
Abstract
Background:
Biofield Therapies, with a historical lineage spanning millennia and continuing relevance in contemporary practices, have been used to address various health conditions and promote wellbeing. The scientific study and adoption of these therapies have been hindered by cultural challenges and institutional barriers. In addition, the current research landscape for Biofield Therapies is insufficiently documented.
Objectives:
This scoping review aims to comprehensively document the peer-reviewed research landscape of Biofield Therapies. Furthermore, an online searchable and dynamic Evidence Map was created to serve as a publicly accessible tool for querying the evidence base, pinpointing research gaps, and identifying areas requiring further exploration.
Methods:
A systematic search of PubMed, Embase, CINAHL, and PsycInfo databases was conducted from inception through January 2024. Peer-reviewed interventional studies in English involving human participants receiving Biofield Therapy were included. Data on study design, population, intervention, comparator, outcomes, citation details, and direction of results reported were extracted and synthesized into two summary tables and three data tables.
Results:
In total, 353 studies in 352 published reports were included: 255 randomized controlled trials, 36 controlled clinical trials, and 62 pre-post study designs. Named biofield interventions included Reiki (n = 88), Therapeutic Touch (n = 71), Healing Touch (n = 31), intercessory prayer (n = 21), External Qigong (n = 16), Spiritual Healing/Spiritual Passé/Laying-on-of-hands (n = 14), “distant or remote healing” (n = 10), and Gentle Human Touch/Yakson Therapeutic Touch (n = 9). Also included were 56 studies in 55 reports involving bespoke, unknown, or other interventions, 20 studies involving multimodal interventions, and 17 studies involving multiple biofield interventions. Studies encompassed a wide variety of populations, most commonly healthy volunteers (n = 67), pain (n = 55), and cancer (n = 46). As reported in the Abstracts, nearly half of the studies (n = 172) reported positive results in favor of the Biofield Therapy for all outcomes being investigated, 95 reported mixed results, 71 reported nonsignificant results, 3 reported negative results, and 12 studies did not report the direction of results.
Conclusions:
Despite rising interest in Biofield Therapies among researchers, practitioners, and patients, the integration of these interventions into allopathic medical systems is hindered by challenges in researching these therapies and inconsistent reporting. These issues contribute to inconclusive findings, which limit our understanding of the efficacy of Biofield Therapies for specific conditions. The resulting scoping review and interactive Evidence Map aim to empower stakeholders to overcome these obstacles, thereby strengthening the evidence for the potential adoption of Biofield Therapies as future integrative care options in allopathic medicine.
Introduction
Biofield Therapies (BTs), sometimes referred to as energy/subtle energy or spiritual healing modalities, have been utilized for millennia to address various health conditions and enhance human wellbeing. Practitioners of BTs, often known as healers, report facilitating healing processes within recipients (sometimes referred to as healees) by interacting with their biofields. 1,2 This interaction involves mobilizing or channeling what is sometimes termed energy, consciousness, or spirit in modern conceptualizations and concepts such as Qi, Prana, mana, or Ki in religious and ancient traditions. Some of these practices have distinct lineages dating back to recorded history, while others have been codified within the last century using similar principles but divorced from religious or spiritual beliefs. 1,2
Modalities commonly recognized as BTs include Reiki, Healing Touch, Therapeutic Touch, Spiritual/Faith Healing, and External Qigong, among others. The utilization of these practices to address a diverse range of physical and mental health conditions is increasing. 3,4 This trend is apparent not only among individuals seeking therapies outside the conventional medical system for both chronic and acute conditions but also within the expanding availability of BTs in hospital systems and medical clinics. In 2012, the International Association of Reiki Professionals reported that 60% of the 25 best hospitals (as ranked by U.S. News and World Report) had formal or informal Reiki programs available to their patients and/or staff. 5
With the increased use and availability of all integrative medicine modalities, BTs are also available for patients within the U.S. Veteran Administration (VA) medical facilities and clinics. 6,7 Notably, BTs are not required to be offered at VA facilities but are considered optional approaches deemed safe that VA clinics are allowed to offer to patients. 8 In fact, a 2015 report found that 30% of VA clinics included BTs (referred to as energy medicine in their report), marking a doubling (20–40 clinics) since 2011. The primary reasons reported for seeking the use of BTs were anxiety (68%), enhancement of well-being (62%), alleviation of back pain (60%), and to address depression symptoms (60%). 9 These findings were echoed in a 2021 publication reporting on 196 Department of Veterans Affairs Medical Centers (DVMC), where the authors noted that many VA clinics throughout the United States had officially incorporated BTs. Among the BTs reported in this survey, Therapeutic and Healing Touch (34 programs), Reiki (18 programs), and Native American Healing (9 programs) were all incorporated into DVMCs. 10
Despite their increasing use and purported benefits, the scientific study and adoption of BTs in Western culture have been hindered by cultural challenges and institutional barriers, and the research landscape is poorly understood in terms of mechanisms and efficacy for specific therapies, conditions, and outcomes. Previous systematic reviews that synthesize and pool the literature on various BTs such as Healing Touch, Therapeutic Touch, and Reiki have generally suggested potential benefits for outcomes such as pain and anxiety. 11,12 However, these reviews also frequently highlight methodological limitations, a scarcity of high-quality randomized controlled trials (RCTs) with robust sample sizes, and inconsistent reporting practices. Consequently, findings have been inconclusive, occasionally resulting in unwarranted recommendations or assertions regarding the efficacy of these therapies. Notably, Cochrane reviews have underscored that aggregating results across studies often fails to demonstrate significant effects for specific BTs due to the inconsistent state of the evidence. 13,14 The difficulties facing the study and integration of BTs are also exemplified by the National Center for Complementary and Integrative Health’s (NCCIH) statement on Reiki, which asserts: “Reiki hasn’t been clearly shown to be effective for any health-related purpose. It has been studied for a variety of conditions, including pain, anxiety, and depression, but most of the research has not been of high quality, and the results have been inconsistent.” 15
To advance the understanding of and transparently showcase the current research landscape on BTs, we performed a scoping review (ScR) with results accompanied by a searchable interactive dynamic Evidence Map (EM) tool. The aim is to provide stakeholders with a reliable foundation of existing knowledge, enabling informed decisions on the next steps for advancing BT research and determining the appropriateness of care.
ScR objectives
The specific objectives of this ScR were to capture the breadth and depth of existing literature on BTs, identify the diverse populations and medical conditions studied, and describe the variety of BT practices presented in research. Additionally, the ScR aimed to assess the outcomes and measures used to evaluate the effectiveness and impact of BT interventions, as well as describe the controls, comparators, and study designs employed.
EM objectives
From the ScR findings, the authors created a publicly available, interactive, and dynamic EM to be used as a tool to learn about the current research landscape and facilitate a deeper understanding of the breadth of research to date. This EM will help researchers identify gaps and promising areas, develop focused hypotheses, and explore the effectiveness and mechanisms of BTs for specific conditions, populations, and outcomes.
