
Abstract
Introduction:
The use of traditional, complementary, and integrative medicine (TCIM) has grown rapidly worldwide. The aim of this umbrella review is to provide a comprehensive synthesis of the available evidence on factors associated with TCIM use to identify the most influential factor driving the use of TCIM. This review was guided by the following research question: What is the most influential factor driving TCIM use?
Methods:
This review was conducted in accordance with PRISMA guidelines. International literature was systematically searched using PubMed, Embase, and manual searching of reference lists. The search was limited to peer-reviewed systematic literature reviews published between January 2005 to March 2024, in Arabic and English languages, and reported empirical research findings on factors associated with TCIM use.
Results:
A total of 62 review articles were included. The following five prominent factors were identified and critically analyzed: Socioeconomic status; dissatisfaction with conventional medicine; internal locus of control; being holistic, natural, and safe; and perceived usefulness. Of these, perceived usefulness, defined as the perceived benefits of a TCIM modality in meeting specific health needs or goals, was the most influential factor driving TCIM use.
Discussion:
The findings of this umbrella review revealed that individuals would not use a specific type of TCIM unless they perceived some benefit from its use, even if the benefit lacked supporting scientific evidence. This insight provides a foundation for researchers, health practitioners, and policymakers to advance TCIM research, clinical practice, and policy by targeting its perceived benefits. Focusing on perceived benefits can help researchers prioritize areas that are most valued by patients, leading to more impactful studies and evidence-based recommendations for practice. Understanding perceived benefits can also lead to more informed discussions between patients and health practitioners, creating a more collaborative and culturally sensitive health care environment. Furthermore, addressing perceived benefits can guide regulations to ensure the safe, effective, and ethical use of TCIM practices, leading to more effective integration of TCIM into conventional medicine as the evidence of its usefulness accumulates.
Introduction
The use of traditional, complementary, and integrative medicine (TCIM) has grown rapidly worldwide. 1 Approximately 80% of the global population utilizes TCIM 2 to address gaps in conventional medicine, cope with chronic illnesses, and meet their ongoing holistic health needs. 3 According to the World Health Organization (WHO), traditional medicine refers to health care practices and beliefs derived from an indigenous tradition, while complementary medicine refers to health care practices that are neither indigenous nor part of the conventional medicine of a nation. Integrative medicine is the integration of proven traditional and complementary medicine into conventional medicine. 3,4 Well-known TCIM modalities include acupuncture, herbal remedies, massage therapy, and spiritual practices.
While many literature reviews have explored factors influencing TCIM use, 5 –64 they vary in scope, and context, often examining specific populations, geographical location, or TCIM modalities. In addition, no study has systematically determined which factor is the most influential across different contexts. This gap underscores the need for a comprehensive synthesis that consolidates findings from existing reviews. To address this, the present umbrella review aims to identify the most influential factor driving TCIM use, providing a more integrated and generalizable perspective on TCIM use. This review is guided by the research question: What is the most influential factor driving TCIM use?
Methods
Study design
An umbrella review, also known as an overview of reviews, was conducted to summarize and synthesize findings from a diverse range of systematic reviews on factors associated with TCIM use. As the highest level of evidence synthesis, an umbrella review includes only high-quality systematic reviews, 65,66 providing a comprehensive and rigorous assessment of the available evidence. By integrating findings from multiple systematic reviews, this approach offers an overarching body of evidence, enabling clinicians and decision-makers to access the highest level of evidence in a shorter timeframe to support informed decision-making. 66
A key strength of an umbrella review is its ability to synthesize evidence from heterogeneous sources, capturing data from diverse populations and geographic locations. This heterogeneity enhances the generalizability and robustness of findings, making them more widely applicable. 65,66 The umbrella review design was particularly crucial for identifying the most influential factor driving TCIM use, as it allowed for the identification of the factor that remained consistently prominent across various contexts rather than those that were context-dependent. This study was conducted in accordance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 67
Search strategy
The search strategy was developed with the assistance of a health sciences librarian and included both subject headings and keywords related to three concepts: the field of interest (TCIM), phenomena of interest (factors associated with TCIM use), and publication type (review studies) (Table 1). Two electronic databases, Embase and PubMed, were systematically searched from January 2005 to March 2024. To ensure the search was comprehensive and all relevant literature was located, the authors also conducted hand searches of all referenced publications. Articles were eligible for inclusion if they were: (1) peer-reviewed systematic literature reviews of primary research studies, (2) published in Arabic and English languages, (3) and reported empirical research findings on factors associated with TCIM use. Review studies were excluded if they were of low quality. Articles that were not directly relevant to the specified inclusion criteria were also excluded (e.g., primary studies, book review articles, or reviews that did not adopt systematic search with explicit method/data-reporting procedures).
