
Abstract
Introduction:
Growing evidence suggests that acupuncture can improve pelvic pain in women with endometriosis. The treatments used in research vary considerably. It remains unclear which treatment could be recommended for clinical practice. This research project aimed at clarifying how acupuncture could be used when treating this condition.
Methods:
This research comprised two phases: a systematized literature review to extract acupuncture treatment details from published research, and an e-Delphi study to gain knowledge about details as used by expert acupuncturists.
Review:
Four databases were searched using predefined eligibility criteria. Data were extracted based on the STandards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA) criteria.
e-Delphi:
Purposeful sampling from colleagues and international experts. An open first round gathered qualitative data, analyzed with the Framework method. In rounds 2 and 3, experts rated statements to build group consensus, defined as a rating of ≥5 on a 7-point Likert scale by ≥70% of the experts. The strength of agreement was graded using the median score and interquartile range. Results from the literature review and the e-Delphi were compared using the STRICTA items.
Results:
The literature review (n = 29 unique studies) found a wide range of treatment details with little agreement. The e-Delphi of international experts (n = 20) resulted in agreement on 94 statements (such as key factors for effectiveness); disagreement on a further 29 (such as acupressure); and absence of consensus on 55 statements (such as the number of needle insertions). A comparison of the review and e-Delphi results found little agreement.
Conclusions:
Details of acupuncture treatment for endometriosis-related pelvic pain were presented. In the absence of acupuncture guidelines for this condition, the researchers of this e-Delphi recommend using the treatment details on which experts agreed as guidance for good practice. The effectiveness of these guidelines should be evaluated in future research.
Clinical Trial Registration:
Deutsches Register Klinischer Studien, DRKS00022215, June 30, 2020, retrospectively registered.
Introduction
Endometriosis is defined as the presence of endometrial tissue outside the cavum uteri, with a prevalence of ∼10% in the western countries. 1 The most frequently reported symptom is pelvic pain, 2 leading to annual costs per woman around 10,000$ and significant impairment in quality of life and mental health. 3,4
Conventional treatment options for pain reduction include hormonal therapies, analgesics, and surgery. 5 Ongoing pain symptoms, significant side effects, or recurrence of symptoms after discontinuation of therapy limit treatment success, 5 and these suggest that further treatment options are required. 6 Guidelines refer to acupuncture as a potential treatment for endometriosis—stating that clinicians should ask and, if wished, discuss non-medical strategies such as acupuncture with women managing their endometriosis symptoms. However, guidelines criticize evidence quality and therefore reject a recommendation for any specific non-medical intervention. 5,7
Acupuncture involves the insertion of acupuncture needles in the body to cause changes. 8 The technique originated in TCM (Traditional Chinese Medicine), 9 which evolved over more than 2000 years and has developed its own theory. 10
According to a 2019 global report of the World Health Organization (WHO), acupuncture is the world's most widely used type of traditional and complementary medicine. 11 According to Schwartz et al, 12 359 (62.5%) out of 574 women with a confirmed diagnosis of endometriosis seek support from complementary medicine. Of all complementary health approaches and home remedies listed, “acupuncture/Traditional Chinese Medicine” were selected by approximately one-quarter of all participants. 12
There is growing evidence, including systematic reviews, supporting the use of acupuncture as an effective intervention to reduce pain scores in women with endometriosis. 13 –21 In addition, quality-of-life outcomes show significant improvements in the acupuncture groups. 14,15,18,19 None of the studies reported serious adverse events. However, study limitations include small sample sizes 20 and uncertain 14,15,18 or high risk of bias 14,18 in at least one category, as reported by Mira et al. 21
Despite searching Medical Literature Analysis and Retrieval System Online (MEDLINE), the Allied and Complementary Medicine Database (AMED), and the Database of Abstracts of Reviews of Effects (DARE), no guidelines could be identified to assist acupuncturists treating pelvic pain related to endometriosis in clinical practice.
An initial review of acupuncture treatment details in published research showed significant variations, including treatment duration ranging from 8 weeks to 24 months. 14,19 This research project aimed at examining how acupuncture has been used in research on endometriosis, and how experts in the field treat this condition, to define how acupuncture could be used in treating pelvic pain in endometriosis.
