
Abstract
The prevalence of cardiovascular disease (CVD) has increased in South Africa, emphasizing the importance of prevention strategies. This study used echocardiography to investigate the impact of Rooibos on cardiovascular function in those at risk of CVD. This research aims to contribute to understanding its effects on reducing cardiovascular risk factors. The study design involved a 12-week randomized, parallel, double-blinded, placebo-controlled dietary intervention trial using capsules containing standardized water-soluble extracts of green and traditional fermented Rooibos alongside a placebo control. Echocardiography was incorporated as a diagnostic imaging tool to assess cardiac function in the participant cohort. Aorta (AO) dimensions showed no significant change in any intervention group. Left atrium (LA) reduced in size from 3.832 ± 0.071 cm to 3.675 ± 0.067 cm (P = 0.01). There was no significant change in LA/AO ratio in any intervention group. Interventricular septum diameter in the placebo group decreased from 1.334 ± 0.030 cm to 1.250 ± 0.025 cm (P = 0.002), with no significance in fermented Rooibos, while green Rooibos resulted in a decrease from 1.282 ± 0.036 cm to 1.186 ± 0.029 cm (P = 0.002). Left ventricle posterior wall (LVPW) showed no significant changes in any of the intervention group. The left ventricle mass in the placebo and green Rooibos groups demonstrated no significance changes, while fermented Rooibos caused a decrease from 204.102 ± 7.102 g to 191.394 ± 6.707 g (P = 0.015). The phytochemical bioactive components, such as the polyphenolic antioxidants present in green and fermented Rooibos, improved cardiovascular function. This study confirms the effectiveness of echocardiography as imaging tool for assessing cardiac function in this particular population. Regular Rooibos consumption may offer promising therapeutic benefits for preventing and managing CVD risk.
INTRODUCTION
Cardiovascular disease (CVD) has significantly increased in South Africa over the years, and early management is crucial to lessen the morbidity to individuals and the cost burden to our healthcare system. 1 CVD is the leading category of noncommunicable diseases (NCDs) according to Pillay et al. (2016), 2 and the mortality rate for NCDs in South Africa has now surpassed those of HIV/AIDS and tuberculosis. 3 Smith and Swart (2018) 4 agree with this statement made by Pillay et al. (2016) 2 and note that CVD is widely studied, constitutes a range of chronic diseases, and is currently the most common noncommunicable disease. According to Nojilana et al. (2016), 3 the age-standardized death rates (ASDRs) from cerebrovascular disease, hypertensive heart disease, diabetes mellitus, ischemic heart disease (IHD), and cardiomyopathy were relatively high among black Africans.
The field of echocardiography has expanded rapidly in recent years, allowing for a detailed assessment of cardiac function. Improved technology has enhanced image quality, making echocardiography increasingly valuable in emergency, surgical, and critical care departments. 5,6 According to Tendera and Wojakowski (2015), 7 all patients should have a resting transthoracic echocardiogram at the time of initial presentation with CVD systems, as it eliminates other possible causes of chest discomfort. Chang et al. (2009) 8 and Yildiz et al. (2020) 9 suggest that two-dimensional (2D) echocardiography is still the most widely utilized imaging modality for assessing the heart.