Databases and Search Strategy
Data screening
The study selection process was summarized using the PRISMA diagram (Fig. 1). The initial search yielded a total of 8,201 articles, which were exported to Covidence, an online software designed for systematic review management. Using Covidence, duplicate records were removed (729 publications). The title and the abstract of the remaining literature (7,472 publications) were screened to determine eligibility against the inclusion criteria. Potentially eligible articles were then screened in full text (144 publications). Finally, 62 systematic literature reviews were included. This process was performed by the first and the second authors independently. Disagreements on eligibility were resolved through discussions and consensus.
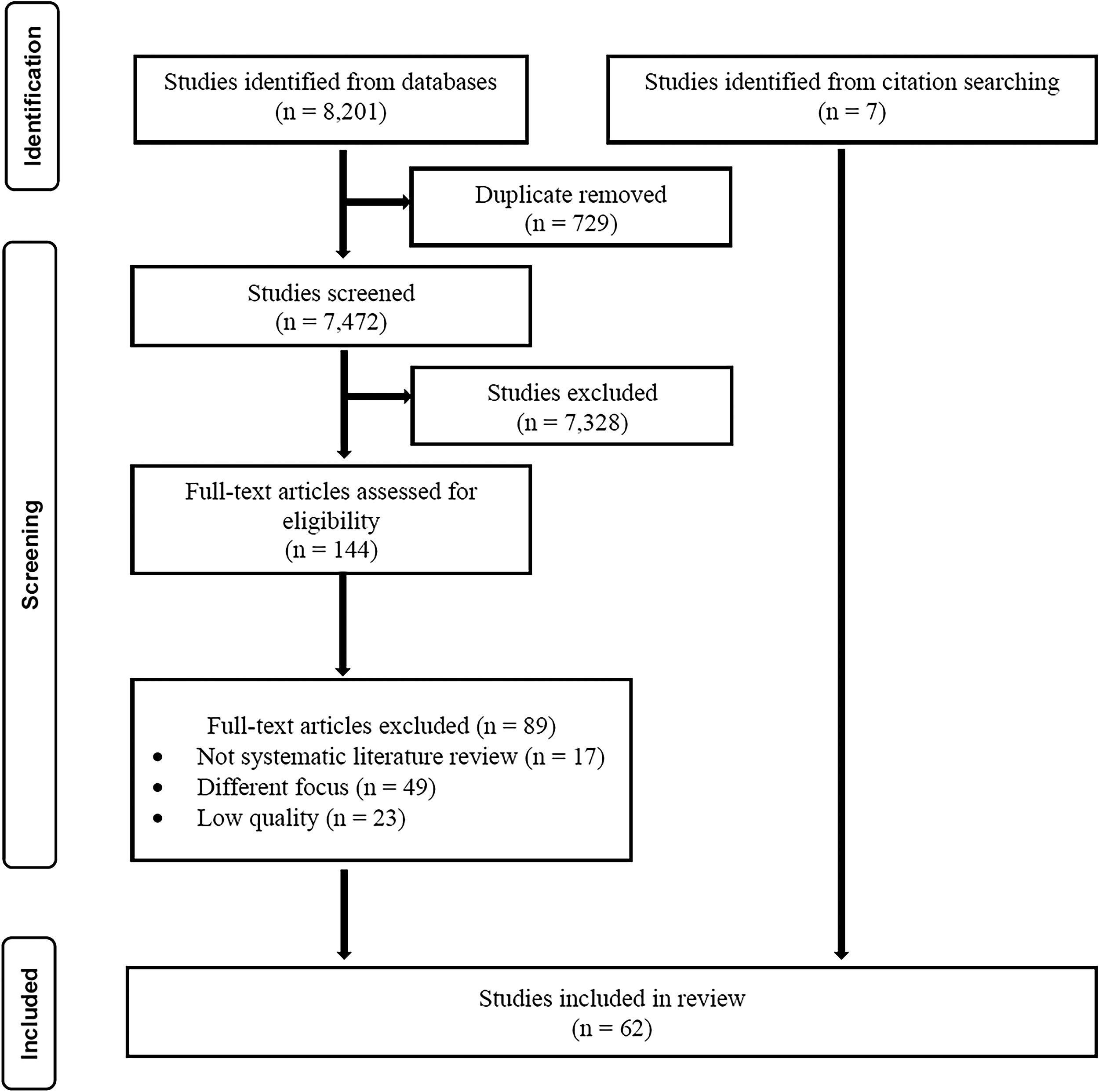
PRISMA flow diagram of the study selection process.
Quality assessment
The quality assessment of the retrieved reviews was conducted using the Joanna Briggs Institute (JBI) critical appraisal checklist for systematic reviews and research syntheses. 66,68 The JBI tool consists of 11 items assessing the following criteria for review papers: The statement of review question, inclusion criteria, search strategy, studies appraisal, data extraction, data synthesis, publication bias, and recommendations. The assessment criteria for each item are “yes,” “no,” “unclear,” or “not applicable”. If the specific criterion is met, one point is allocated. Thus, the overall quality score ranges from 0 to 11. A threshold of 10–11 for high quality and 7–9 for moderate quality was chosen to ensure rigor while maintaining comprehensiveness. Reviews scoring 6 or below were excluded due to significant methodological weaknesses. Two reviewers (W.H.M. and H.B.) independently assessed and scored each of the studies against the criteria on the JBI checklist to minimize bias. A third author (A.A.) was consulted if consensus could not be reached. Quality appraisal scores of all included reviews were presented in Table 2.
Data Extraction
TCIM, traditional, complimentary, and integrative medicine.
Data extraction and synthesis
To systematically extract data from the included articles, a data extraction form was developed (Table 2). The extraction form was piloted and amended by the first author to ensure that all the required information could be extracted. The form included prominent factors associated with TCIM use as well as items on general study characteristics: The author and publication year, quality appraisal score, number of studies included, years covered, and context (population, geographical location, and TCIM modality). All data were extracted by the first author and checked by the second author to minimize error.
Each review was carefully examined to identify and extract factors associated with TCIM use. A narrative synthesis approach was employed to systematically summarize and integrate findings, following an iterative process to categorize key factors across studies. Through this process, five prominent factors emerged, which were critically analyzed to assess their significance. To determine the most influential factor, each identified factor was evaluated based on its frequency and consistency across diverse populations and geographic regions. A factor was considered highly influential if it was consistently evident across various populations and geographic locations and demonstrated robustness beyond specific contextual settings. The results were structured according to the five key factors identified in the included reviews, providing insight into their relative influence and ultimately determining which factor played the most dominant role in driving TCIM use.