Ethical approval to involve experts in the Delphi process was given on June 11, 2020 and an amendment after a pilot test on September 15, 2020 by the Northern College of Acupuncture Research Ethics Committee.
Materials and Methods
This project comprised a systematized literature review and an e-Delphi study, followed by a synthesis of both results. Figure 1 provides an overview of the study process.
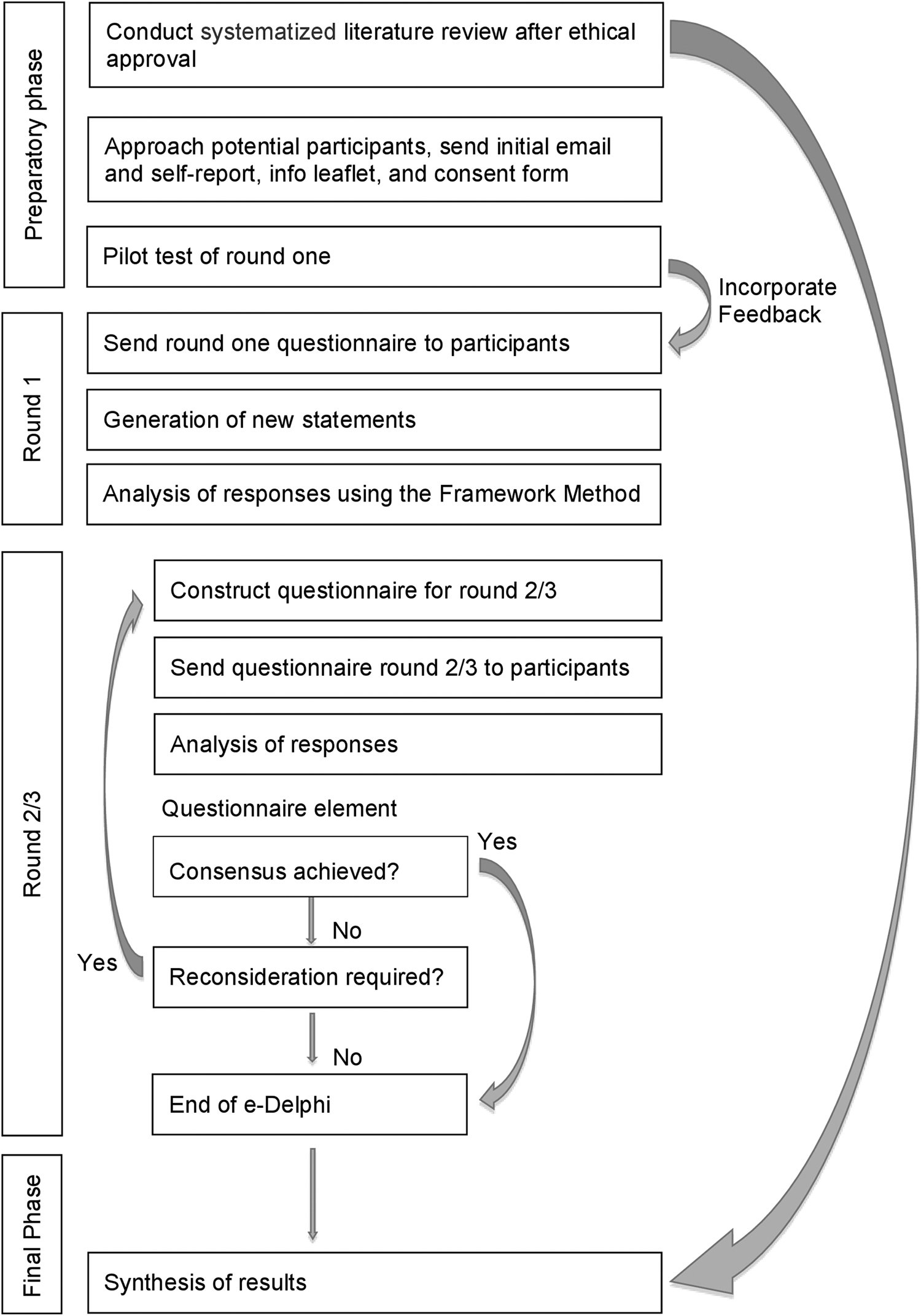
Overview of study process.