Methods
Defining BTs and biofield interventions
The term “biofield” was originally proposed during an ad hoc meeting of researchers and integrative medicine practitioners convened by the U.S. National Institutes of Health’s Office of Alternative Medicine (now the NCCIH since 2014). The biofield concept emerged in an effort to bridge a diverse set of practices whose underlying mechanism of action was culturally conceptualized as practice-specific forms of an undefined form of energy. From these discussions, the biofield was defined as “a massless field, not necessarily electromagnetic, that surrounds and permeates living bodies and affects the body.” 16,17 Over time, the term has evolved as researchers and practitioners have modified the definition to align with their specific research and practice. At present, there remains no consensus on the definition of “Biofield Therapy,” with different perspectives shaping its conceptualization and application. Furthermore, “biofield” is not available as a Medical Subject Heading term according to the National Library of Medicine.
To define BTs for this ScR, the research team engaged in a formalized process to solicit feedback from stakeholders and subject matter experts (SMEs). First, the team compiled existing definitions of Tracking the evolution of the term “biofield” (since its newly proposed usage in 1992). Extracting definitions and modalities from previous systematic reviews. Reviewing definitions and modalities discussed in the 2015 special issue of Global Advances in Health and Medicine, titled “Biofield Science and Healing: Toward a Transdisciplinary Approach.”
18
The collated definitions and interventions, along with a series of questions, were sent to 10 SMEs for feedback (see Supplementary Data). Responses received from six SMEs were collated and integrated into a proposed definition and list of modalities and then shared with additional four stakeholders including researchers and community leaders. Iteratively, this exercise yielded a working definition of BTs, a compilation of umbrella terms associated with BTs, as well as a list of specific BTs considered for this ScR.
Our definition of BTs, adapted from Jain et al., 2 was used to inform the development of the search strategy as well as the inclusion and exclusion criteria for this ScR:
BTs are nonphysically invasive and noninstrumental therapies in which a practitioner explicitly works locally or remotely with another living system’s (e.g., person, plant, animal, cell) biofield (interacting fields of energy, consciousness, and/or information that surrounds living systems) to facilitate a healing response.
Informed by the definition and feedback from SMEs and stakeholders, this ScR included for consideration a preidentified list of biofield modalities (see Supplementary Data). Additionally, acknowledging that there might be therapies meeting the BTs definition, which were either unnamed or unfamiliar to the study team, we also employed umbrella terms to identify and include additional therapies not initially listed (see Supplementary Data).
Protocol and registration
Our protocol was devised using the Preferred Reporting Items for Systematic Reviews and Meta-analysis extension for ScRs (PRISMA-ScR) and was registered with the Open Science Framework 3 (https://osf.io/2hmxz). The PRISMA-ScR reporting checklist is available in Supplementary Table S1.
Information sources and search strategy
From the BTs definition and list of modalities, we devised a search strategy for the ScR. PubMed, Embase, CINAHL, and PsycInfo were searched from their database inception through December 2022 and updated through January 2024. Complete search strategies can be found in Supplementary Data.
Study selection
Eligibility criteria
Studies were eligible if they (1) were peer-reviewed interventional studies presented in the English language, including clinical trials (e.g., RCTs, nonrandomized controlled clinical trials [CCTs], pre-post interventional trials); observational studies (e.g., prospective or retrospective longitudinal cohort studies, case–control studies, cross-sectional studies, and case studies and case series); as well as ScRs, systematic reviews, and meta-analyses and (2) involved humans, animals, or cell models as the study participants (i.e., receivers of the intervention) in which (3) a BT was delivered between a practitioner(s) (i.e., healer[s]) and client(s)/patient(s)/receiver(s) (i.e., healee[s]). All clinical outcomes and types of control/comparators were considered for inclusion. Observational studies that involved surveys reporting the prevalence of BT usage within a population and studies involving multimodal interventions, where subjects were exposed to various modalities including BTs, were also initially included.
Editorials, commentaries, book chapters, conference proceedings/abstracts, narrative reviews, and practice guidelines were excluded. Studies involving plants or inanimate objects as recipients, or where the practitioner served as the recipient (working on their own system), were excluded. Additionally, interventions where the BT involved the use of a tool or instrument, such as tuning forks and magnets, or directly incorporated other modalities into their practice, such as massage or aromatherapy, were excluded.
Article selection
The initial screening phase involved 10 screeners (B.S., C.D., H.B., L.B., N.L.D., N.I., N.P., P.M., R.S., and S.A.). Each title and Abstract citation yielded from the literature search was screened in tandem using the predefined study eligibility criteria within the online systematic review platform Covidence.org. Conflicts were resolved by consensus between screeners with the guidance of the review manager (L.T.) and SME (M.L.S.).
Studies that passed the initial screening phase were tagged according to study design type, population type, and BT intervention type. The results were sorted according to these tags. Given the number of studies that met the eligibility criteria, data extraction was limited to clinical trials involving humans. All other studies were reserved for future ScRs and updates to the online EM.
Charting the data
A data extraction protocol was developed, pilot tested, and implemented for identifying and describing study characteristics including population details, intervention and comparator specifics, outcome measures, as well as the results and conclusions of the studies (see Supplementary Data for the full list). Following the pilot testing and training period, six reviewers (S.A., C.D., N.I., R.M., A.S., and N.L.D.) independently extracted relevant data items from studies that met the eligibility criteria during the full text review using a companion Excel spreadsheet (Microsoft Corporation). The review manager (L.T.) verified each extraction and provided guidance to the reviewers. A risk-of-bias assessment was not conducted.
Synthesis of results
Data were synthesized into two summary tables (Tables 1 and 2) and three data tables describing each study according to its study design: RCTs (Supplementary Table S2), CCTs (Supplementary Table S3), and pre-post study designs, which compare outcome measurements before and after subjects are exposed to the biofield intervention (Supplementary Table S4). Each table is organized by the type of BT. The authors collaborated with Alma Economics to devise an online interactive and dynamic EM, which will be updated yearly. Category buckets were created according to study design, condition of population, intervention, comparator, and outcome.
Summary Table 1
Studies in which the authors named the biofield intervention “Distant Healing” or “Remote Healing”.
Neonatal (<4 weeks); infants (4 weeks-1 year); children (2–12 years); adolescents (13–18 years); adults (19–64 years); seniors (65+ years).
Does not include pre-post study designs. Each study may have more than one comparator arm.
Based on results reported in the abstract on the effectiveness of the BT on outcomes reported as compared with the comparator arm(s) for RCT and CCT study designs or baseline for pre-post study designs.
BT, Biofield Therapies; CCT, controlled clinical trial; NA, not applicable; NR, not reported; NS, not statistically significant; PP, pre-post study design; PTSD, post-traumatic stress disorder; RCT, randomized controlled trial.