Native to South Africa, Rooibos (Aspalathus linearis), grown exclusively in the Cederberg region of the Western Cape Province of South Africa and enjoyed by millions of households, has gained popularity worldwide and is on track to become the second most commonly consumed beverage. 10,11 In addition to Rooibos being caffeine free, it also has lower levels of tannins compared to the Camellia sinensis teas and is rich in unique phytochemical constituents with various bioactivities, including redox modulation, antioxidant, and anti-inflammatory activities. 12 –14 These characteristics make Rooibos a potentially promising candidate to impact CVD prevention through dietary interventions. Previous studies have reported the ability of tea to modulate risk factors associated with CVD. 15 –17 The mentioned studies highlight the potential of green tea extract as a natural and supportive approach to managing cardiovascular health. These dietary flavonoids have been found to decrease the risk of death due to coronary artery disease, cancer, and stroke, likely due to their antioxidant protection in the vascular endothelium and ability to reduce the risk of atherosclerosis. 18
Oxidative stress, caused by an imbalance of free radicals and antioxidants in the body, contributes to cell and tissue damage and the development of chronic diseases. 19 Herbal teas, rich in antioxidants such as flavanols, flavanones and isoflavanones, can potentially increase antioxidant levels in the blood and prevent chronic illnesses. 20 Duffy et al. (2001) 21 studied the effect of long-term black tea consumption on endothelial dysfunction and found that certain antioxidants in black tea can be linked to a reversal in endothelial dysfunction in participants with coronary artery disease. Previously, it was shown that the chronic intake of fermented Rooibos improved the lipid profile, enhanced the redox status, and reduced the oxidative lipid damage in adults at risk for developing CVD. 13 This study aims to contribute to this and further our understanding of its effects on cardiovascular health by using echocardiography.
Study design
The echocardiography study was part of a larger research project titled “Rooibos, Heart and Cognitive Health,” which aimed to investigate the potential cardiovascular and cognitive benefits of Rooibos. Echocardiography was included after discussing its potential as a diagnostic tool for cardiac abnormalities in the at-risk participant cohort. The study involved a 12-week randomized, placebo-controlled parallel dietary intervention trial. Participants were randomly assigned to one of three intervention groups consuming placebo, fermented Rooibos, or green Rooibos capsules. The capsules contained standardized cold water-soluble extracts manufactured by Rooibos Ltd. under Good Manufacturing Practices certification and packaged in a registered Food and Drug Administration facility. Participants took one capsule three times a day with meals for 12 weeks, with each capsule equivalent to three cups of Rooibos. The groups were matched based on age and gender, and the researcher was blinded to which capsules each participant consumed. Before starting the intervention, participants had a 2-week washout/stabilization period where they followed their normal diet with certain dietary flavonoid restrictions. Transthoracic echocardiography was done before and after the 12-week intervention. Participants were requested to follow their usual diet, while compliance was monitored from completed daily dietary records and return of capsule holders at the end of the study.
Study population
Participants for the study were recruited from a screening program conducted at the Applied Microbial and Health Biotechnology Institute, at the Bellville campus of the Cape Peninsula University of Technology (CPUT) in Cape Town, South Africa. The Human Research Ethics Committee of the Faculty of Health and Wellness Sciences at the university approved the study (CPUT HWS-REC 2021/H29 renewal). All participants attended an information session where the study criteria were explained, and the researcher described the procedures regarding the participant’s involvement in the study. Potential volunteers were first requested to complete a screening questionnaire based on the following inclusive criteria: hyperlipidemia—raised cholesterol levels of >5.5 to 7.5 mmol/L and triglyceride levels of >1.7 to <2.5 mmol/L, hypertension—increased blood pressure readings of >120–139/80–90 mmHg, hyperglycemia—elevated blood glucose levels, and lifestyle factors, which include a body mass index of > 25 to 38 kg/m2, classified as overweight or obese, physically inactive, and following a high atherogenic diet.
The study participants each provided written consent before the study commenced and were advised that they may withdraw from the study at any moment without prejudice or detrimental influence. This study adheres to the Protection of Personal Information Act that went into effect on July 1, 2021, in South Africa, intending to govern the processing of personal information during research. Each participant was assigned a unique study code that was used on all research-related data and documents for each participant to ensure the confidentiality of all information collected in this study.
A total of 721 adults between 28 and 79 years of age participated in a screening program. From the screening, 413 adults who met the study’s inclusion criteria were invited to attend information sessions about the study. 257 participants completed the baseline phase. Finally, while 219 participants completed the full 12-week Rooibos intervention phase and were included in the study. The participants had two or more modifiable CVD risks.
