIS) and presented with more comorbid illnesses. In contrast, nonteaching hospitals were more likely to be in quartiles 1 and 2. Overall mortality was 35.6% (n=910) in quartile 1, 38.2% (n=939) in quartile 2, 35.3% (n=1136) in quartile 3, and 32.7% (n=784) in quartile 4.
Strata range from the lowest rate of ICP monitoring (quartile 1) to the highest (quartile 4).
ICP, intracranial pressure; IQR, interquartile range; CVA, cerebrovascular accident; AIS, abbreviated injury scale; SBP, systolic blood pressure; GCS, Glasgow Coma Scale; TBI, traumatic brain injury.
Relationship between ICP monitoring and mortality at the patient level
We evaluated the association between ICP monitoring and in-hospital mortality at the patient level using a random-intercept multilevel model. Using this approach, ICP monitoring was associated with significantly lower odds of death [adjusted OR, 0.44; 95% confidence interval (CI), 0.31–0.63; p<0.0001). In addition, admission to a center with a higher volume of TBI patients, as opposed to a lower-volume center, was associated with lower mortality (p=0.01). By contrast, all of the following were associated with a higher risk of death: increasing age; fall-related injuries; a lower GCS motor score in ED; a higher head AIS; the presence of traumatic subarachnoid hemorrhage; intracerebral mass lesion; compressed/absent basal cisterns; brainstem/cerebellar lesion; hypotension on admission; and a number of comorbid illnesses, including coronary artery disease, renal failure requiring dialysis, cancer, and bleeding disorders (Table 3). When introducing interaction term between ICP monitoring and age, the association between ICP monitoring and lower mortality was more pronounced in patients ≤65 years of age (adjusted OR, 0.35; 95% CI, 0.23–0.54), as opposed to older patients (adjusted OR, 0.60; 95% CI, 0.44–0.83). No significant interaction was found between ICP monitoring and motor GCS score on admission (p=0.44).
ORs were estimated using a random-intercept multilevel model with ICP monitoring (patient-level variable) as the main exposure and in-hospital mortality as the outcome of interest.
ICP, intracranial pressure; OR, odds ratio; CI, confidence interval; IQR, interquartile range; CVA, cerebrovascular accident; AIS, Abbreviated Injury Scale; SBP, systolic blood pressure; GCS, Glasgow Coma Scale; NA, not applicable.
This regression model showed good discrimination (c-statistic, 0.86) and calibration (based on an observed-vs.-predicted plot) and explained 61.1% of the observed variation in mortality across patients.
Relationship between ICP monitoring and mortality at the hospital level
After adjustment for the patient- and hospital-level factors in a random-intercept multilevel model, there were significant differences in the mortality rate across quartiles (Fig. 1). Compared to the quartile with the lowest ICP monitoring rate (quartile 1), the adjusted OR of dying in the hospital after TBI was 0.52 (95% CI, 0.35–0.78) for quartile 4, 0.63 (95% CI, 0.43–0.93) for quartile 3, and 0.72 (95% CI, 0.48–1.06) for quartile 2. This regression model had good discrimination (c-statistic, 0.86) and good calibration (based on an observed-vs.-predicted plot) and explained 61.2% of the observed variation in TBI in-hospital mortality.