Results
Characteristics of included studies
This umbrella review synthesized the findings of 62 peer-reviewed systematic review articles published between 2005 and 2024. In total, this review incorporated data on 2,824 primary research studies collected from database inception to 2024. More than half of the included articles (60%) were published over the past 8 years, and this trend is in line with the growing interest in TCIM use as well as the global growing research attention in this field. The majority of the included reviews (64%) were of moderate quality, and the remaining 32% were of high quality. About 83% of reviews focused on TCIM in general, while the others focused on specific TCIM modalities, including herbal medicine, 26,34,44,49,56,62,69 acupuncture, 14 mistletoe therapy, 55 and chiropractic. 20
Studies were diverse and cross-cultural. Sixty-two percent of the included reviews included international studies with no geographical limits, while 38% were specifically conducted in the Middle East, 10,34,44 Saudi Arabia, 27 Morocco, 62 African countries, 26,39,41,52 Sub-Saharan Africa, 43,46 –48 European countries, 7,40,51,55 United Kingdom, 50 Canada, 25,51 Asia-Pacific countries, 57 Australia, 9,18,25 the United States, 15,25,51 New Zealand, 25 and Republic of Korea. 8 The included reviews were also diverse in terms of populations. While 21% of the reviews were conducted among the general population, 79% were conducted among condition-specific populations including cancer, 15,25,33,38,45,48,49,51,55,59,62 maternal and reproductive health, 26,31,32,34,39,44,47,52,56,70 gastrointestinal disorders, 9 cardiovascular disease, 42 malaria, 57 diabetes, 10,29,41 hypertension, 46 attention deficit hyperactivity disorder, 61 autism, 17 sickle cell anemia, 28 arthritis, 24 amyotrophic lateral sclerosis, 63 headache and migraine, 5,64 constipation, 23 back pain, 16 depression, 53 neurological disorders, 54 and menopause. 22 Twenty-one percent of the included reviews focused on uniquely important subgroups such as children and adolescents, 11,17,28,33,38 elderly, 69 rural communities, 60 nurses, 30 community pharmacists, 58 and indigenous and ethnic minority populations. 15,21,25 Detailed characteristics of the included studies are presented in Table 2.
Factors associated with TCIM use
This umbrella review identified five key factors driving TCIM use: socioeconomic status (SES), dissatisfaction with conventional medicine, internal locus of control, being holistic, natural, and safe, and perceived usefulness. While all five factors were prominent across the included reviews, perceived usefulness emerged as the most influential due to its consistent presence across diverse populations and geographical regions, indicating its widespread relevance beyond specific contexts (Table 2).
Factor 1: SES
SES has been associated with TCIM use, though findings remain inconsistent across studies. The majority of reviews reported a positive association between TCIM use and higher income and education, 5,7 –12,15 –18,20,22,24,26,33,34,38,41,43,45,48 –50,52 –62,69 indicating that individuals with higher SES are more likely to use TCIM. However, other reviews found the opposite trend, with low SES being linked to TCIM use in certain contexts. 26,34,43,52,57,62,69 Notably, several reviews documenting the TCIM–SES relationship reported contradictory findings or no clear association across the studies they analyzed. 6,9 –11,14,18,21 –23,26,28,32,35 –38,40,47,49,52,57,58 This inconsistency suggests that SES is not a universally influential factor driving TCIM use, as its impact is highly context-dependent.
Factor 2: Dissatisfaction with conventional medicine
Dissatisfaction with conventional medicine (e.g., being ineffective, causing side effects, unsatisfying doctor-patient interactions) was reported as a factor influencing TCIM use. 16,18,19,21,23,29,35,36,38 –40,43,45 –47,49,50,53,54,57,59,60,64,70 However, findings from several systematic reviews across multiple contexts reveal that patients generally do not abandon conventional medicine in favor of TCIM. Rather, the concurrent use of both approaches is widely documented as the global norm. 5,12,16,18,19,21 –25,35,36,41,43,46,48,49,53,57,59 –61,63,64 In addition, TCIM is not solely sought for managing illness but is widely used by healthy individuals for wellness and prevention benefits, 5,50,53 independent of any dissatisfaction with conventional health care. While dissatisfaction with conventional medicine is a prominent factor, it does not meet the criteria for being the most influential factor, as its influence remains context-dependent and does not consistently drive TCIM use beyond specific health care settings.