Summary Table 2
Bespoke, unknown, or other interventions outside of the categories already listed in Table 1: biofield awareness, n = 1; bioenergy healing (The Mackay Method), n = 1; “biofield therapy,” n = 1; Brennan Healing Science, n = 2; Catalonia Technique, n = 1; Compassionate Intention Distance healing, n = 1; direct mental interactions with living systems, n = 2; Distant Intentionality, n = 1; Energy Chelation, n = 1; “energy healing,” n = 2; “energy medicine,” n = 2; Expressive Touch, n = 1; Gentle Touch Therapy, n = 3; Healer’s electromagnetic heart field, n = 1; “healing therapy,” n = 1; “healing therapy/healing ceremony,” n = 1; Informational Manual Therapy/Poyet–Pialoux Method, n = 1; Instituto di Ricerca sull’Energia Cosmica Applicata, n = 1; Johrei, n = 5; Magdalena Energy Healing, n = 1; mindfulness-based touch therapy, n = 1; Native American method, n = 1; Okada Purifying Therapy, n = 4; Oscillatory Biofield Therapy, n = 1; Pagan Spell-Casting, n = 1; Polarity Therapy, n = 2; Pranic Healing, n = 3; “psychic healing,” n = 1; Psychokinetic Healing, n = 1; Quantum BioEnergetics, n = 1; Raimondi Technique, n = 1; Remote Mental Healing, n = 1; The Secret prayer, n = 1; Tellington Touch, n = 1; Theta Healing, n = 1; Trivedi Effect® attunement method, n = 1; tawba and istighfar Spiritual Therapy, n = 1; virtual energy healing, n = 1.
In which subjects within an intervention arm were exposed to more than one modality including BT.
Studies with multiple biofield intervention arms comparing biofield interventions of different category types.
Neonatal (<4 weeks); infants (4 weeks-1 year); children (2–12 years); adolescents (13–18 years); adults (19–64 years); seniors (65+ years).
Does not include pre-post study designs. Each study may have more than one comparator arm.
Based on results reported in the abstract on the effectiveness of the BT on outcomes reported as compared with the comparator arm(s) for RCT and CCT study designs or baseline for pre-post study designs.
BT, Biofield Therapies; CCT, controlled clinical trial; NA, not applicable; NR, not reported; NS, not statistically significant; PP, pre-post study design; PTSD, post-traumatic stress disorder; RCT, randomized controlled trial.
Results
Selection of sources of evidence
The initial comprehensive database search yielded 26,070 citations. After removal of duplicates as well as records that clearly did not fit study design criteria, 13,406 titles and Abstracts were screened according to the predetermined eligibility criteria, and 12,071 citations were excluded.
Of the 1335 citations that passed the initial screening, 802 citations were identified as noninterventional study designs and/or nonhuman populations and were reserved for a future ScR. The remaining 533 interventional trials involving humans were sought for PDF retrieval, of which 30 PDFs were unavailable. After full-text screening, additional 152 citations were excluded largely due to wrong study design (n = 70) or wrong intervention (n = 74), resulting in 351 reports. One further study was found via reference list review, resulting in a total of 353 studies within 352 reports included in this ScR (see Fig. 1 for further details). 19 –370 All studies and their characteristics were included in the online EM (www.biofieldsciencemap.org). 19 –370
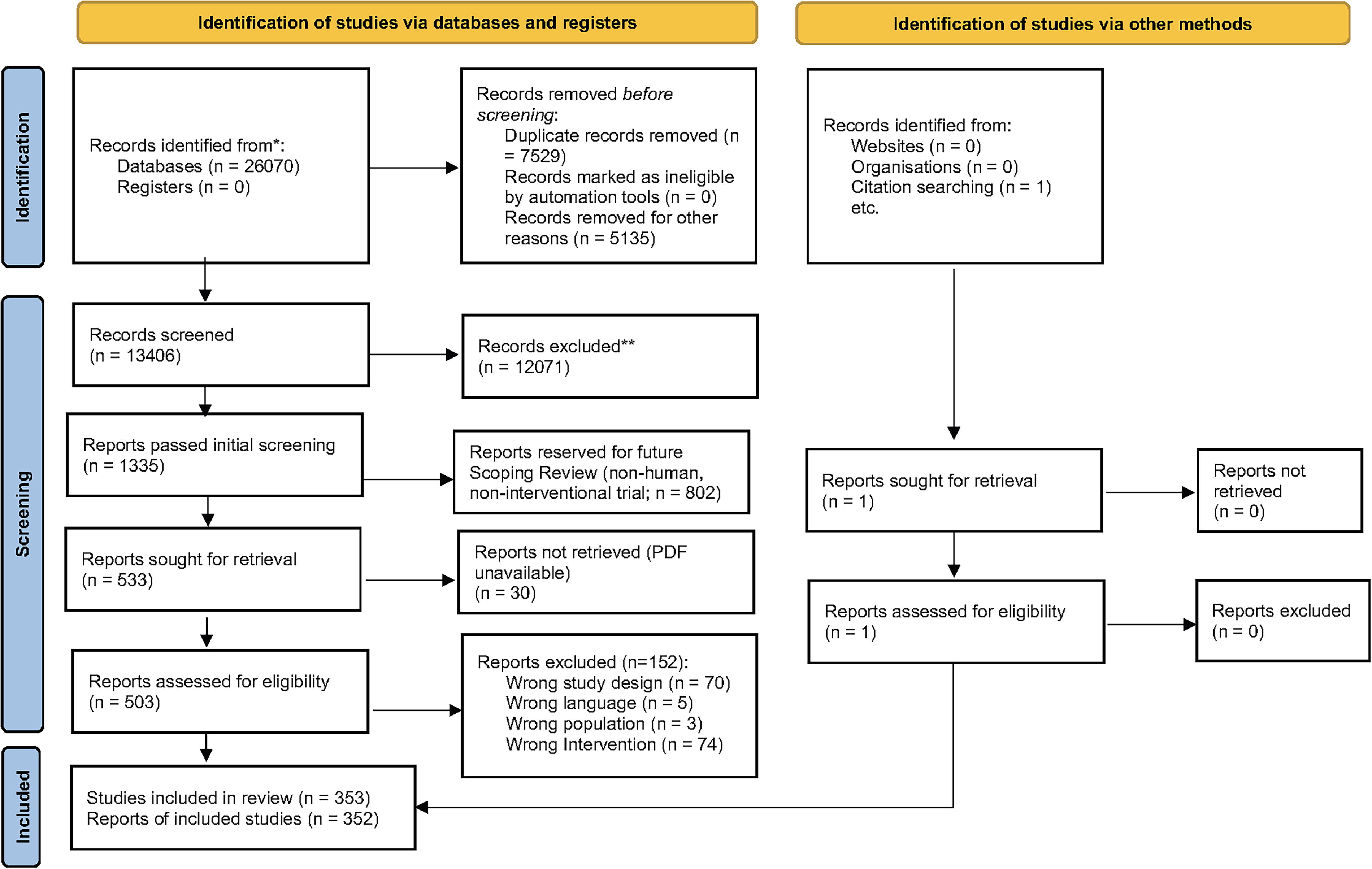
The flow diagram.
