
Abstract
This study evaluated the effects of consumption of hydrolyzed water-soluble egg membrane (WSEM) on joint function in an otherwise healthy population experiencing chronic pain. A randomized, double-blind, placebo-controlled crossover study included two 4-week periods of placebo and WSEM consumption, separated by a 4-week washout period. Twenty-five study participants were randomized to either the “placebo-first” or “WSEM first” sequence in the crossover trial, and 22 participants completed the study requirements. Range of motion (ROM) was assessed using digital inclinometry for joints associated with vertical weight bearing from neck to knees and for shoulders. Pain at rest and when physically active was scored for the same anatomical areas using visual analog scales (VAS). Physical functioning was tracked using questionnaires with VAS. Consumption of WSEM was associated with improved ROM for neck, spine, hips, and knees, with ROM for the neck and right knee being significantly improved during WSEM consumption compared to placebo (P < .05). ROM improvement for the dominant shoulder was highly significant during WSEM consumption (P < .01). Physical activity levels were significantly higher after WSEM than after placebo consumption (P < .05). Many aspects of physical functioning as part of daily living improved. Subgroup analysis showed rapid improvement of lower back pain after 5 days of WSEM consumption compared to placebo consumption (P < .05) in subjects who participated in the study during the winter season. Daily consumption of 450 mg WSEM was associated with improved joint function, comfort during daily activities, and increased physical activity.
Introduction
A
Components and actions of chicken EM have been researched for decades for numerous industrial applications. Recent research has focused on its ability to perform as an extracellular matrix environment, nerve guide channels in peripheral nerve regeneration, 5 nutrient delivery systems, 6 and other biotechnical uses. However, the mechanisms by which EM supports tissue repairs have not yet been determined. Further evaluation is needed to determine EM's ability to support specific regenerative processes, in comparison with known factors that promote regeneration. Currently, the literature on EM falls into at least three categories based on the type of EM: crude/native, enzymatically digested, or hydrolyzed water-soluble material. It is important to scrutinize which material is used when evaluating data.
An EM-based dietary supplement containing glycosaminoglycans and essential proteins was found to be a successful treatment for pain and inflexibility caused by joint and connective tissue disorders in several clinical studies. In an initial open-label clinical study, supplementation with crude EM significantly increased flexibility in 7 days and significantly reduced general- and range of motion (ROM)-associated pain in 30 days. 8 Crude EM has also been evaluated as a treatment option for osteoarthritis and was shown to significantly reduce joint pain and stiffness associated with knee osteoarthritis compared to placebo. 9 As osteoarthritis requires long-term treatment, the use of EM offers a potentially beneficial complementary intervention, as it does not result in the side effects associated with analgesics and nonsteroidal inflammatory drugs.
More recently, EM was suggested to be safe for human consumption as it did not exhibit cytotoxic, genotoxic, acute, or repeated-dose oral toxicity in a preliminary study. 10 In addition, EM has been documented to suppress production of proinflammatory cytokine production using an in vitro cellular model, suggesting future anti-inflammatory applications. 11 Of further interest, EM subjected to in vitro digestion was more effective in reducing production of the proinflammatory cytokine Tumor Necrosis Factor-Alpha than native EM when the cells were exposed to a mitogen. This provides support for the use of EM as a consumable anti-inflammatory supplement for the treatment of arthritic conditions.
The ability of hydrolyzed water-soluble EM (WSEM) to function as a surface for human dermal fibroblast adhesion in vitro was tested and showed that dermal fibroblasts adhered to a water-soluble alkaline-digested form of eggshell membrane conjugated to an artificial cell membrane biointerface. 12 As this scaffold has potential topical applications in wound healing, as well as deep-tissue applications such as stabilizing connective tissues, further study of WSEM was needed.
The controversy regarding whether orally delivered EM aids in regulating reparative mechanisms prompted the need for clinical documentation of effects associated with consumption of EM. Specifically, the documentation after consuming a WSEM hydrolyzate is an important step, due to the ease of delivery in multiple application systems associated with improving joint and connective tissue health. The effects of consuming WSEM were evaluated in a study population with osteoarthritis and showed significant reduction of C-reactive protein (CRP), as well as improved daily functioning (manuscript in preparation).