Transthoracic echocardiography
Transthoracic echocardiography measurements were performed with an E2 Series Digital Color Doppler Ultrasound system with Brightness mode, Motion mode (M-Mode), and Doppler facilities (color, pulsed-wave, and continuous-wave Doppler). The ultrasound system is manufactured by SonoScape Medical Corporation based in China. A 2–8 MHz multifrequency phased array transducer with coupling gel was used to assess the cardiac structures. Echocardiography was performed by an experienced sonographer who was blinded to the intervention cohort and clinical data of the participants. The scanning was conducted according to the recommendations of the American Society of Echocardiography. The systolic and diastolic cardiac functions were obtained from the 2D and M-mode imaging applications. Using the parasternal long-axis view and short-axis view, the left ventricle in diastole diameter (LVIDd) and the left ventricle in systole diameter (LVISd) measurements were obtained, as well as the interventricular septum thickness in diastole diameter and the left ventricle posterior wall diameter (LVPWd) thickness. The right ventricle (RV), aorta (AO), and left atrium (LA) sizes were determined using the parasternal long-axis and the four-chamber views to determine the right atrial size. The pulmonary arterial pressure was estimated by measuring the RV systolic pressure using tricuspid valve regurgitation velocities. The diastolic function and the mitral valve inflow pattern were detected using the pulse-wave Doppler application. Data analysis was done offline using the customized ultrasound software.
The echocardiograms were conducted in a safe and secluded environment, with only authorized personnel who provided medical assistance when necessary. Recordings were automatically saved on the system that was stored in a closed and protected room. Permission was granted to the researcher to utilize the echocardiographic images of participants in this document, respecting their privacy and anonymity. Figure 1 demonstrates the systolic and diastolic measurements of the cardiac structures, and Figure 2 demonstrates the pulse-wave spectral Doppler to assess the diastolic function of the heart.
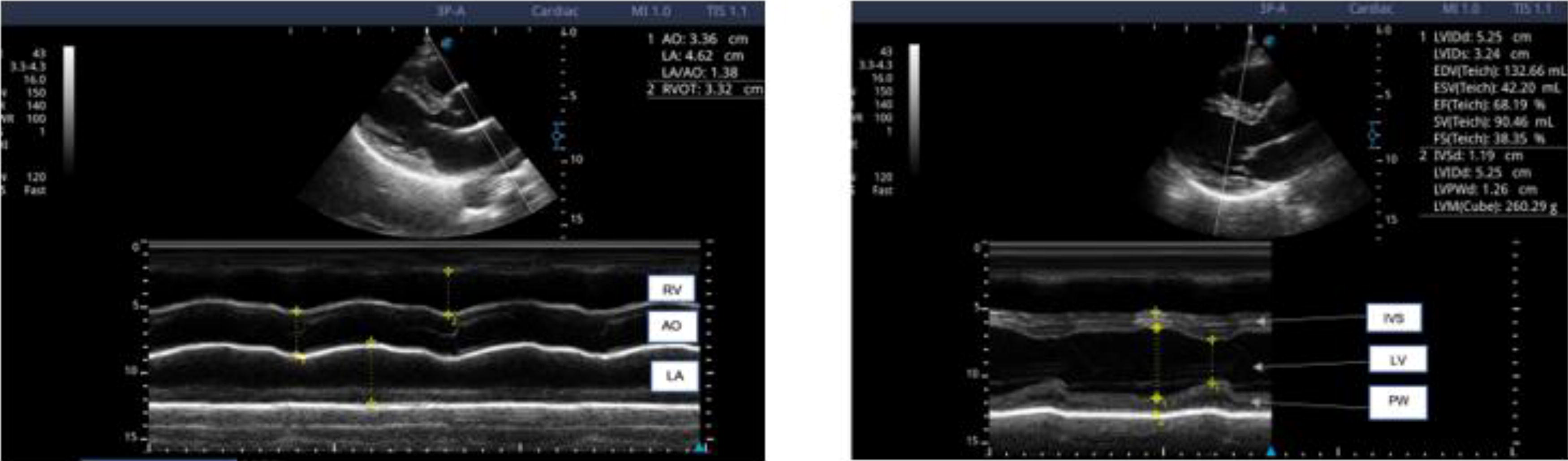
Parasternal long-axis Motion mode measurements of the right ventricle (RV), aorta (AO), left atrium (LA), interventricular septum in diastole (IVSID), left ventricle in diastole (LVIDd), left ventricle in systole (LVISd), and posterior wall (PW).