BTs research landscape
Study designs
Of the 353 studies that met the inclusion criteria, 254 (72.0%) were RCTs, 35 (9.9%) were CCTs, 62 (17.6%) used a pre-post study design, and 1 report included 2 studies, an RCT and a CCT.
Publication characteristics
Studies were published from 1965 to 2024 (Fig. 2). Among the 353 studies within 352 published papers identified, articles were published in nursing journals (n = 105; 29.8%), integrative medicine journals (n = 104; 29.5%), and medical/health care journals (n = 90; 25.6%). The remainder were distributed across frontier journals (n = 25; 7.1%), psychology journals (n = 15; 4.3%), religion journals (n = 7; 2.0%), and public health journals (n = 6; 1.7%) (see Figs. 2 and 3).
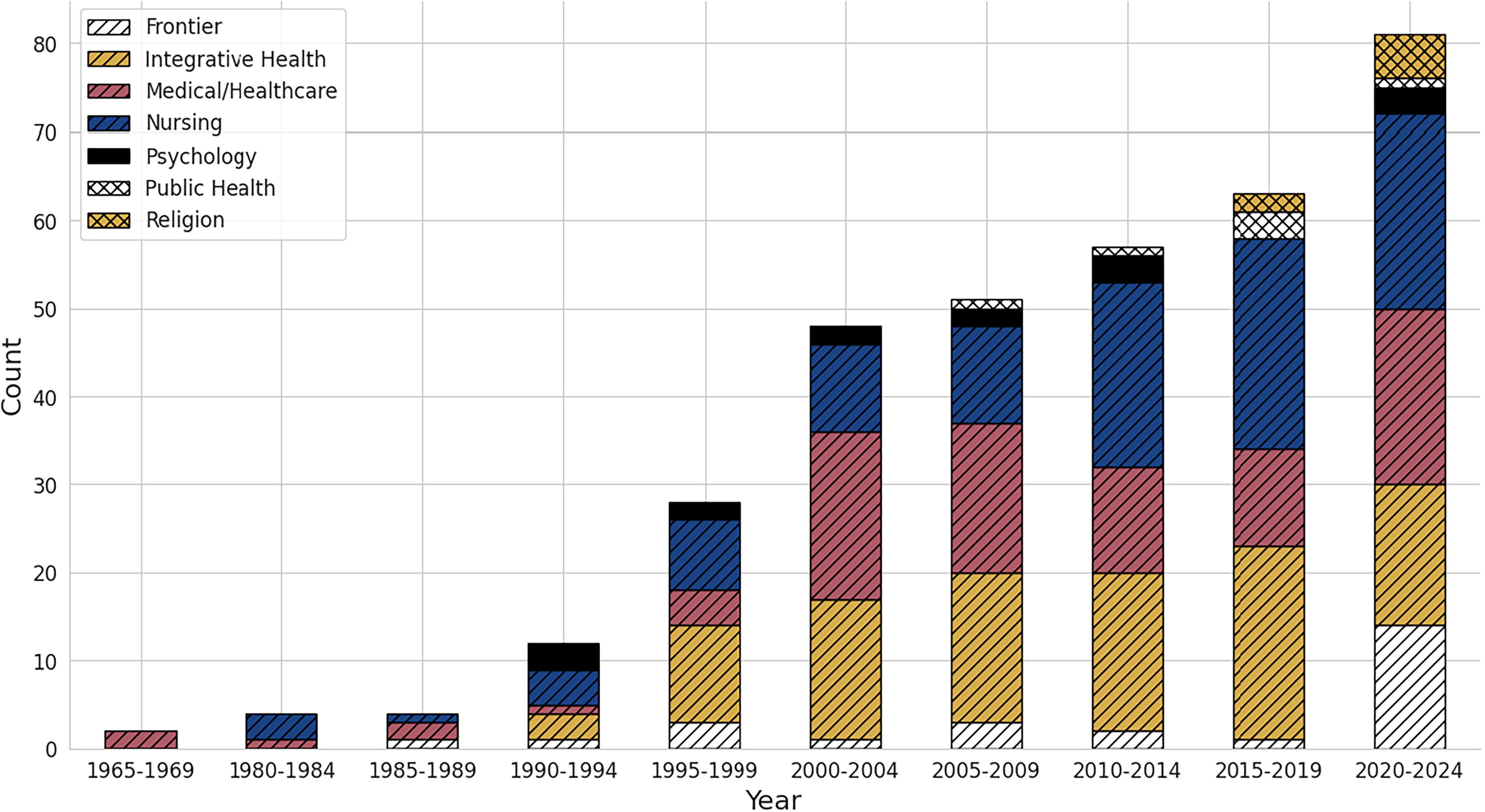
Records by year by journal category.