Systematized literature review
Systematized reviews share many strengths with systematic reviews and are more suitable for the lone researcher. 22 A comprehensive literature search was last conducted on 12/28/2020 on DARE (NIHR Centre for Reviews and Dissemination—CRD Database), the Cochrane Library (Cochrane Library website), MEDLINE (PubMed), and AMED (EBSCOhost) with the search terms “endometriosis” OR “adenomyosis” AND “acupuncture” OR “moxibustion” without any limits, restrictions, or search filters (Supplementary Data S1).
Patient Intervention Comparator Outcome Study-design (PICOS) was used to define inclusion/exclusion criteria, as presented in Table 1: 23 Women with pain and endometriosis receiving any style of acupuncture, study protocols, and all study designs that are based on patient data, limited to studies in English or German. Neither comparator nor outcome is relevant for this study that aimed at gathering details of acupuncture treatments in use, and both have therefore been omitted.
Inclusion/Exclusion Criteria for Screening Search Results
RCTs, randomized controlled trials.
Data were extracted from full-text publications based on items 1-4a of the STandards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA) criteria, 24 including the acupuncture rationale, details of needling, treatment regimen, and other components of treatment. STRICTA is a recognized standard for reporting acupuncture treatments in research and is an official extension of the CONsolidated Standards Of Reporting Trials (CONSORT). 25 The literature review has been reported according to Preferred Reporting Items for Systematic reviews and Meta-Analyses literature search extension (PRISMA-S) checklist. 26
e-Delphi study
An e-Delphi study is a data collection method to seek consensus among a group of experts, administered by e-mail. 27 Its use is based on the assumption that group consensus is more valid than individual opinion. 28 It was the most suitable research method for an international expert panel convened without financial support. The Guidance on Conducting and REporting DElphi Studies (CREDES) was implemented to ensure methodological rigor. The implications of using CREDES are shown in Table 2. 29
Features of This Study That Were Based on the Conducting and Reporting Delphi Studies Guidance
Recruitment
Recruitment consisted of purposeful sampling by personal acquaintances, recommendations, internet search, and snowballing. As sample sizes in Delphi studies vary and the majority reported 11–25 participants in their final round, 30 50 international acupuncturists were invited to take part. Eligibility criteria for expert selection were predefined as: practicing or recently retired acupuncturists who self-reported treating endometriosis-related pelvic pain for a minimum of 5 years with at least two patients/week; ability to understand and communicate in English; access to e-mail.
Recruitment took place between June and September 2020. Participants provided written consent for participation. They could withdraw at any time until the end of data collection. The participants remained anonymous to each other during the study. Permission was obtained to be acknowledged by name in this publication.
Study design
The e-Delphi study was limited to three rounds because of practical time constraints and to minimize participant attrition. 27 Given that there are no strict guidelines on the definition of consensus in Delphi studies, a level of 70% was used, as proposed by Keeney et al. 27
The Delphi study was conducted independently from the literature review. No information about the review results was provided to the participants. In an open first round, participants were asked for treatment details they use in clinical practice based on items 1–4a of the STRICTA categories. Rounds 2 and 3 built upon the statements generated in round 1 of the Delphi process to gain consensus among experts. Items that had been missed by experts in round 2—and that left the item on a threshold of inclusion/exclusion—were included again at round 3.
Data analysis
Qualitative data from round 1 were analyzed with the Framework Method to generate statements. 31 In rounds 2 and 3, participants were asked to rate the statements to gather group consensus predefined as ≥5 on a 7-point Likert scale by ≥70% of the experts. The strength of agreement was graded post hoc using the median score and interquartile range, as shown in Table 3.
Criteria for Grading the Strength of Agreement
IQR, interquartile range.
Synthesis
The review and e-Delphi results were compared using items from the STRICTA checklist as a framework.
Results
Systematized literature review
Ninety-four papers were identified, and 83 were screened after removal of duplicates. After excluding 19 due to language restrictions and another 48 for various reasons (Fig. 2), 16 papers were included.