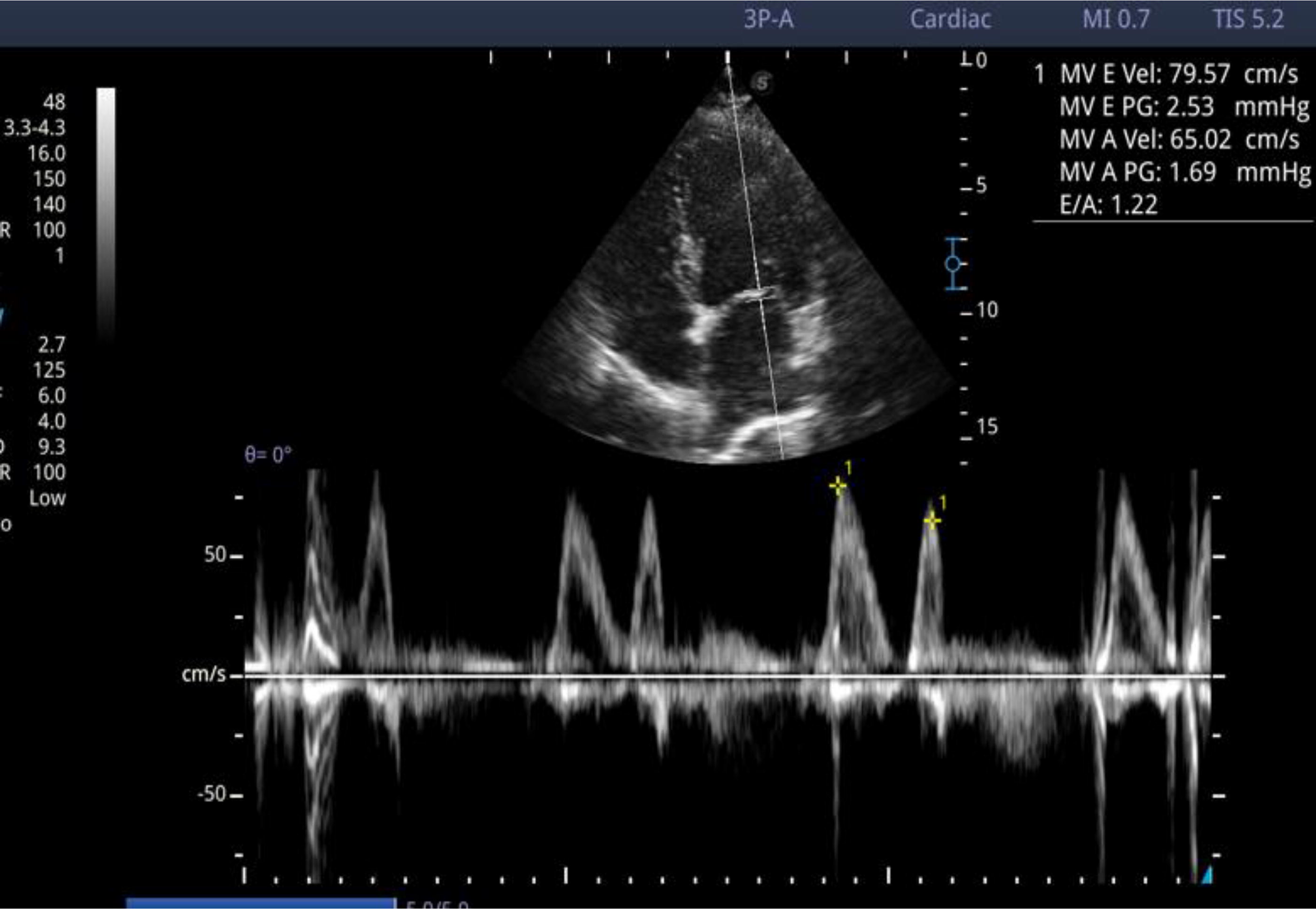
Apical four-chamber view demonstrating pulse-wave (PW) spectral Doppler to assess the diastolic function of the heart.