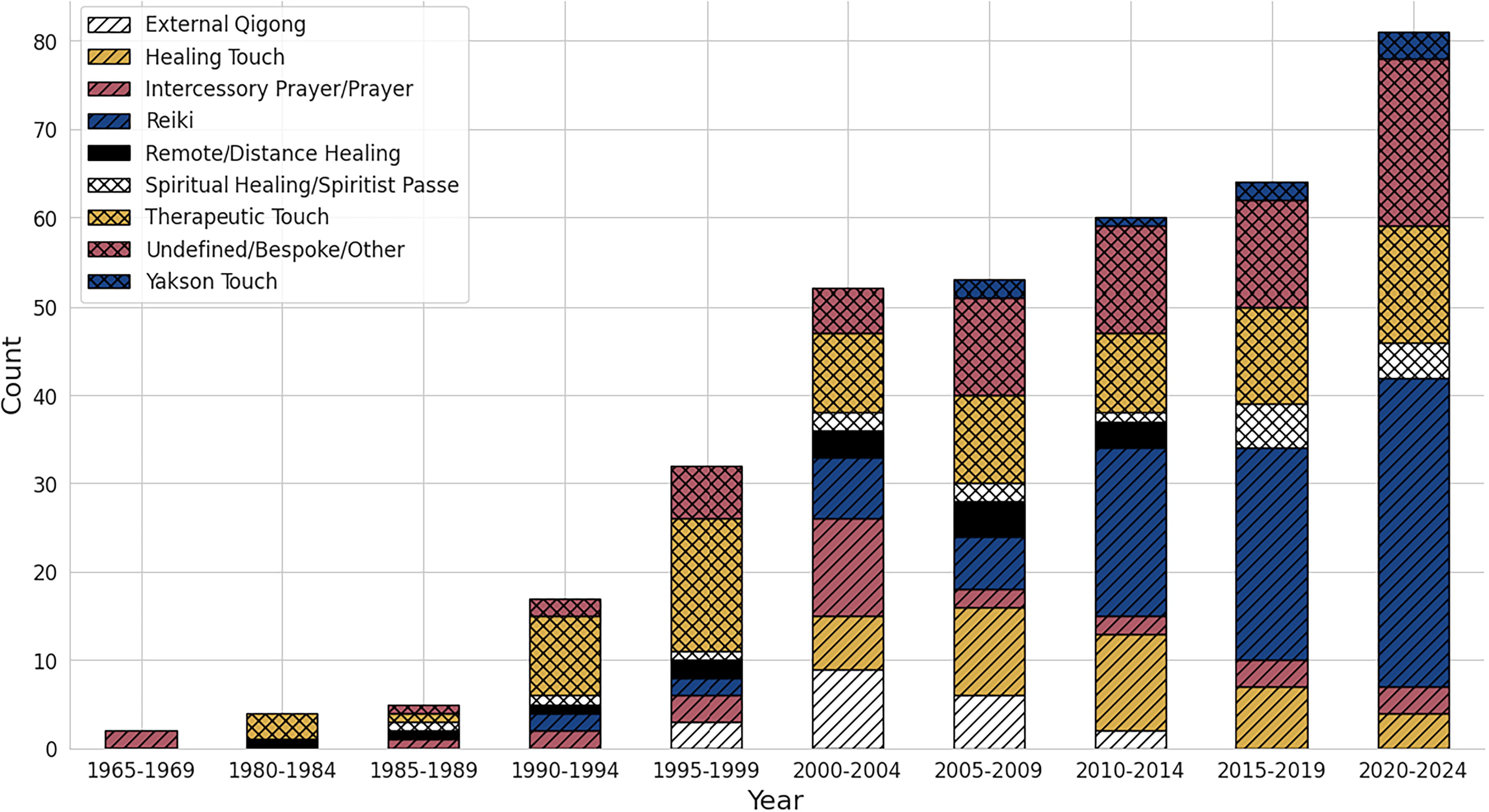
Records per year by Biofield Therapy.
Population types
The most common conditions or populations across studies were healthy volunteers (n = 67; 19.0%), patients with pain (n = 55; 15.6%), patients with cancer (n = 46; 13.0%), and surgical patients (n = 40; 11.3%). Several studies included populations with musculoskeletal conditions (n = 29; 8.2%), pediatric populations (n = 27; 7.6%), and those with cardiovascular or circulatory conditions (n = 27; 7.6%). Additionally, 30 studies (8.5%) investigated populations with psychological conditions, including anxiety, depression, post-traumatic stress disorder, and stress. For information on other populations studied, see Tables 1 and 2.
Intervention types
Reiki (n = 88; 24.9%) and Therapeutic Touch (n = 71; 20.1%) were the most common interventions evaluated among the studies. Other inventions included Healing Touch (n = 31; 8.8%), intercessory prayer (n = 21; 5.9%), External Qigong (n = 16; 4.5%), Spiritual Healing/Spiritual Passé/Laying-on-of-hands (n = 14; 4.0%), Distant or Remote Healing (n = 10; 2.8%), and Gentle Human Touch/Yakson Therapeutic Touch (n = 9; 2.5%) (see Table 1). Fifty-six studies (15.9%) in 55 reports involved bespoke, unknown, or other interventions outside of the categories already listed (see Table 2). Twenty studies (5.7%) involved multimodal interventions (see Table 2). Seventeen studies (4.8%) involved multiple biofield intervention arms (see Table 2).
Outcome categories
Study outcomes were sorted into six categories, with many studies assessing outcomes in multiple categories: psychological and behavioral (n = 273; 77.3%), biological and physical (n = 231; 65.4%), pain (n = 123; 34.8%), cognitive (n = 13; 3.7%), outcomes involving study execution (e.g., study feasibility and retention of participants) (n = 8; 2.3%), and other outcomes (e.g., number of hospital days, medication usage, etc.; n = 25; 7.1%).
Direction of results
Since this is a ScR and not intended to determine efficacy or effectiveness, the authors did not perform statistical calculations or pool effect sizes. However, a basic scan of reported results at an Abstract level was conducted. Based on primary authors’ conclusions, nearly half of the studies (48.7 %, n = 172) reported all positive results in favor of BTs. Nonsignificant results were reported in 20.1% of studies (n = 71), negative results in 0.9% (n = 3), mixed results in 26.9% (n = 95), and 3.4% (n = 12) did not report the direction of results. For more details, refer to Tables 1 and 2, as well as Supplementary Tables S3, and S4.
Interactive Evidence Map—Synthesis of results
The Biofield Science Evidence Map (https://www.biofieldsciencemap.org/) offers a comprehensive visual representation of the results from the ScR, encompassing all 353 unique reports. a This dynamic online tool allows users to search and tailor the displayed evidence according to their specific inquiries.