The clinical study reported here was conducted in a healthier study population and aimed at documenting whether consumption of hydrolyzed WSEM had clinically significant effects in relieving chronic pain associated with mild to moderate limitations to physical functioning. The study design aimed at collecting data on rapid effects as well as long-term observations.
Materials and Methods
Study design
A randomized, double-blind, placebo-controlled crossover study design was used for this clinical study. Twenty-five people went through screening and were enrolled in the 12-week study upon signing written informed consent, as approved by the Sky Lakes Institutional Review Board before the study started (Table 1). Exclusion criteria included the following: previous major gastrointestinal surgery, intensive athletic training; major trauma or surgery in the past 6 months; use of injectable corticosteroids or other injectable pain prescription medication within 6 months before randomization; use of prescription pain medications; daily consumption of over-the-counter pain medication; regular consumption of glucosamine, chondroitin, or hyaluronic acid; regular use of marijuana; active autoimmune disease; thyroid disease, inflammatory bowel disease or other active uncontrolled disease; diagnosis with fibromyalgia or chronic fatigue syndrome; severe degenerative musculoskeletal disease; cancer and/or chemotherapy during the last year; chronic viral infections; ongoing acute infections; currently experiencing asthma or taking asthma medications; frequent headaches, including migraines; currently taking antidepressant, antipsychotic, antianxiety and/or hypnotic medications; and currently on anti-inflammatory nutritional supplements judged by the study coordinator to negate or camouflage the effects of the test product.
Average ± standard deviation is shown.
BMI, body mass index; WSEM, water-soluble egg membrane.
Subjects were asked to maintain a constant intake of supplements over the time of the study. As documented by prescreening interviews, all study participants were on a normal diet (regular meals, no excessive consumption of sugar, soft drinks, or alcohol) and moderately active either by physical work or normal daily activities such as housework and gardening (no extreme athletes). Study participants were instructed to maintain their normal diet and lifestyle throughout the study. After a successful screening process, the participants were randomized to receive either product or placebo for the first 4-week phase of the crossover study. After the 4-week visit, they had a 4-week washout period, followed by a 4-week period of consuming the other test product. One set of study participants enrolled in November 2013 and completed the study in February 2014. Another set enrolled in January 2014 and completed the study in April 2014. The study was carried out in Southern Oregon (USA), where study participants live and work at an elevation of 1200–1500 m above sea level.
Consumables
The active consumable product BiovaFlex® (450 mg/day) and placebo were provided by Biova LLC (Johnston, IA, USA). The placebo capsules contained microcrystalline cellulose and were matched for appearance to the active capsules. The study participants were instructed to take one capsule in the morning. Adherence to the study protocol was evaluated at each visit by counting of returned capsules, interview with the study coordinator, and review of diary.
ROM using digital inclinometry
The evaluation of ROM was conducted in a detailed manner using the J-Tech Tracker Freedom dual digital inclinometry (J-Tech Medical, Midvale, UT, USA), where not only a person's major area of discomfort was evaluated but also the entire vertical weight-bearing axis of the body was studied, from the neck to the knees. In addition, shoulder ROM was also evaluated. The rationale behind this detailed assessment is that often a person's primary complaint (e.g., right hip) would lead to a compensated posture and compensated ROM of other anatomical areas as the person strived to put less pressure on a painful area, as previously described in studies for natural products. 13 –15
Questionnaires on activities of daily living
At each visit, difficulties pertaining to physical functioning were evaluated using a set of 12 questions pertaining to daily activities and scored using unmarked 100-mm visual analog scales (VAS).
Pain assessment
The pain assessments at each 4-week visit involved the scoring of pain levels in different areas of the body (neck, shoulders, upper and lower back, hips, knees) when at rest and when physically active, where the scores were measured using unmarked 100-mm VAS. In addition, the study participants also answered a similar pain questionnaire daily, during both of the 4-week consumption phases of the 12-week crossover study.