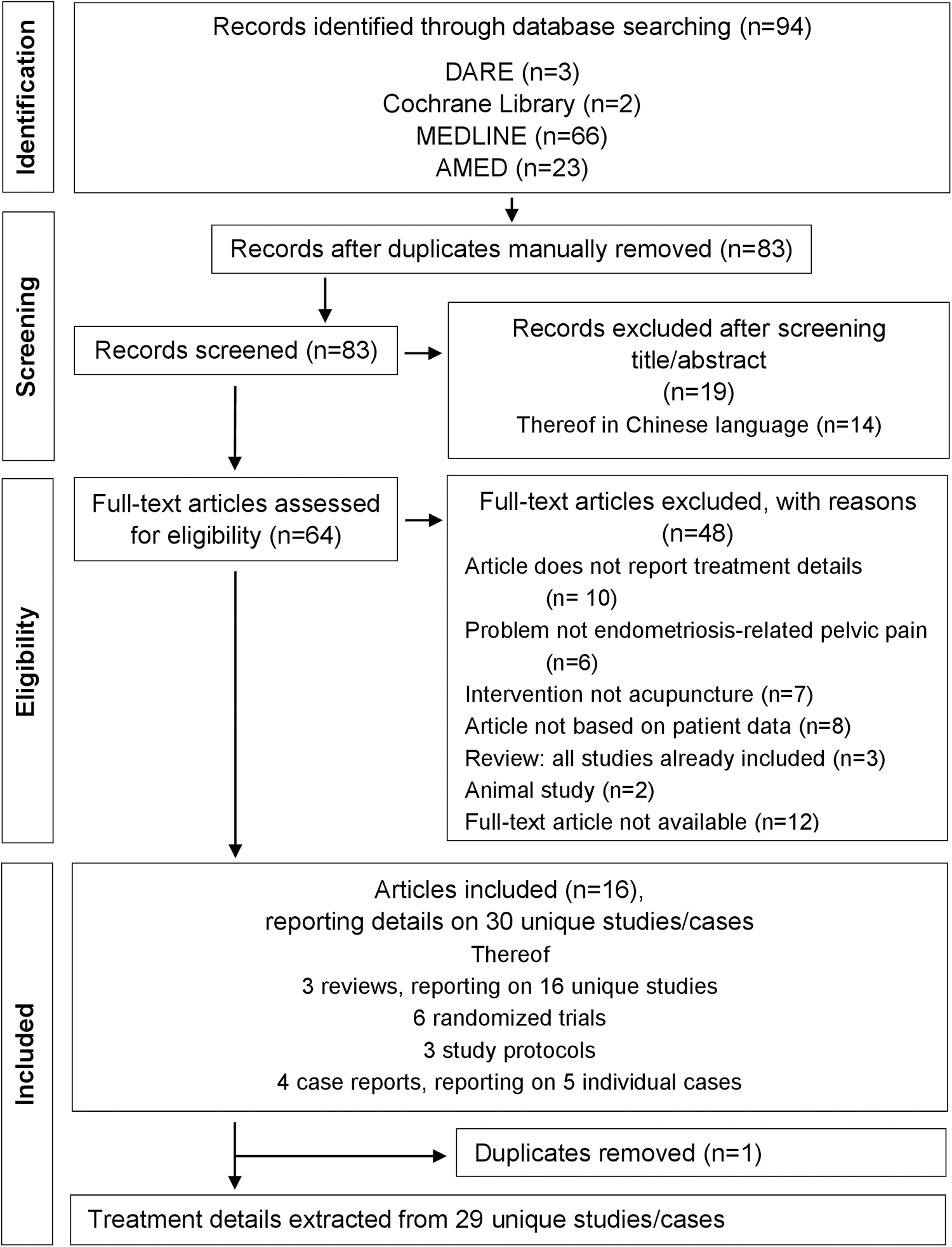
PRISMA flowchart of study selection and results. AMED, The Allied and Complementary Medicine Database; DARE, Database of Abstracts of Reviews of Effects; MEDLINE, Medical Literature Analysis and Retrieval System Online; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
The 16 papers included reported on 29 unique studies/cases: randomized trials (n = 15), study protocols (n = 3), observational studies (n = 3), unique cases (n = 5), and studies with unclear study design (n = 3). The study characteristics of the included studies are presented in Table 4.