Customizing the EM
Table views
Users can adjust the orientation of the X and Y axes within the map to organize and view results using different study characteristics. These include: Intervention (X-axis) by Health Condition (Y-axis) (default view) (Fig. 4) Health Condition (X-axis) by Intervention (Y-axis) Intervention (X-axis) by Outcome Category (Y-axis) Direction of Study Results (X-axis) by Intervention (Y-axis) (Fig. 5) Direction of Study Results (X-axis) by Intervention (Y-axis)
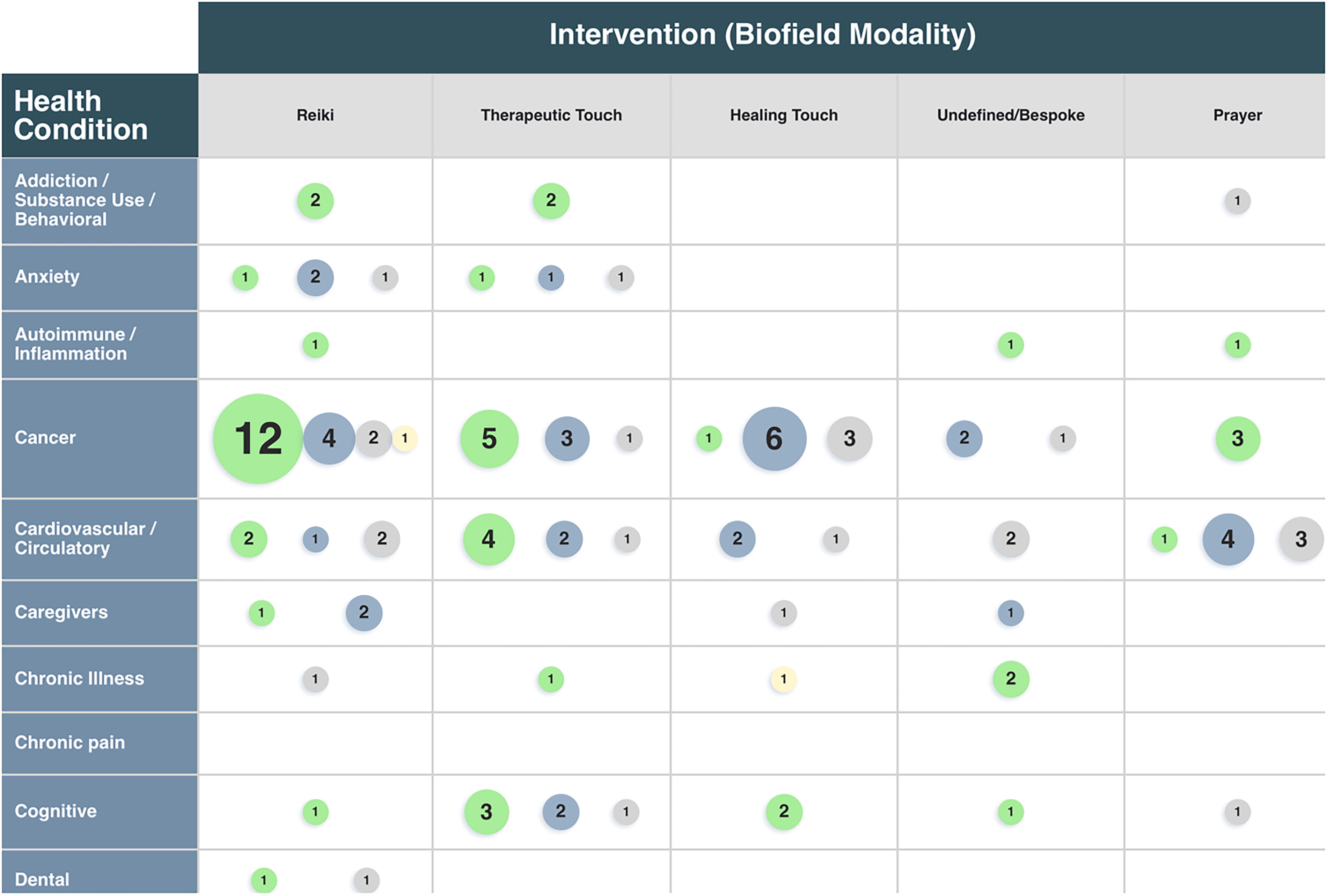
Evidence Map: Intervention (X-axis) by Health Condition (Y-axis). This snapshot offers a glimpse of the Evidence Map; for a comprehensive view, please refer to the online version (https://www.biofieldsciencemap.org), which allows both vertical and horizontal scrolling to view the full list of interventions (biofield modalities) and health conditions. Information about bubble size, color, and inserted numerical value of each circle are explained in the EM study display section. Further user options are described in EM table views, EM filters, and EM search function.
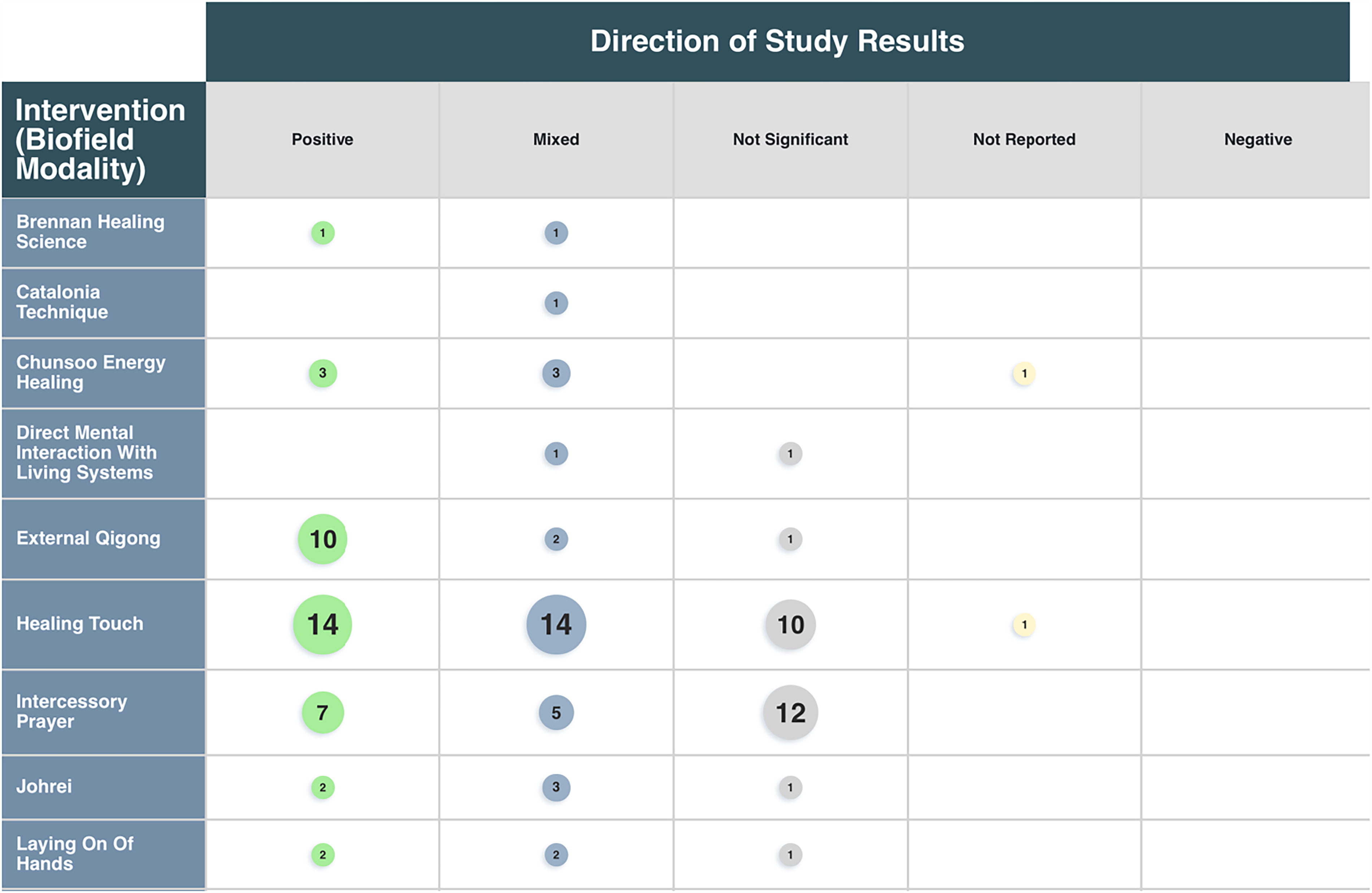
Evidence Map: Direction of Study Results (X-axis) by Intervention (Y-axis). This snapshot offers a glimpse of the Evidence Map; for a comprehensive view, please refer to the online version (https://www.biofieldsciencemap.org/), which allows for vertical scrolling to view the full list of interventions (biofield modalities). Information about bubble size, color, and inserted numerical value of each circle are explained in the EM study display section. Further user options are described in EM table views, EM filters, and EM search function.