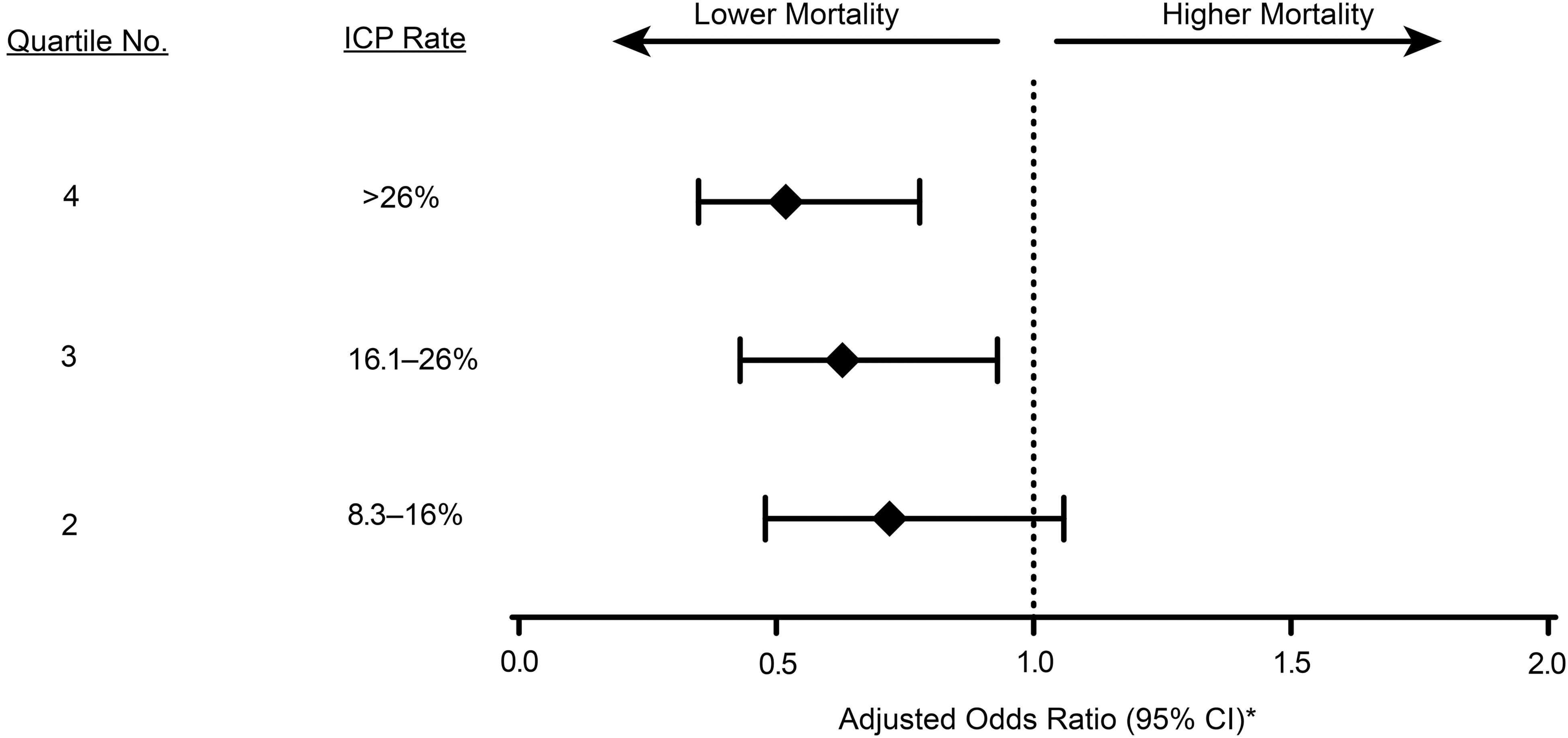
Forest plot of adjusted odds ratios (ORs) of death after severe traumatic brain injury at the different hospital quartiles of intracranial pressure (ICP) monitoring use. Quartile 4 has the highest rate of ICP monitoring and quartile 1 (the reference) has the lowest. Dotted line represents the odds of dying at the reference quartile (quartile 1). CI, confidence interval. *ORs were estimated using a random-intercept multilevel model with hospital-specific ICP monitoring rate (categorized into quartiles) as the main exposure and in-hospital mortality as the outcome of interest. Patient-level covariates were age, gender, comorbid illnesses, Glasgow Coma Scale motor score, Abbreviated Injury Scale score for body region head, hypotension on admission, type of intracranial lesion, mechanism of injury, and type of insurance. Hospital-level covariates were volume of traumatic brain injury patients per center, teaching status, and number of hospital beds.
The MOR for TBI in-hospital mortality across the various hospitals was 1.48. In other words, the median adjusted odds of dying after TBI were 1.48-fold greater if the same patient was admitted to one randomly selected hospital, as opposed to another. In a similar model that had the same patient- and hospital-level factors, but lacked the hospital-specific ICP monitoring rate, the proportional change in interhospital variance in TBI mortality, after adding the hospital-specific ICP monitoring rate (categorized into quartiles), was −9.89%, indicating that 9.89% of the interhospital variation in TBI mortality could be attributed to the hospital-specific ICP monitoring utilization rate. 35 Similarly, the volume of TBI patients per center could explain an additional 3.63% of this variation. However, this interhospital variation was not explained by hospital teaching status (p=0.97) or number of hospital beds (p=0.53).
Sensitivity analyses
Using a “doubly robust” inverse-probability-weighting estimator with a multi-level logistic regression model to predict mortality, the adjusted association between ICP monitoring and lower mortality was also significant (adjusted OR, 0.50; 95% CI, 0.43–0.59; p=< 0.0001). Within each hospital quartile of ICP use, our findings were consistent with both the overall patient-level associations and quartile-adjusted associations. More details regarding these sensitivity analyses are provided in the Supplementary Appendix (see online supplementary material at
Discussion
In the field of neurotrauma and critical care, invasive ICP monitoring has long been considered a standard of care for severe TBI patients without being supported by rigorous assessment of its effectiveness in improving outcomes. 38 In our study, we demonstrated a strong association between ICP monitoring and a lower risk of death after severe TBI. This finding was consistent when we examined the effectiveness of this technology at either the patient or hospital level. Further, there appeared to be a dose-response, with higher rates of ICP monitoring associated with lower rates of mortality, lending further credence to a causal relationship.