Study Characteristics of Included Studies
RCT, randomized controlled trial.
Overall, there was little information available on treatment details, especially from studies reported only in reviews (comprehensive in Supplementary Data S2). For example, 13 out of 29 studies did not report on the acupuncture style used, 19 of 29 lacked information on the number of needle insertions, and 25 of 29 did not report whether acupuncture needles were inserted uni- or bilaterally. It was, therefore, impossible to identify common treatment details that could guide clinical practice based on the research literature.
e-Delphi study
Due to the lack of information on treatment details in published research, it was impossible to conduct the Delphi study based on the literature review. Both the literature search and the Delphi process were, therefore, conducted on the basis of the STRICTA criteria, but completely independently of each other. Of the 50 invited international expert acupuncturists, 21 indicated interest in participating, 1 of whom was excluded based on the eligibility criteria. Twenty were included. Table 5 shows the characteristics of the included participants. There were no dropouts.
Characteristics of Recruited Participants
TCM, Traditional Chinese Medicine.
Delphi rounds
Round 1
A total of 176 statements were generated in round 1 of the Delphi process. Figure 3 shows an example of how statements were generated. These statements contained detailed information beyond the STRICTA criteria.
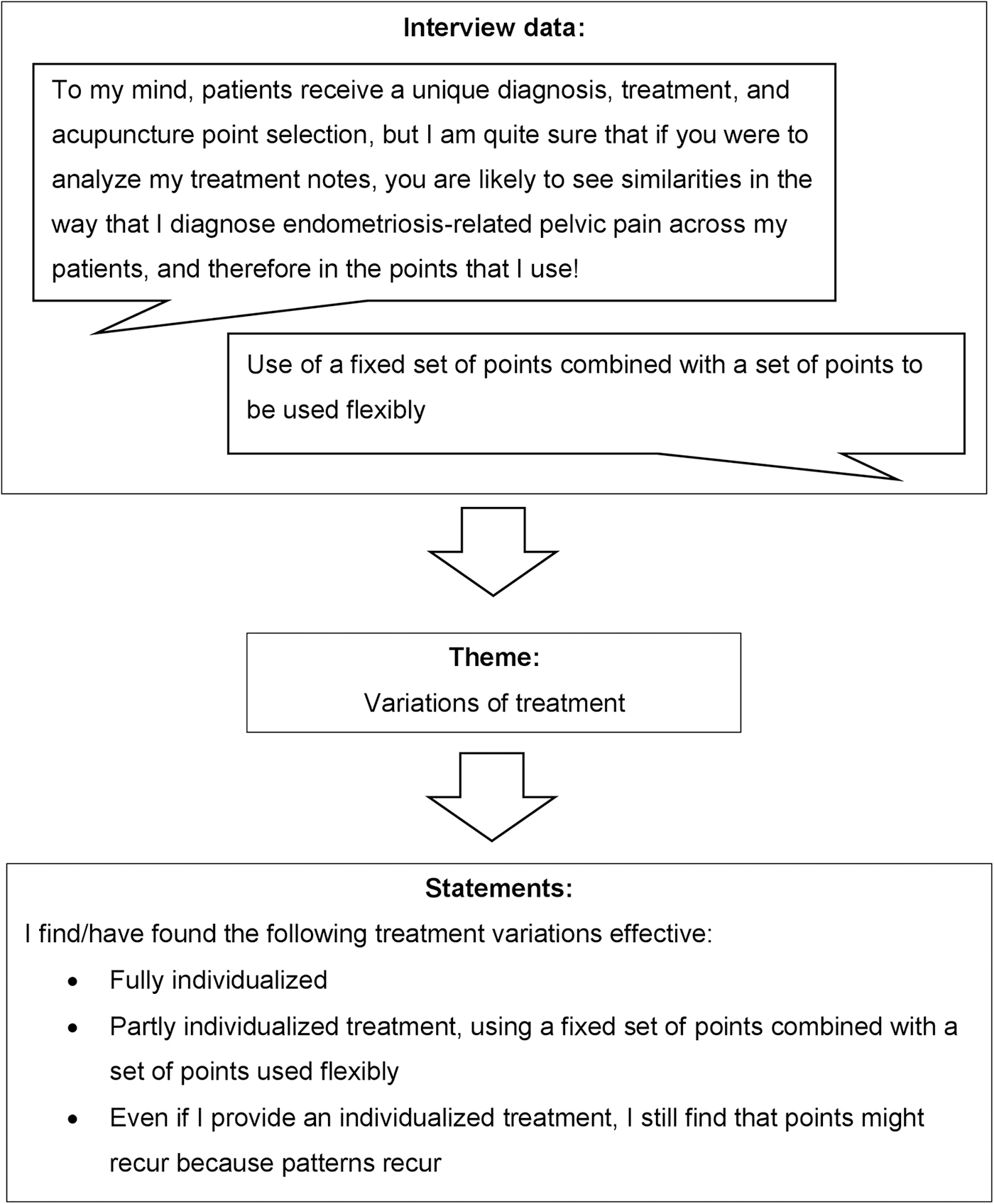
Example of statement generation.