Factor 3: Internal locus of control
Internal locus of control, described as “actively participating in treatment,” “autonomy,” “self-determination,” or “taking control of one’s own health and body” was reported as a potential driver of TCIM use. 6,13,14,18,19,24,31,36,43,53,55,70 However, two systematic reviews examined the link between internal locus of control and TCIM use reported mostly negative results. No relationship was found by Galbraith et al.’s review, 6 while Bishop et al. 13 reported contradictory findings, with the majority of studies (10 of 13) reporting no association. These findings indicate that internal locus of control is not consistently linked to TCIM use and does not meet the criteria for being the most influential factor.
Factor 4: Being holistic, natural, and safe
The perception of TCIM as holistic, natural, and safe was cited as a factor driving its use. 5,10,13,14,18,19,21,22,24,27,29,31,36,37,40,42,43,51,53,58,61,70 However, literature indicates that individuals do not choose treatments arbitrarily, even when they value these attributes; rather, they select a specific treatment modality based on its perceived benefits in meeting their health needs. 19,31,36,37 Systematic reviews indicate that TCIM users are critical consumers who discontinue treatments if dissatisfied, 36 do not automatically assume TCIM’s safety and quality, 27,32,35,36 and advocate for clear regulatory and educational frameworks to guide its provision. 6,19,27,35,36 Consequently, TCIM use is more prevalent among well-educated individuals. 16,18,19,21,23,29,35,36,38 –40,43,45 –47,49,50,53,54,57,59,60,64,70 These findings suggesting that TCIM use is a deliberate and informed choice driven by its perceived benefits in meeting specific health needs rather than solely a preference for natural or holistic treatments. While these attributes may contribute to TCIM’s appeal, they do not consistently drive its use across diverse contexts. Therefore, this factor does not meet the criteria for being the most influential driver of TCIM use.
Factor 5: Perceived usefulness
Perceived usefulness, defined as the perceived benefits of a TCIM modality in meeting specific health needs or goals, emerged as the most influential factor driving TCIM use. Unlike other factors, perceived usefulness was consistently linked to TCIM use across diverse populations and geographic contexts. 5,10,18 –64 Findings from this umbrella review indicate that, regardless of contextual differences, individuals are unlikely to use a specific TCIM modality unless they perceive some benefit from it, even in the absence of scientific evidence. The reproducibility of perceived usefulness across various contexts reinforces its central role in TCIM use, suggesting that it is a universal determinant rather than a region-specific or population-dependent influence. The most reported benefits of TCIM were curing illnesses, 19,24,29,32,35,36,38,40,45,48,52,56,59,61 alleviating symptoms, 10,19,21,22,26,29,31,34,36,38,45,48,53,54,61,63,64,71 reducing side effects of conventional medicine, 18,19,25,29,38,48,49,55,59,61 addressing unmet psychological or spiritual needs, 19,29,31,45,49,52,54,59 improving quality of life, 19,22,23,40,49,53,59 maintaining well-being, 19,21,22,25,28 –32,34 –36,38,40,45,48,49,54,56,59,60 and preventing disease. 10,18,19,22,29,31,32,34,36,39,40,45,47,52
Discussion
This systematic umbrella review synthesized the available evidence and identified perceived usefulness as the most influential factor driving TCIM use. Four other factors, including SES, dissatisfaction with conventional medicine, internal locus of control, and being holistic, natural, and safe, were also prominent. However, by integrating findings across diverse populations and geographical locations, this review demonstrates that perceived usefulness is not merely a frequent finding but a consistently dominant factor shaping TCIM use globally.