Accurate, continuous ICP monitoring by an invasive tool can lead to the prompt recognition of spiking pressure around the injured parts of the brain. 5 Such recognition could potentially lead to timely intervention that is able to control the rising pressure inside the rigid skull, a process that is thought to be the leading cause of death among severe TBI victims, especially during the first 48 hours after injury. 6,7 Despite the plausibility of its efficacy in guiding us to provide better care, many have questioned its effectiveness based on several studies that failed to provide conclusive, consistent results. This inconsistency among previous studies might explain the wide variability in ICP monitoring utilization across different hospitals. 22 Our findings agree with a number of previous studies that support the value of ICP monitoring in TBI, 22,39 but contrast with several studies that either failed to show an association between ICP monitoring and better outcomes, 14,15,17,19,40,41 or showed an association between ICP monitoring and higher mortality. 18 However, previous observational studies in this area have generally suffered from several limitations, including small sample size, a lack of or inadequate adjustment for multiple important confounders, and selection bias. 42 –44 In addition, the clustering of TBI management strategies at different hospitals is expected and would potentially lead to a clustering of patient outcomes. Accounting for such clustering during statistical analysis in TBI studies, including ICP monitoring studies, is commonly overlooked. 15,18,19,21,23 The only randomized trial in this area showed no difference in the primary outcome, a composite measure based on performance across 21 measures of functional and cognitive status, between care focused on maintaining ICP at 20 mmHg or less and care based on imaging and clinical examination in the setting of the developing world, where ICP monitoring is very rarely used. 41 However, the trial was not sufficiently powered to detect a mortality difference between both groups. 41 In addition, differences in injury characteristics, prehospital, intensive care unit (ICU) and post-ICU structure and processes of care, and the observation of “delayed mortality” due to medical complications, accounting for more than one third of deaths subsequent to TBI in Latin America, may render as questionable any extrapolation of epidemiologic or treatment studies from the developing to developed world. 45
In our study, we found considerable unexplained variation in hospital mortality, even after accounting for measured patient- and hospital-level characteristics. Moreover, our data were derived from verified trauma centers that have interest in high-quality care by virtue of their participation in TQIP and quality improvement activities. For that reason, study hospitals may have lower mortality rates than hospitals not participating, and we may have underestimated the extent to which in-hospital mortality varies across hospitals. Upon examining the determinants of this variation, we found that the utilization rate of ICP monitoring explained only 9.89% of the interhospital variation in severe TBI mortality. Albeit to a smaller extent, volume of TBI patient per center was another determinant of this variation. Other factors that might further explain interhospital variation in TBI mortality and were not examined in our study include variations in community or institutional approach toward withdrawal of life-sustaining therapy. 45 Identifying other institutional practices that affect mortality is an important area for future research.
This is the largest study of ICP monitoring in TBI to date. The strengths of the study include the broad selection criteria, adjustment for multiple important confounders, and the fact that the hierarchical structure of the data was taken into account during the statistical analysis. However, our results should be interpreted with caution. Our findings are limited mainly by the retrospective nature of the data, which do not include information about all potential confounders. For example, we lacked information about pupillary abnormalities that are known to be strong predictors of poor outcome after TBI. However, recent evidence suggests that ICP-monitored patients are more likely to have pupillary abnormalities than those patients managed without invasive ICP monitoring. 14 Therefore, we do not expect that accounting for pupillary reactivity will change the direction of observed association. In addition to the patient characteristics, the decision to insert an ICP monitor in a TBI patient involves multiple considerations, including physician judgment, the course of the patient during the hospital stay, and the availability of trained staff. These nuances are not measured in our data, although we attempted to adjust for measured confounders, in addition to adding an extra term to account for the random differences in TBI mortality between different hospitals using a random-intercept multilevel model with ICP monitoring as a patient-level variable, we repeated the analysis with ICP monitoring rate as a hospital-level factor, and we used propensity score (representing the probability that patients would be selected for ICP monitoring) methods to reduce selection bias. Each of these analytic approaches provided results that support the benefit of utilizing ICP monitoring technology in severe TBI.
In studies of TBI mortality, the ideal outcome measure would include deaths after acute care hospitalization. However, previous studies have shown that TBI-related death after hospital discharge is uncommon. 47 –49 In a population-based cohort study of hospitalized TBI patients who were discharged alive, approximately 92% of those patients were alive at 15 months after discharge. 50 Among post-discharge deaths, only 17% were TBI related. 50 Limited by our database, we could not assess the relationship between ICP monitoring and other important outcome measures, including long-term functional and quality-of-life outcomes. Future studies are required to examine these important relationships.
Until further observational studies with rigorous adjustment for potential confounding factors or more randomized trials become available, we recommend wider utilization of ICP monitoring technology in the management of patients with severe TBI and abnormal computed tomography (CT) findings to better inform medical decisions and guide more prompt interventions.
Conclusion
In the largest study to date of ICP monitoring in severe TBI, the utilization of such technology was associated with lower in-hospital mortality, suggesting that wider utilization of ICP monitoring is warranted. However, variability in ICP monitoring rates contributed only modestly to interhospital variability in TBI mortality. Identifying other institutional practices that impact on mortality is an important area for future research.
Footnotes
Acknowledgment
This work was supported, in part, by funds from the Physicians' Services Inc. Foundation (to A.S.A.) and a Canada Research Chair Program in Systems of Trauma Care (to A.B.N.). R.A.F. was supported by a Heart and Stroke Foundation Clinician Scientist Award. D.C.S. was supported by a New Investigator Award from the Canadian Institutes of Health Research.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.