Round 2
All statements provided to the experts in rounds 2 and 3 were anonymized. In round 2, 92 out of 176 statements reached consensus (pre-defined as a rating of ≥5 on a 7-point Likert scale by ≥70% of the experts), of which 79 found consensus for use, whereas on another 13, experts found consensus against use.
Missing data was an issue in round 2. Even though all experts returned the questionnaire, 13 out of 20 experts failed to rate at least 1 element. Missing ratings could have affected the results, and these statements were therefore also included in round 3.
Round 3
The final round included 86 statements that did not reach consensus in round 2. Participants received the overall ratings from round 2 and were asked to reconsider their ratings in round 3. Thirty-one reached consensus, of which agreement for use was reached on 15, and agreement against use for another 16. Fifty-five statements did not reach consensus. Only three ratings were missing in the final round.
Synthesis
Overall, a comparison of review and e-Delphi results found little agreement, largely due to missing information in published research and the synthesis remained incomplete. The results of the synthesis are detailed in Supplementary Data S3.
Comparing what has been done in research and what acupuncture experts stated in the e-Delphi process, two clear discrepancies appeared: Panelists stated that the individualization of treatments and the application of critical factors for effectiveness, namely the additional use of Chinese herbal medicine and giving dietary advice, are key. In research, only 6 out of 29 provided an individualized treatment and Chinese herbal medicine was used in only 5 out of 29 studies.
Summary of final results
The e-Delphi study produced three types of results (comprehensive in Supplementary Data S4): Statements where at least 70% of participants agreed on their use (94 statements), statements where at least 70% participants agreed against their use (29 statements), and statements for which no consensus was reached (55 statements).
Provisionally recommended for use
The following treatment details found consensus for use and strong or moderate agreement within the Delphi process and are recommended to treat pelvic pain in endometriosis. Table 6 summarizes treatment details by STRICTA criteria.
Provisional Recommendations for Use in Clinical Practice
TCM, Traditional Chinese Medicine; TDP, Teding Diancibo Pu (special lamp used in TCM, which operates in special electromagnetic spectrum).
Practitioners should consider using TCM-style, Master Tung- and electroacupuncture, or combinations of various styles, in an at least partially individualized approach. Thirty-one acupuncture points are provisionally recommended in this context. Uni- or bilateral needling was felt to depend on the individual, although bilateral needling was usually recommended for points on the abdomen and back. An individualized approach be taken is provisionally recommended for the depth of needle insertion depending on the individual (within the range recommended in the standard literature), and whether to seek a qi response and stimulate the point depending on the point and situation.
Provisional recommendation for needle retention time is about 30 min using medical stainless-steel needles of a diameter and length dependent on the patient's body and anatomy. A treatment frequency of once to twice a week for at least 2–3 months is provisionally recommended, continuing until pain relief is achieved, supplemented by a number of other treatment components such as the use of Chinese herbal medicine, moxibustion, and qigong breathing exercises.
Essential treatment details that reached consensus for use: Practitioners should consider adding Chinese herbal medicine and dietary advice for treating women with endometriosis-related pelvic pain, as both were rated as key factors for effectiveness.