SES was related to TCIM use in 58% of the reviewed literature, but inconsistent results were noted and there appeared to be geographical differences. TCIM is easily accessed in regions where TCIM is grounded in the local history and culture. TCIM is readily available to the population regardless of an individual’s SES, even in high-income countries where conventional systems are well established. For instance, In Saudi Arabia, where the conventional health care system is well developed, individuals use TCIM because it is deeply embedded in their native cultural traditions. 72 In some instances, the traditional medicine may even be considered an integral part of the conventional medicine and is thus covered by the national insurance (e.g., China). 35
A similar pattern of TCIM use is seen in low-resource areas where TCIM is an entrenched part of the culture and access to conventional care is limited due to its cost and distance. In this context, owing to the limited availability and soaring cost of conventional medicine, TCIM use might be expected to be disproportionately more common among people with low SES. However, it is still well documented that TCIM is a culturally respected and valued health care resource and is thus accessed by both the poor and elite; the only difference is that affluent individuals have greater access to more resources, including conventional medicine. 73,74 In fact, recent literature reviews of low-resourced areas in Africa, including sub-Saharan Africa, suggest that as access to conventional medicine increases, TCIM is also increasingly sought. 43,73
In regions where TCIM is not grounded in the history and tradition of the local population, TCIM may not be easily accessible, as seen in the examples discussed above. In such contexts, TCIM might be disproportionately accessible by individuals with high SES. For instance, studies based on national survey data collected in the United States at multiple points in time (1998, 75 2008, 76 2014 77 ) have consistently reported that TCIM users are better educated and wealthier than TCIM nonusers. These findings are to be expected, as TCIM use in such contexts can be expensive and is seldom covered by health care insurance. The popularity of TCIM among highly educated, affluent individuals suggests that they have greater access to health information and resources and have disposable income to spend on an array of treatment options, including both conventional and TCIM.
Nevertheless, the two extreme situations observed in some African regions (low-resource areas) and the United States (high-resource areas) do not reflect a profile of TCIM users but rather illustrate structural obstacles (cost and access) that are beyond the control of individuals of low SES. In fact, a population’s access to treatments of proven efficacy, including conventional medicine and TCIM, should not be limited to individuals with high SES. This is a principle that is firmly rooted in the 1948 WHO constitution, which declares that health and health care are fundamental human rights, not privileges for those who can afford them. 78
Dissatisfaction with conventional medicine was reported by 39% of the studies. However, results of multiple literature reviews suggested that it is relatively rare for patients to reject conventional medicine and rely solely on TCIM. The populations in countries ranging from low to high income view conventional medicine as their default option and tend to use TCIM concurrently to complement rather than replace conventional medicine. 5,12,16,18,19,21 –25,35,36,41,43,46,48,49,53,57,59 –61,63,64 In addition, the value of TCIM as an adjunctive therapy to conventional medicine has been documented in several systematic reviews. 18,19,21,29,33,35,45,53 –55,59,61 Specifically, those reviews found that TCIM use reduced side effects from conventional therapies (e.g., chemotherapy); assisted in disease management; addressed unmet emotional, psychological, or spiritual needs; and improved general well-being and quality of life. These results suggest that while individuals may retain a belief in the importance and effectiveness of conventional medicine, they also feel that TCIM is a valuable health care resource, even if it is only to provide hope when conventional care fails. 18,19,24,28,36,38,40,45,55,56,59
In 19% of the studies, internal locus of control was reported as a factor influencing TCIM use. This factor suggests that patients gravitate toward TCIM because they value having an active or collaborative role in treatment decisions, a role they may find restricted by conventional medicine. However, the most prominent characterization of TCIM users is that they are relatively affluent and highly educated individuals with greater access to resources and higher levels of health literacy. 5,8 –12,15,16,18,20,22,24,33,34,38,41,45,48 –50,53 –55,58 –62,64 This typical TCIM user profile is not compatible with the notion of individuals who are prevented from having an active role in treatment decisions within the conventional health care system. In addition, the internal locus of control factor suggests that users of TCIM are more likely to value active participation in and personal control of their treatment process than nonusers. Nonetheless, with respect to the potential association between internal locus of control and TCIM use, no significant associations were found in most of the studies included in two systematic reviews. 6,13 That is, those using TCIM did not show a significantly different locus of control (or desire for control and active participation in treatment) than TCIM nonusers. This finding was not surprising, as the tendency to use TCIM is not a stable or unique trait of some individuals by which they can be differentiated from TCIM nonusers. In fact, an individual may even use TCIM in one context but not in others as needed.