EM study display
The diameters of the bubbles adjust based on the selected view, conforming to the dimensions set by the X and Y axes. Each bubble represents the number of studies meeting specific criteria, with the size of the bubble corresponding to the quantity of studies (larger bubbles indicating a greater number of studies) and color indicating the direction of results: Green: Positive results Blue: Mixed results Gray: Nonsignificant results Red: Negative results Yellow: Results not reported
Selecting (clicking on) a bubble displays a list of the studies, including details such as title, authors, year, and journal. Selecting a specific study reveals a page featuring information about the article extracted by the review team, complete with a hyperlink to access the full publication if openly available, or to the publisher’s page if not.
EM filters
Users can sort by various criteria, including intervention, health condition, study design subtype, direction of study results, published year, species, outcome category, sample size, local or distance forms of BT delivery, comparator category, single or multiple sessions, age category, and gender. Additionally, they can filter studies based on whether the study tested potential mechanisms.
EM search function
For inquiries not covered by basic and advanced filters, the search box allows users to find specific information within the map and individual article pages.
Discussion
This work represents the first comprehensive ScR of all peer-reviewed clinical studies on BTs conducted up to January 2024. It can be used to explore potential research directions based on gaps and promising areas for exploration. Unlike a systematic review, this ScR was not designed to assess the effectiveness, efficacy, or safety of interventions but to understand the overall research landscape. Our review identified 1,335 publications during the initial screening, of which 352 publications (353 studies) met our eligibility criteria. Based on previous reviews 11,12 and expert consultation, we defined inclusion/exclusion criteria centered on the reported mechanisms of BTs (e.g., channeling energy to facilitate healing), due to the limited scientific understanding of these practices, similarities in reported healing methods, and commonalities in their approach and delivery.
Widening the scope of the present review beyond individual BT modalities to include the umbrella of BTs was designed to elucidate the different characteristics of the research performed to date and to identify any notable clusters of evidence as well as gaps in the research landscape. This is particularly crucial given the limited advancements in scientific understanding of efficacy and mechanisms, which hinder the ability to assess whether adoption of BTs as an integrative modality within allopathic medicine is warranted. Additionally, by defining and categorizing the landscape of BTs in this review, our aspiration is that the definitions and terminology pertaining to BTs may be used and adopted as a valuable resource.
Research challenges
Challenges for clinical research
Researching BTs presents unique challenges, as evidenced by several inconsistent reporting practices observed in the studies. First, while the authors provided details about patient populations and their inclusion/exclusion criteria, there was a frequent absence of information regarding the specific inclusion/exclusion criteria applied to the BT practitioners (“healers”) described in the methods (see Supplementary Tables S2, S3 and S4). The criteria applied to identify BT practitioners, particularly concerning their training and years of practice, are crucial as they may impact the intervention’s efficacy. Additionally, detailed information about the “dosage” of BTs was sometimes lacking: 29 (8.2%) studies did not report the duration of the healing intervention, nor did they specify the number of BT sessions. 25,26,44,55 –57,59,65,69,73,74,78,82,87,88,92,94,136,178,182,194 ,196,198,220,227,271,278,286,345
The lack of uniformity and consistency in reporting on the identification of BT practitioners (or “healers”) and the “dosage” of therapies makes it difficult to assess the efficacy of the BT, further complicating the study of these treatments. BT practitioners report that BTs can operate through a variety of delivery methods, including hands on, hands above, or near the patient, and even at a remote distance. Practitioners often combine these methods, tailoring their approach to each patient’s unique needs, thereby challenging research designs to mirror real-world practice. Among the 286 studies in which the BT was delivered locally, 56 studies (19.6%) did not report whether the BT was delivered hands-on, hands-off, or a combination of both. 22,31,40,45,49,51,57,64,68,74,75,102 –106,115,116,149,159,160,174,176 –178,199,202,203,212,218,219,229,236,237,241,247,253,255,256,263,268,273,275,283,286,307,309,310,312,314,325,327,345,349,351,358 Furthermore, 38 studies (13.3%) reported mixed delivery without precise detailed information on when and why there was variation in the delivery of the BT modality. 26,32,47,48,55,59,67,78,86,87,93,95 –97,99,120,123,127,136,147,151 –154,156,157,163,166,168 –171,175,205,254,287,298,299 Additionally, BT practitioners frequently integrate various additional modalities and tools, such as aromatherapy, massage, tuning forks, and relaxing/soothing music, all of which have been demonstrated to have positive effects on patient-reported outcomes. This multifaceted approach in terms of delivery and integration of additional modalities not only impedes standardization of study protocols but also complicates the isolation of specific variables for investigation. The studies included in this review often did not provide clear intervention protocols, which hindered the ability to assess the precise methodology employed and its impact on outcomes, as well as hampering attempts to reproduce the research findings.
The challenge of disentangling and isolating elements of real-world practice within the research landscape has resulted in a lack of clarity regarding how to assess the effectiveness of a specific BT intervention, given the variability in therapy delivery, regardless of the presence of additional modalities. Understanding the key elements that render a BT effective is crucial for advancing both our comprehension of their mechanisms and the potential integration of these therapies into allopathic medicine. A further challenge to BT clinical research is to establish rigorous control conditions. While various controls were been employed, including the use of “sham” (or “mock”) in 104 (29.5%) of the studies identified by this review, 22,28,30,36 –38,47,50,52,53,117,120 –122,125,128,130,131,134,137,147,148,151 –155,157,159,162,167,187,213,215 –219,221,233,235,236,238,240 –244,247 –249,251,258 –261,264 –266,269,272,276,277,279 –281,288,293,295 –300,303,306,308,309,313,314,318,319,321 –323,328,331 –335,342,344,346,347,350 –356,359,361 elucidating the precise elements underlying BT’s effects remains a significant challenge crucial to designing appropriate controls. Closing these gaps will be essential for future efficacy and mechanism research.
Clinical research reporting
As evidenced by this review, one of the primary challenges within the current evidence landscape for BTs is the lack of uniformity in reporting study methods and outcomes. This inconsistency is likely hindered by the complex nature of real-world practice including the uncertainty surrounding the optimal dosage and delivery methods. 2,371 This deficiency inhibits the meaningful aggregation of data across studies due to the heightened risk of bias. Despite the extensive literature base, which encompasses 353 clinical trials, including 255 RCTs, a significant obstacle to evaluating the evidence base persists due to the lack of comprehensive description and standardization in reporting biofield interventions. Incomplete details of experimental procedures can impede replication and understanding of interventions’ effectiveness, hindering the ability to pool results and conduct systematic evaluations to assess BT efficacy for specific outcomes.