Other miscellaneous recommendations include that practitioners should not reduce the treatment to blood stasis. Blood stasis is the most frequently reported syndrome in endometriosis, 42 arising from lack of movement and consequent stagnation in TCM conceptualization of blood. 43 A treatment according to syndrome differentiation is crucial to maximize the efficacy of TCM-treatment. 44
Further, e-Delphi experts found agreement that blood stasis is always a branch, and practitioners need to treat the base root as well. The root and branch theory (called Ben and Biao) is common in TCM and means that the underlying pattern that led to the diagnosis of blood stasis also needs to be addressed. 45 –47
Moreover, it is provisionally recommended to combine local and distant points, provide treatment throughout the menstrual cycle, evolve it accordingly, and adapt it to comorbidities such as infertility. In severe cases, frequency can be increased around menstruation and ovulation. If heat improves the pain, the provisional recommendation is to use heat, even if the tongue shows signs of heat. It is suggested that the treatment should also aim at helping the patient to achieve emotional balance.
Not recommended for common use
Consensus against use was found for 29 statements, such as scalp acupuncture, 8 acupuncture points, and a range of additional components of treatment such as vaginal steaming or acupressure.
Where guidance could not be developed
Fifty-five statements did not reach consensus, including the number of needle insertions per subject per session and the number of treatment sessions.
Limitations
Limitations of the literature review included the restriction to German and English literature. Bias, including mistakes, may have arisen from the researcher (N.G.) working without a second reviewer. 48
The main limitation of the e-Delphi-study is inherent in the method itself, as even a panel with an adequate level of expertise might come to other conclusions due to differences in their backgrounds. 49 Mitigation included the international diversity of participants, their relatively high level of expertise with full participant retention through all three rounds.
Discussion
Initially, the aim of synthesizing the results of the review with those of the e-Delphi was to develop guidelines for good practice based on what has been used in published research and what gained consensus in the e-Delphi process. Published research indicates that acupuncture treatments for endometriosis-related pelvic pain are generally effective, 13 –21 although the quality of evidence is limited. Expert opinion data provide details but cannot provide information about effectiveness, and therefore the guidance on good practice emerging from this e-Delphi study is provisional pending further studies on the effectiveness of this guidance.
Level of consensus versus strength of agreement
The level of consensus (defined as a rating of ≥5 on a 7-point Likert scale by ≥70% of the experts) is not necessarily equivalent to the strength of agreement (using the median score and interquartile range). Theoretically, the strength of agreement can be low, even in cases where there is a level of consensus of 100%, if all experts rated 5 on the Likert scale. Compared with the less precise level of consensus, using the median and the interquartile ranges mirror the typical rating and have therefore been added post hoc in this research project.
Findings in the context of previous research
Clinical guidelines in conventional medicine provide concrete and specific recommendations for clinical practice, 50 and they are usually developed from systematic reviews/meta-analysis or high-quality randomized controlled trials. By contrast, evidence summaries in acupuncture tend to report effectiveness, without providing sufficient information on how the treatment should be applied in detail. 51 Insufficient reporting of treatment details is a significant problem in acupuncture research, as has been shown by the present study.
Expert opinions such as committee reports, opinions, or clinical experiences of respected authorities are generally ranked at the bottom of the evidence hierarchy. 52 Nevertheless, the fact remains that group consensus is superior to a single expert opinion and as such plays a major role in medical science: Widely applied reporting guidelines such as the CONSORT statement or PRISMA were formulated on group consensus alone. 53,54
The Delphi technique is a commonly used method in other fields of medicine such as mental health or nursing to use expert opinion to build group consensus to inform clinical guidelines. 25,55 However, when used in the development of clinical guidelines, Delphi studies usually combine findings from systematic reviews with expert opinion. 56,57 In conclusion, where there is a lack of high-quality research from the top of the evidence hierarchy to inform clinical guidelines by providing information on treatment details, it may be helpful to explore treatment details based on a consensus method such as the Delphi technique.