Parasternal long-axis view M-mode measurements of the RV, AO, LA, interventricular septum in diastole, LVIDd, LVISd, posterior wall (PW).
Apical four-chamber view demonstrating pulse wave spectral Doppler to assess the diastolic function of the heart.
Statistical analysis
The generalized linear model consists of three components: a random component, a systematic component, and a link function.
22
The assumptions of the classical linear model, as outlined by McCullagh and Nelder (1989),
22
are as follows: All components of Y, the dependent variable, are independent and normally distributed, and they all have common variance (random component), The covariates are combined to give the linear predictor (systematic component), Relationship between the random component and the systematic component is described using a link function, which follows a specific probability distribution, according to the characteristics of the dependent variable.
The generalized linear model relaxes the first assumption to allow dependent values that may be from one of the exponential family of distributions and to allow variances that are not common. Link functions are chosen according to the data type and the context of the data.
In the case of repeated (dependent) measures, the generalized linear model can be extended to the generalized estimating equation application.
23
This application allows for the dependent variable to be numerical or categorical. In this study, the dependent variable is a binary variable; thus, a logit link function
RESULTS
The anthropometric and general health characteristics of the study population are presented in Table 1.
Anthropometric Characteristics of the Study Participants (n = 219)
n, total number; kg, kilogram; m, meter; kg/m2, kilogram per square meter; mmHg, millimeters of mercury; g/dL, grams per deciliter.
Echocardiography outcomes
Based on the generalized estimating equation application demonstrated in Table 2, no significant effect of the three study interventions was observed for the AO, LVPWd, LVISd, LVIDd, and EF%; however, some of the interventions did affect the LA, IVSd, and left ventricular mass (LVM) measurements. This analysis demonstrated that both the green Rooibos and fermented Rooibos interventions had a discernible impact on cardiovascular function. It is noted that the placebo group also exhibited changes in one of the cardiovascular function parameters.
Effect of the Three Study Interventions on the Measured Echocardiography Variables
AO, aorta; LA, left atrium; IVSd, interventricular septum diameter; LVPWd, left ventricle mass; LVM, left ventricular mass; LVPWd, left ventricle posterior wall diameter; LVIDd, left ventricle in diastole diameter; LVISd, left ventricle in systole diameter; EF, ejection fraction.
Furthermore, when considering the association between echocardiography measurements and the three distinct dietary interventions, Chi-square tests were conducted to evaluate statistical significance. These tests provided evidence that the various interventions did, indeed, influence specific cardiac variables, including the LA, interventricular septal thickness in diastole (IVSd), and LVM.
The green Rooibos group demonstrated a slight reduction in the aortic size from the baseline to the intervention echocardiogram. This change was, however, not statistically significant (P = 0.75). The fermented Rooibos (P = 0.57) and placebo (P = 0.25) groups exhibited increased AO dimensions, which did not reach statistical significance. In LA dimensions, a significant reduction (
DISCUSSION
Fermented and green Rooibos interventions positively impacted cardiovascular parameters (Table 2). A significant reduction was demonstrated in LA dimensions and the interventricular septum thickness in the green Rooibos group, while fermented Rooibos showed a decreasing trend without statistical significance. Both groups exhibited nonsignificant positive changes in aortic dimensions. Fermented Rooibos, however, resulted in a significant decrease in left ventricular mass, which was not observed in the green Rooibos, suggesting a role for fermented Rooibos in cardiac remodeling and function enhancement. These differences may stem from variations in the bioactive compounds present in fermented versus green Rooibos, suggesting potential specific benefits of each preparation on cardiac parameters. These findings also imply that the bioactive compounds in fermented and green Rooibos may contribute to these cardiovascular benefits. A cross-sectional analysis by Senftinger et al. (2023) 25 investigated the associations between coffee consumption and various cardiac biomarkers, echocardiographic and electrocardiographic parameters, and found that different levels of coffee consumption did not show significant correlations with the investigated electrocardiogram, echocardiogram, or the prevalent CVD. However, they observed a positive correlation between high coffee consumption, elevated LDL cholesterol levels, and lower systolic and diastolic blood pressure. Dömötör et al. (2015) 26 found that the consumption of coffee did not affect cardiovascular function.