The perception of TCIM as holistic, natural, and safe was cited as a factor driving TCIM use in 35% of the studies. However, prior research suggests that individuals do not choose treatments solely based on these attributes but rather gravitate toward what they believe is useful in addressing their specific health needs and goals. 19,31,36,37 Literature on this factor further hypothesize that TCIM is generally utilized because it enables self-care due to its holistic and natural characteristics. 3 However, this assumption does not fully account for practitioner-led TCIM modalities such as acupuncture, which do not inherently promote self-care and can pose risks if unsafely practiced. 79 Yet, acupuncture remains one of the most commonly used TCIM modalities worldwide. Moreover, self-care is not exclusive to TCIM; it is also an integral aspect of conventional medicine, 50,80 including practices such as adherence to medication regimens, which are not necessarily natural, holistic, or free from side effects. Despite this, patients do not abandon conventional medicine or its self-care components.
Finally, this review revealed consistent evidence that perceived usefulness, reported by 79% of the studies, is the most influential factor driving the use of TCIM. Findings revealed that individuals would not use a specific type of TCIM unless they perceived some benefits from its use, even if the benefit lacked supporting scientific evidence. In other words, individuals’ primary motive for using TCIM is a perception that a particular TCIM modality is useful in addressing their specific needs or goals. 19,31,36,37,81 –83 This perception may be based on scientific information or myths, personal experience or recommendation of others, religious or cultural traditions and values, or massive media via advertisements or internet search. 21,22,30 –32,34,63
Perceived usefulness was generally reported in two ways across the included studies: (1) as the degree of confidence in the usefulness of a TCIM in meeting a specific health goal or need (e.g., faith in the usefulness of a TCIM modality and gaining hope when other options fail), (2) or in terms of perceived beneficial outcomes (e.g., curing illness and preventing disease). Hence, key terms representing this factor across the reviewed literature were faith or confidence in TCIM, 25,36,37,45,56,58 cultural beliefs in its usefulness, 19,21,25,29,31,35,40,46,57 being effective, 10,21 –24,27,29,32,35 –39,44,45,47,50,52,53,55,56 gaining hope for treatment, 18,19,24,28,36,38,40,45,55,56,59 curing illnesses, 19,24,29,32,35,36,38,40,45,48,52,56,59,61 managing health conditions, 10,18 –20,24,26 –29,32,34,36,39,41,44,45,47,52,56,59 –61,63 alleviating symptoms, 10,19,21,22,26,29,31,34,36,38,45,48,53,54,61,63,64,71 reducing stress, 25,30,32,40,45,59 boosting immunity, 38,40,45,48,49,55,59 managing side effects of conventional medicine, 18,19,25,29,38,48,49,55,59,61 supplementing or synergizing conventional treatment, 18,19,21,29,35,38,45,53 –55,59,61 improving quality of life, 19,22,23,40,49,53,59 spiritual and psychological healing, 19,29,31,45,49,52,54,59 preventing disease or complications, 10,18,19,22,29,31,32,34,36,39,40,45,47,52 and promoting overall well-being and health. 19,21,22,25,28 –32,34 –36,38,40,45,48,49,54,56,59,60
Not only was perceived usefulness the most consistent factor across various contexts, but it was also the most robust, aligning with individuals’ broader motivation for seeking health care, including conventional medicine. A literature review on treatment selection concluded that in both TCIM and conventional medicine, individuals are primarily influenced by their perceptions of how useful a particular treatment will be in addressing their specific health needs or goals. 83 Furthermore, empirical evidence supports the notion that perceived usefulness is a key factor in long-term commitment to health care use, influencing both adherence and ongoing utilization. 36,37,81 Specifically, a recent systematic review investigating adherence patterns found that an individual’s degree of confidence in TCIM usefulness (e.g., having a positive attitude toward its usefulness) was a major factor in determining whether they continued or discontinued a particular TCIM modality. 37 This suggests that perceived usefulness extends beyond initial TCIM use, playing a critical role in sustained engagement with these treatments. Given its strong influence on TCIM use, it is expected that TCIM adoption will continue to expand as scientific evidence supporting its benefits grows.