In this e-Delphi study, expert acupuncturists agreed that at least partly individualized approaches should be used. However, even Delphi studies in TCM have struggled to capture details of the individualization of treatments. For example, Flower et al reported that experts used a range of 50–150 g of dried herbs/day for women with endometriosis, without providing advice regarding the cases in which to use 50 g and those requiring an increased amount. 42 Likewise, Lai et al reported having focused on “fundamental principles” (p. 436) such as “individualized herbs are more effective than standardized herbs” (p. 437)—rather than giving detailed information. 58
The need for an individualized treatment is hotly debated in TCM, mainly in research. Overall, research comparing the effectiveness of an individualized versus a standardized TCM treatment approach shows divergent results. 59,60 Nevertheless, a debate on individualized versus standardized treatments would be over-simplifying: this depends on the nature of treatment aspects. For example, the use of TCM-style acupuncture can be used by default without individualization, as the e-Delphi study shows; however, specific aspects of needling, such as when to use which acupuncture point, are issues that require an individualized approach.
Recommendations for future research
Even though the individualization of treatment is recommended, it remains unclear which factors lead to which specific needling detail. It is recommended that future research takes up the challenge of defining determining factors for individualization. Qualitative research using individual interviews would be appropriate, as they are likely to provide more detailed information than surveys or focus groups. 61
Assessment of the effectiveness of the treatment details reported in this e-Delphi study, taking into account the critical factors for effectiveness identified in this project (additional use of Chinese herbal medicine and giving dietary advice). It is suggested to use a pragmatic controlled trial study design, which is the best way of evaluating effectiveness under real-world conditions, 62 comparing three groups: a whole-systems intervention based on the provisional recommendations of this study versus standardized treatment versus no treatment. Hullender Rubin et al have investigated the effectiveness of whole-systems TCM on infertility, emphasizing that even and especially effectiveness research should reflect what practitioners are doing in the real world as effectiveness research does not reflect the capabilities of TCM when reduced to single interventions. 63 The request for a whole systems intervention is consistent with what acupuncture experts reported in this e-Delphi and is in line with the request of the Society for Acupuncture Research in 2007. 64
Conclusions
This research project intended to establish clinical practice guidelines for the treatment of pelvic pain in endometriosis based on a comprehensive literature review and an e-Delphi consultation with experts. The review of published research identified insufficient reporting of treatment details. Therefore, provisional guidelines were developed from the e-Delphi (comprising 20 international acupuncture experts) alone.
These provisional guidelines include the style of acupuncture, details of needling, a number of acupuncture points, the treatment frequency and duration, as well as other components of treatment. The e-Delphi also highlighted elements outside of the STRICTA elements as being critical for effective treatment (whole-systems treatment, including the usage of Chinese herbal medicine and dietary advice).
The authors offer these treatment details as an initial attempt to fill the gap in guidance for practitioners in this field. Expert opinion data do not inform on the effectiveness of specific treatment details, and therefore these guidelines should be considered as provisional.
Future research should explore the constitutional factors for individualized treatment aspects and evaluate the effectiveness of these provisional guidelines using whole-systems TCM.
Availability of Data and Materials
The anonymized datasets generated and analyzed during the current study are available from the corresponding author on reasonable request. Unanonymized data such as self-reports are not publicly available but are, however, available from the corresponding author on reasonable request and with permission of the participants.
The datasets supporting the conclusions of this article are included within the article (and its Supplementary Data).
Footnotes
Acknowledgments
The authors acknowledge with appreciation the contributions of the experts who took part in this e-Delphi study: Mike Armour, Young-Ju Becker, Naava Carman, Jeanelle Ji Chen, Martine Cornelissen, Peter Kington, Lily Lai, Anita Lienhard, Paddy McBride, Song MiDeok, Christophe Mohr, Jessica Noll, Wang Peng, Olivia Pojer, Caroline Radice, Lee Hullender Rubin, Keren Sela, and Fransiscus Sulistyo Winarto.
Authors' Contributions
N.G.: Conceptualization, methodology, project administration, investigation, formal analysis, writing—original draft. M.K.H.: Writing—review and editing, supervision.
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
No funding was received for this study.
Supplementary Material
Supplementary Data S1
Supplementary Data S2
Supplementary Data S3
Supplementary Data S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.