Statistical analysis
The number of subjects was determined by power calculations based on data from a preliminary open-label pilot study, and this study was 90% powered to detect a 10% change. Statistical significance of changes from baseline to later assessments was evaluated by between-treatment analysis using the two-tailed independent t-test. Within-subject analysis was performed using the two-tailed paired t-test. Statistical significance was indicated if P < .05. Subgroup analysis was performed for the group receiving placebo before WSEM, the subgroup receiving WSEM before placebo, and the two subgroups enrolled at different times of the year.
Results
Study demographics and compliance
The gender, age, and body mass index (BMI) were evenly distributed between the group receiving the active test product WSEM during the first 4-week consumption period (placebo during the second 4-week consumption period) and the group that received the products in reverse order (Table 1). The BMI range did not exceed 35 kg/m2, and the average BMI was below 30 kg/m2 for women and between 30 and 31 kg/m2 for men. The adherence to study protocol and compliance was good and slightly higher during the consumption of WSEM. Mean compliance with respect to product consumption was at or higher than 86% throughout the study (Table 2).
Study participants were randomized to either consume WSEM during weeks 1–4 and placebo during weeks 9–12 or consume products in the reverse order.
Range of motion
Results from the ROM evaluations showed significant between-treatment improvements in ROM for the cervical lateral motion as well as for the right knee, after study participants consumed WSEM, compared to the same people consuming placebo (Fig. 1). Using within-subject statistical analysis, highly significant improvements in ROM were seen for all three ROM measurements of the neck as well as for the dominant shoulder.
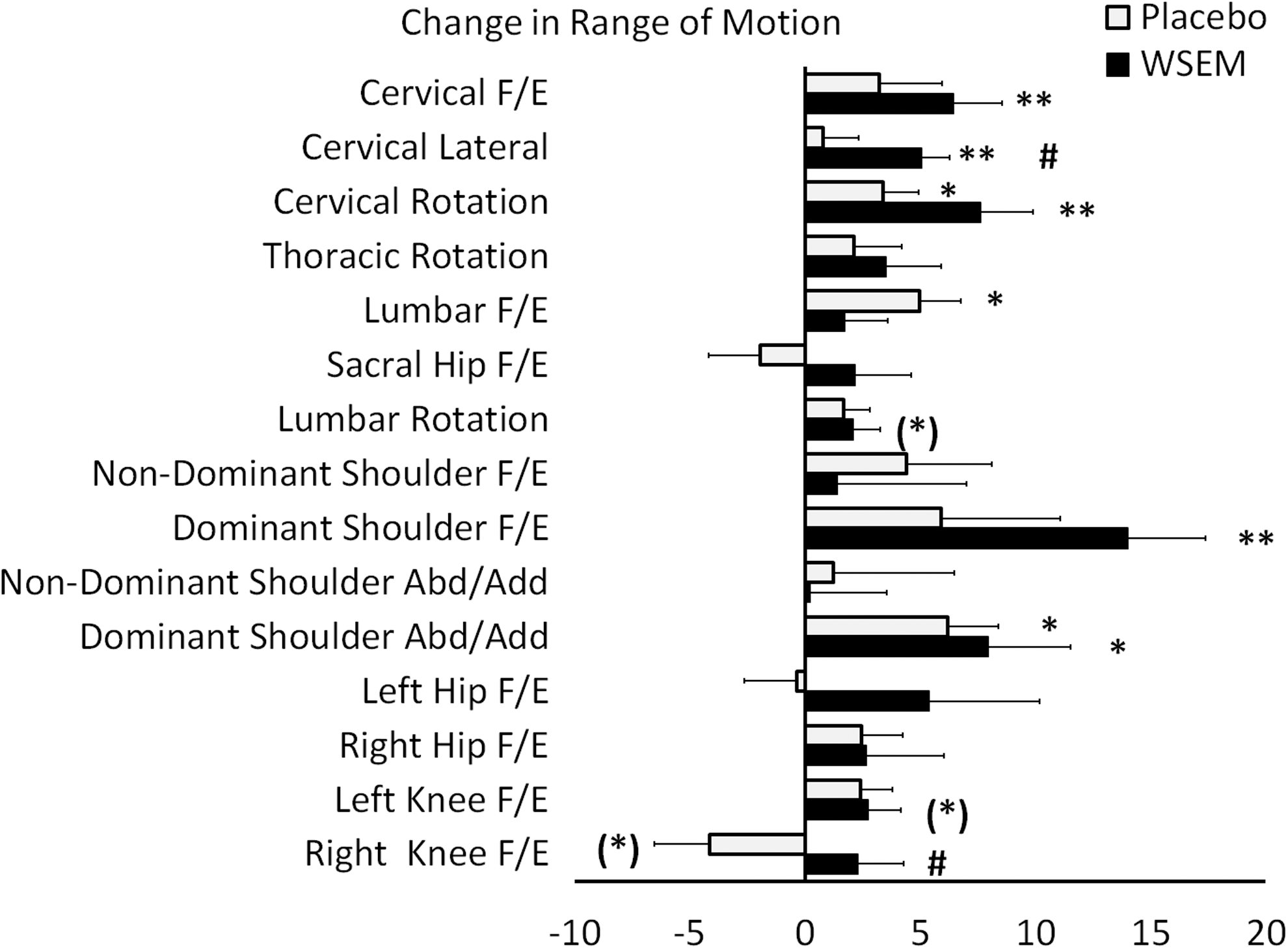
Range of motion (ROM) evaluation. The average % increase in ROM is shown for the changes during consumption of WSEM (black bars) and placebo (gray bars). The data graph shows the average ROM change ± SEM. Statistical significance using between-treatment analysis is indicated by hash marks (# P < .05), and statistical significance using within-subject analysis is shown by asterisks ((*) P < .1, *P < .05, **P < .01). Abd, abduction; Add, adduction; F/E, flexion/extension; WSEM, water-soluble egg membrane.
Improved ability to perform daily activities
The level of difficulties of physical functioning associated with performing daily activities was scored at each visit during the study (Fig. 2). The level of difficulty for each task was scored at the beginning and end of each 4-week consumption period, separated by the 4-week washout period. After consuming WSEM, subjects reported less difficulties in performing daily activities. There was no statistical significance using between-treatment analysis. Statistical significance using within-subject analysis showed significant improvements for a number of complex tasks associated with daily living.
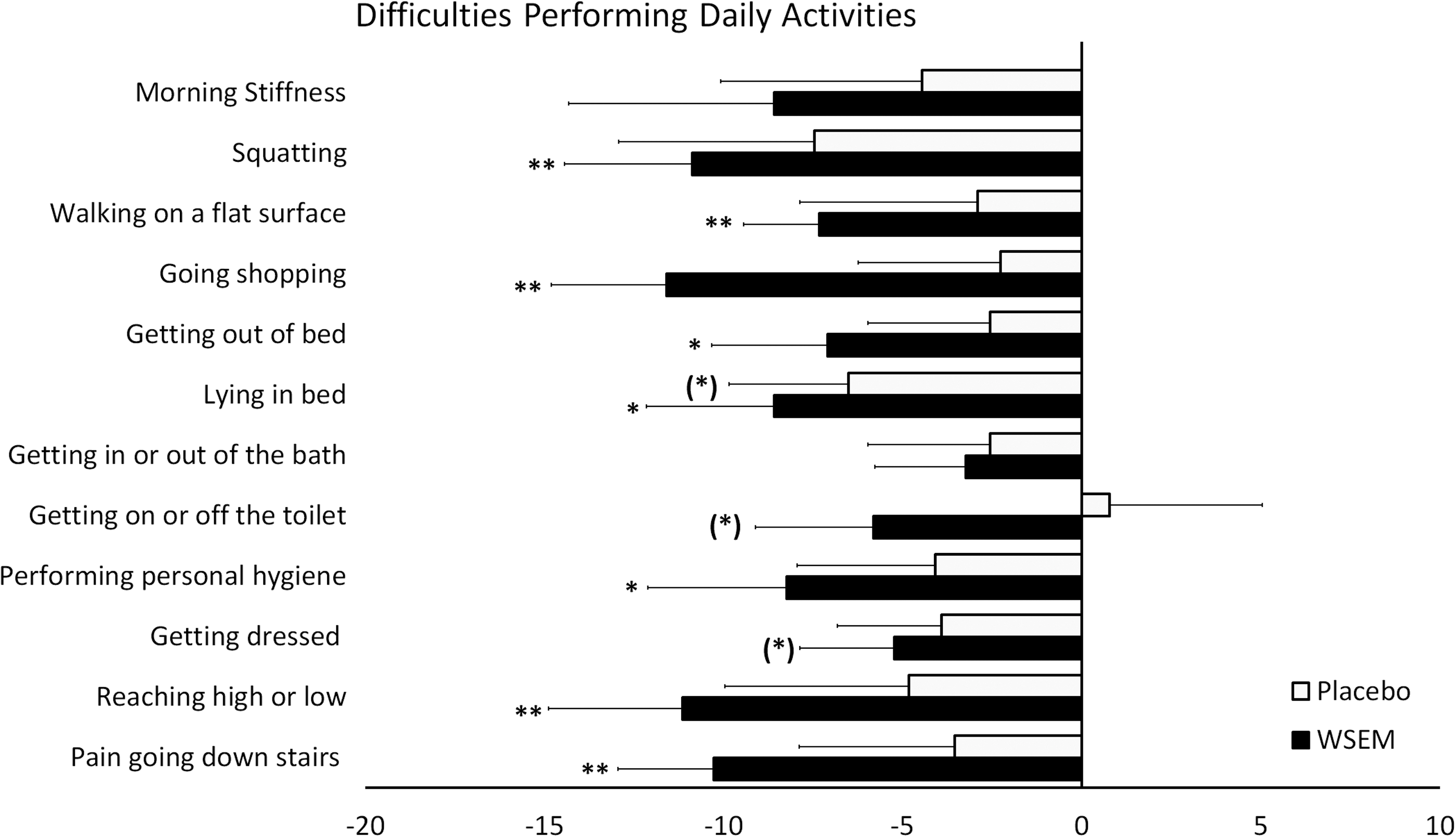