Limitations and strengths
This review was restricted to peer-reviewed articles, excluding gray literature such as government reports, policy papers, and conference proceedings. While this exclusion may have introduced publication bias, peer-reviewed literature was prioritized to ensure methodological rigor and the inclusion of systematically analyzed evidence. Given that the focus of this review was to identify the most influential factor driving TCIM use, peer-reviewed articles provide the most reliable and validated findings for this purpose. Therefore, while the omission of gray literature limits the breadth of sources, it is unlikely to have altered the conclusions of this review.
A key strength of this umbrella review is the heterogeneity of the included studies, which examined factors driving TCIM use across various populations and geographical locations. By synthesizing evidence from heterogeneous studies, this review distinguishes between universal driver of TCIM use and context-specific influences, providing a more nuanced and globally relevant understanding of what shapes TCIM use.
Conclusion
This systematic umbrella review provides comprehensive international examination of evidence-based factors associated with TCIM use. The findings indicate that perceived usefulness, defined as the perceived benefits of a TCIM modality in meeting specific health needs or goals, is the most influential factor driving TCIM use. Given that perceived usefulness is influential in driving TCIM use, TCIM use is expected to expand as evidence of TCIM’s usefulness increases.
Implications
Understanding TCIM within national contexts
National health authorities can use perceived usefulness as an indicator of how TCIM is valued and utilized within their populations. Beyond simply identifying which TCIM modalities are widely used, it is essential to assess what specific health benefits individuals believe they are receiving from these practices. By developing a national profile of TCIM use based on these perceived benefits, authorities can gain valuable insights into public health care preferences. This approach ensures that policies are better aligned with actual demand.
Prioritizing research and resource allocation
Future research should validate the most sought-after benefits of commonly used TCIM modalities. It is essential for TCIM studies to align with the priorities of the users, bridging the gap between scientific evidence and the public’s perception of the benefits of TCIM. This alignment can ensure that limited research funding and health care resources are directed toward the TCIM practices that offer the greatest potential public health impact. Moreover, studies should focus on whether perceived benefits align with measurable clinical outcomes, providing evidence that can help health care professionals and policymakers integrate TCIM modalities into conventional health care settings in an evidence-based manner.
Optimizing TCIM integration within national health care systems
TCIM modalities that citizens are most confident in their usefulness are more likely to positively impact public health when integrated into conventional health care systems under appropriate regulations. By integrating widely accepted TCIM practices, health authorities can ensure evidence-based, standardized, and safe TCIM use within medical settings. This integration can maximize patient engagement and satisfaction, leading to improved health outcomes. As well as it can strengthen health care system responsiveness to culturally embedded health care practices.
For example, if traditional massage therapy is widely used for injury rehabilitation, health care facilities can partner with licensed TCIM practitioners, ensuring that only certified professionals with standardized training provide these services within regulated medical settings.
Footnotes
Acknowledgment
The authors would like to acknowledge Amelia Brunskill, Health Sciences Librarian at the University of Illinois Chicago, for her valuable assistance in developing the search strategy for this study.
Authors’ Contributions
W.H.M.: Conceptualization, methodology, validation, formal analysis, investigation, writing—original draft, writing—review and editing, funding acquisition, and project administration. H.B.: Conceptualization, validation, formal analysis, and writing—review and editing. A.A.: Conceptualization, validation, and writing—review and editing. J.M.S.: Conceptualization, validation, writing—review and editing, and supervision. C.F.: Conceptualization, validation, writing—review and editing, and supervision.
Availability of Data and Materials
All data generated or analyzed during this study are included in this published article.
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
This study is part of the first author W.H.M.’s PhD research, which was supported by a scholarship from King Abdulaziz University.