In response to this challenge, Biofield Therapies: Reporting Evidence Guidelines were developed in 2024. 371 We strongly urge future researchers to adhere to these guidelines, with particular attention to describing details of the delivery methods of BTs, including local applications with hands-on and hands-off techniques, as well as distant interventions, each of which may involve different mechanisms and influences on study outcomes. Such complete descriptions will expedite meaningful comparisons across studies and mitigate the risk of bias in reporting, ultimately enabling the pooling of results.
Evidence Map
The EM was developed to help various stakeholders navigate inquiries about the clinical effectiveness of BTs. As these therapies are increasingly used in hospitals globally, the EM was designed with interactive features to improve accessibility and usability. Consideration was given to ensure that the EM could be effectively utilized by diverse audiences with varying levels of understanding of research methods and design.
Targeted and rigorous research is essential for the scientific validation of BTs. Initiatives such as this EM aim at increasing awareness of the evidence base and comprehensively understanding the current state of scientific knowledge on BT and can help identify gaps and optimal avenues for future investigation. By addressing these needs within the field, evidence-informed strategic decision-making can be facilitated for various stakeholders, including research funders, practitioners, patients, the general public, as well as health systems policymakers.
Review limitations
This review exclusively focused on articles published in English and peer-reviewed journals, potentially limiting the breadth of perspectives and insights available. As BTs have roots that span millennia and diverse cultural contexts, it is likely that non-English literature could offer unique insights and practices not captured within English publications alone. Therefore, expanding future reviews to include languages other than English and additional sources could provide a more comprehensive understanding of BTs and their applications across different cultures and regions.
This ScR did not conduct a risk of bias assessment, evaluate the clinical effectiveness of BTs for individual conditions, or pool statistical results to determine effect sizes. These steps are crucial for accurately evaluating claims about effectiveness and efficacy and informing clinical decision-making. However, the EM allows researchers and health policy specialists to assess whether specific areas of the existing evidence warrant a systematic review and meta-analysis. These limitations highlight areas for future research and methodological refinement in BTs.
As this was a ScR not intended to determine efficacy or effectiveness, the results were categorized based solely on what was reported in the Abstract, a common approach when dealing with a large evidence base like the one in this review. However, authors often selectively highlight key findings or emphasize specific aspects of their research in the Abstract, which may not fully represent the study’s comprehensive outcomes. As a result, some details or additional findings discussed in the full text of the articles may not have been captured, potentially affecting the overall interpretation of the evidence base.
This ScR and EM primarily focused on clinical literature and did not include other study designs. While clinical literature provides crucial insights into the efficacy, effectiveness, and safety of BTs, additional valuable information may be gleaned from alternative forms of evidence, such as case studies and pragmatic trials. These alternative sources offer unique perspectives on the effectiveness of BTs within real-world settings, shedding light on potential uses that may not have been fully captured by the clinical literature. Furthermore, real-world practice of these modalities may yield different outcomes, as clinical trials often restrict the practitioner’s freedom to deliver the intervention and vary its application—a constraint not typically encountered in everyday practice.
Moreover, the exclusion of preclinical literature from this ScR represents the absence of a major class of studies that explore the underlying mechanisms of BTs. Investigating preclinical studies could provide valuable insights into the biological mechanisms through which these therapies operate. Therefore, a future ScR focused on exploring mechanisms of BTs would need to encompass all available evidence, across various study designs.
Conclusions
There is a growing number of publications, increasing interest, and greater use and exploration of BTs among researchers, practitioners, and patient populations. Despite these trends and current evidence suggesting potential efficacy for various conditions, the integration of BTs as adjunctive care into the allopathic medical system has not progressed in large part due to inconsistent evidence supporting their effectiveness and efficacy. The situation can be attributed to the challenges in researching BTs, inconsistent reporting of evidence, limited understanding of underlying mechanisms, and a lack of clarity regarding the specific conditions and symptoms for which BTs may be most effective. By coordinating all the evidence within a dynamic EM, stakeholders will be empowered to learn about BT research, find effective ways to address the challenges hindering BT acceptance, and, most importantly, facilitate additional research to validate whether BTs are appropriate adjunctive treatment options in contemporary allopathic health care.
Footnotes
Acknowledgments
The authors acknowledge Sam Allen, Liscia Beenhakker, Hannah Biddel, Cara Dorchat, Noortje Ijssennagger, Ryesa Mansoor, Nida Paracha, Anisha Saddy, Ryan Sliwak, and Benjamin Smith for their contribution in screening. The authors thank Jackie Phinney and Francis Toole at Dalhousie University’s WK Kellogg Health Sciences Library for their assistance in running the database searches. The authors thank Natalie Dyer, Wayne Jonas, Dean Radin, Helané Wahbeh, and Garret Yount for their subject matter expertise and feedback on the definition of BTs and the therapies included, which was instrumental in determining our inclusion and exclusion criteria as well as the scope of this endeavor. The authors would also like to express gratitude to Alma Economics for their help and guidance in developing the searchable interactive dynamic EM.
Authors’ Contributions
M.L.S., L.T., and C.C. contributed to concept development and study design. M.L.S., L.T., and C.C. contributed to the literature search in conjunction with a health services librarian. M.L.S., L.T., S.A., N.I., and N.L.D. contributed to the abstract, title, and full-text screening for eligibility. S.A., N.I., and L.T. contributed to data extraction and data charting. M.L.S., L.T., and C.C. conceptualized and determined the features and filters of the E.M., M.L.S., and L.T. cleaned and formatted the data for the E.M., M.L.S., and L.T. drafted the article. All authors critically revised the article for intellectual content and contributed to article revisions. All authors approved the final article.
Author Disclosure Statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this article. M.L.S., L.T., S.A., N.I., N.D., and C.C. are consultants and have been paid by Inquiring Systems Inc.—The Biofield Collective through donations from the funders (acknowledged above), for work related to this article. Inquiring Systems Inc.—The Biofield Collective had no role in the writing or imposed any restrictions regarding the submission of this report for publication.
Funding Information
This project was generously funded by members of the Subtle Energy Funders Collective including the Emerald Gate Charitable Trust, the LightEn Educational Network, the Samueli Foundation, Jorge Moll, Ivy Ross, English Sall, and Jeffrey C. Walker, through grants to Inquiring Systems Inc.—The Biofield Collective.
Supplementary Material
Supplementary Data
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
a
In the EM, studies that compare different BTs (e.g. Seskevich et al. 230 ), involve participants receiving multiple therapies (e.g., Krucoff et al. 226 ), or are crossover studies where participants receive different therapies at different times (e.g., Wirth et al. 215 ) are represented in a bubble for each therapy. Consequently, certain studies may be represented more than once within the map.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.