Difficulties performing 12 daily activities requiring complex joint motions are shown for changes in scores, occurring during consumption of WSEM (black bars) versus consumption of placebo (gray bars). The graph shows the group average change ± SEM. There was no statistical significance using between-treatment analysis. Statistical significance using within-subject analysis is shown by asterisks ((*) P < .1, *P < .05, **P < .01).
Increased level of physical activity
At each visit, study participants were asked to score their level of physical activity over the past 4 weeks. These self-reported physical activity levels were significantly higher during the 4 weeks where participants were consuming WSEM than when the same participants were consuming placebo (P < .05) (Fig. 3A). In parallel, an increase in physical energy levels was reported, but did not reach statistical significance (Fig. 3B).
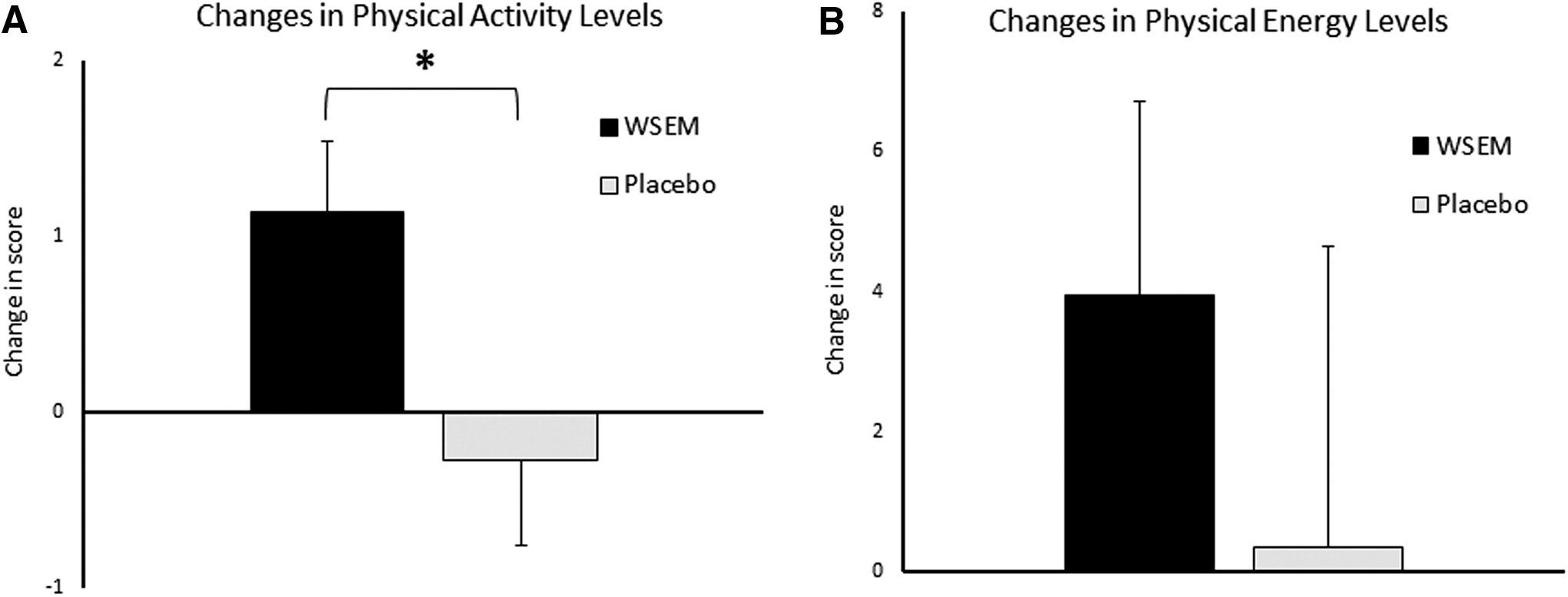
Change in levels of physical activity
Pain reduction
Study participants were required to score pain levels for various anatomical areas on a daily basis. The results showed no significant pain reduction across the whole study population (one subgroup studied during the winter and another during spring) nor did it reach significance for the subgroup (eight people) studied during the spring. However, the data from the subgroup that were enrolled in the colder winter months showed pain reduction in the upper and lower back during WSEM consumption, compared to the scores during placebo consumption (Fig. 4). There was no significant difference in pain scores for the upper or lower back at the beginning of each 4-week consumption period.