Uncontrolled hypertension (HPT) can have detrimental effects on the LV, leading to left ventricle hypertrophy (LVH), and poses a risk to the systolic function, potentially resulting in heart failure, arrhythmia, and even sudden death if not treated. 27 Authors Yue et al. (2007) and Palmieri et al. (2008) 28,29 note that diastolic and systolic dysfunction, LVH, myocardial interstitial fibrosis, increased apoptosis, and oxidative stress upregulation are common diagnoses in diabetic hearts. Huynh et al. (2014) and Shabab et al. (2021) 30,31 agree and note that dilated cardiomyopathy, systolic and diastolic dysfunction, are influenced by several variables, including the oxidative stress process, inflammation, cell death, fibrosis, and hypertrophy. A dilated aortic root effectively indicates increased cardiovascular risk related to target organ injury. 32 This statement is confirmed by (Lee and Park (2015) and Eshoo et al. (2009), 33,34 who state that increased LV mass, reduced LV systolic performance, impaired LV diastolic function, and increased left atrial size are all indicators of poor prognosis linked with hypertension. Suzuki et al. (2011), Boyd et al. (2013), and Dreslinski et al. (1981) 35 –37 documented that HPT causes LVH, decreased LV diastolic function, and LA enlargement.
The results from this study indicated that echocardiography is an effective imaging modality to assess the heart, to exclude CVD in this cohort. The 12-week Rooibos intervention was found to be effective in modulating the cardiovascular function of participants in this research study, which demonstrated a decrease in the AO size, a decrease in the LA size, a decrease in IVS thickness, and a decrease in the LVM. Most of the significant corrections and improvements of the echocardiography parameters in the cardiac function have been observed in the green Rooibos intervention group. The findings in this study agree with previous studies that theorized how the bioactive compounds present in herbals such as green tea, particularly the polyphenolic constituents, can potentially improve cardiovascular health. 38 –42 In addition to having cardiac protective benefits, a study by Afzal et al. (2015) 40 also suggests that green tea has been linked to possessing antitumor, anti-Alzheimer, and antiaging properties, as well as the potential to enhance redox status at the tissue level.
CONCLUSION
This is the first study to report on the possible heart health benefits of Rooibos, specifically using echocardiography, and as such, it provides an important basis for the design of future studies of this nature. The findings of this study align with previous research that has highlighted the potential benefit of Rooibos in influencing CVD. The results also confirm that echocardiography is an effective tool for assessing the heart of participants at risk of CVD. Bioactive compounds in Rooibos play a significant role in improving cardiovascular function, and it is suggested that daily consumption of Rooibos could be a valuable dietary source for antioxidants and other bioactives to include in your daily health regime for improving cardiovascular function. Further research is required to understand the precise mechanisms in both fermented and green Rooibos.
Footnotes
ACKNOWLEDGMENTS
The authors thank the study researchers and Applied Microbial and Health Biotechnology Institute staff for contributing to this study.
AUTHOR DISCLOSURE STATEMENT
The authors have nothing to declare and are responsible for the content and writing of this article.
FUNDING INFORMATION
The South African Rooibos Council (SARC) and the Cape Peninsula University of Technology (CPUT) Department of Higher Education (DHET) Prestigious awards; University Capacity Development Grant (UCDP), and Improvement of Qualifications Program (IQP).