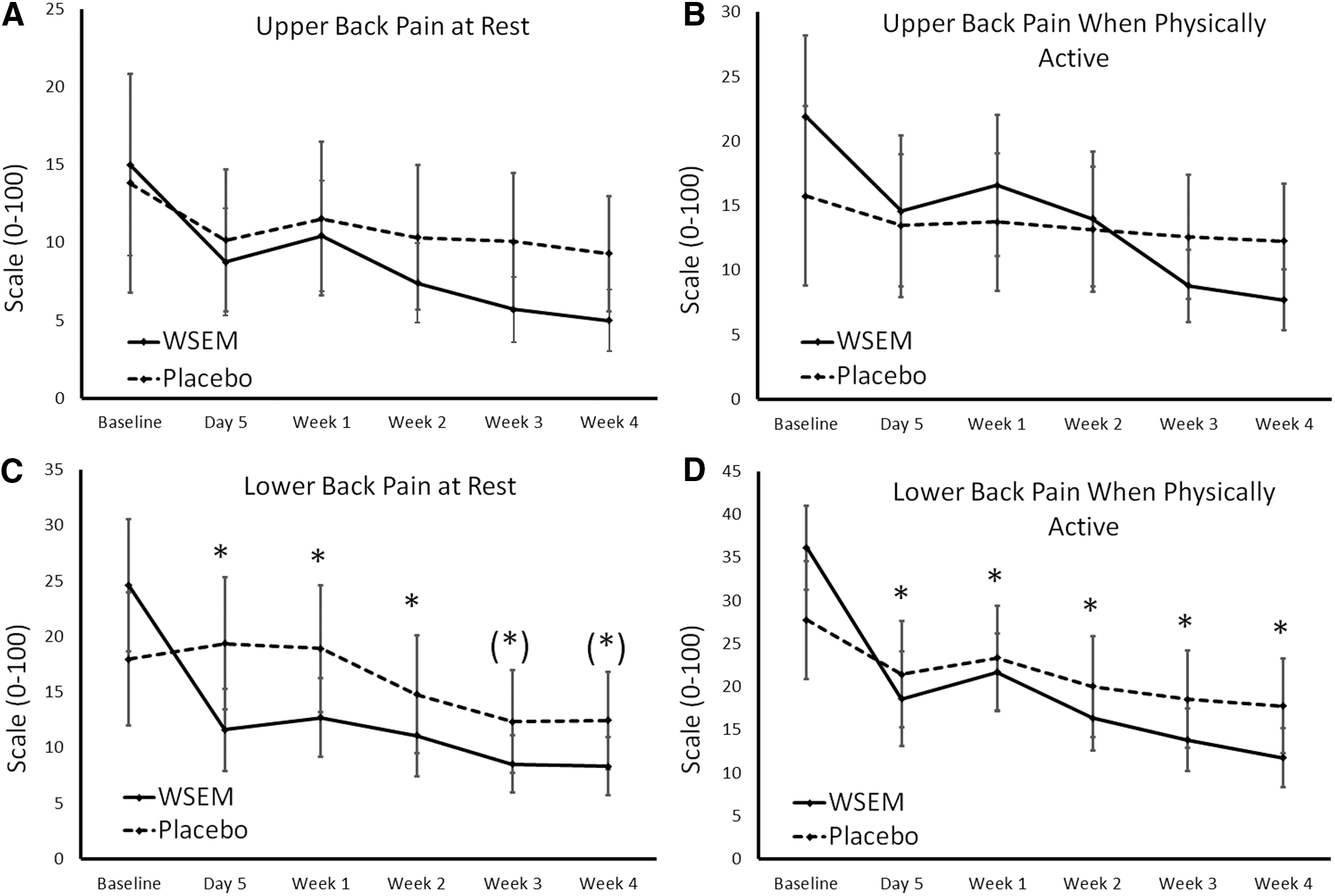
Upper and lower back pain scores at rest
Using between-treatment analysis of the changes in pain scores, a 43% reduction in upper back pain when at rest was seen after 5 days on WSEM, in contrast to 23% reduction for placebo. Upper back pain when physically active improved 33% on WSEM, in contrast to 15% for placebo. The 53% reduction in lower back pain when at rest after 5 days of WSEM consumption was significant when compared to placebo consumption (P < .05) and remained significantly lower than placebo scores for weeks 1 and 2 (P < .05) and remained lower than placebo throughout the 4-week phases (P < .071). The 49% reduction in lower back pain when physically active, compared to 23% reduction on placebo, after 5 days consumption was significant (P < .05), and the lower pain scores remained significant between the treatments throughout the remainder of the study.
Also on a daily basis, study participants were required to score pain levels for their identified area of primary pain at rest and when physically active. Reduced pain scores for primary pain when physically active were seen both when study participants consumed the active product and when consuming placebo. The pain reduction during WSEM consumption reached between-treatment statistical significance in the subgroup that consumed WSEM first, whereas it was not significant in the subgroup that consumed placebo first. This suggests that subjects who consumed the active product during the initial 4-week study phase recognized a lack of similar effect when subsequently consuming the inactive placebo. This was verified by feedback from study participants. Due to the crossover design, all study participants experienced both WSEM and placebo. Eight study participants volunteered information at study visits that they experienced a positive effect when consuming WSEM, not matched by the placebo, even though the study was conducted in a double-blind manner where study participants were never told when they were receiving WSEM or placebo.
Discussion
Joint mobility determines our ability to function, and maintaining good joint function and, thus, reducing sedentary behavior is a major factor in protecting our quality of life as we age. 16 In addition to age-related decline in joint function, many factors associated with diet and lifestyle contribute to reduction of joint mobility. 17 Physical activity in midlife is associated with mobility limitations in old age, where maintaining leisure activities has a protective effect by supporting joint mobility in old age. 18 Decreased joint ROM is associated with compensatory strategies. 19 In addition, obesity adds biomechanical stress on weight-bearing joints, contributing to postural dysfunction, abnormal gait, and increased stiffness along the upper and lower back, all contributing to chronic pain and further loss of physical functionality. 20 Nondisease-related factors contributing to a decline in joint function and mobility include occupational stress, 21 where additional factors affecting musculoskeletal mobility include mental stress-related muscular tension, 22 which over time can contribute to chronic reduction of mobility, typically of the neck and back.
Chronic pain associated with physical limitations prompts the use of over-the-counter pain medication. Consumable natural products for improving joint function include the structural support provided by consuming compounds such as glucosamine, collagen, hyaluronan, and similar natural compounds known to help improve joint function. 13 –15,23 –27 Additional consumables include polyphenol-rich natural products, known to provide both antioxidant protection and anti-inflammatory effects. 28,29
To study the impact of consumption of WSEM, this crossover study was designed to include people experiencing chronic pain in shoulders, hips, or knees, with associated reduced physical functioning for at least 6 months. The intent was not to study a diseased population such as subjects with osteoarthritis, but rather to evaluate improvements in a typical middle-aged population experiencing some joint discomfort. The study aimed at gathering data regarding improvements in joint function and mobility, as well as physical functioning associated with consumption of WSEM. It was important to use a crossover study design to evaluate any improvements during WSEM consumption in light of changes occurring in the same set of people when consuming placebo.
The consumption of WSEM was associated with generally improved ROM for spinal motion, including the neck, upper back, and lower back, as well as major joints such as the dominant shoulder and knee. The observation that improvements were of a general nature, and not limited to each person's primary pain area defined at the time of screening, suggests underlying support of joint and muscle functions. The significant improvement of neck motion was unexpected, since these areas were not defined as primary complaints at screening. The improved ROM for the dominant shoulder suggests improved muscular function and relief of tension, such as could be speculated to be associated with a mild chronic inflammatory condition. A previous placebo-controlled parallel-arm study on WSEM consumption in subjects with symptoms of osteoarthritis showed a significant reduction in CRP during WSEM consumption, in contrast to placebo (manuscript in preparation). Further studies on WSEM should include testing of free radical stress as well as cytokines involved in regulating inflammation and supporting regenerative functions.
In addition to collecting data on joint mobility and physical functioning, an important ancillary observation was a significant increase in self-reported physical activity levels. Physical activity is important in healthy aging, 27,28 and studies have shown that even moderate increases in physical activity levels can contribute significantly to prevention of age-related dementia through prevention of hippocampal atrophy. 29
The study also involved daily scoring of pain levels when at rest and when physically active. This data did not provide a significant pain reduction when analyzed across the two sets of subjects enrolled across different seasons, each having an associated weather profile. Subgroup analysis was performed on each set of study participants and showed that the subgroup enrolled in the study during the winter months, with a fairly stable weather pattern in the given geographical area, showed a rapid and sustained pain relief, which reached statistical significance for the lower back. Feedback from the study participants suggests that the pain relief happened as a result of WSEM consumption and subsequently facilitated an increase in physical activity. A future study should include systematic daily tracking of physical activity as well to help conclude the cause/effect relation and verify this correlation.
In conclusion, the data presented here showed improved mobility and ability to conduct daily activities when consuming WSEM. This study is important because the study population was not diagnosed with a joint disease, such as, for example, osteoarthritis, and the improvements were broad and independent of a person's identified major joint problem(s). Furthermore, the increase in physical energy and activity levels may potentially over time allow for reduction in body fat percentage and an increase in relative percentage of lean body mass. The parallel observations for increased physical energy levels suggest that consuming WSEM may hold promise as a natural support of maintaining quality of life in the aging human. Further studies are warranted in different study populations, such as geriatrics, athletes, and people recovering from trauma to joints and muscles.
Footnotes
Acknowledgments
The study was conducted at NIS Labs, an independent contract research laboratory specializing in natural products research. The study was sponsored by Biova LLC (Johnston, IA, USA), the manufacturer of hydrolyzed WSEM.
Author Disclosure Statement
All authors are associated with NIS Labs and have no competing financial interest in the subject matter.