
Abstract
Background:
Objectives of soft tissue mobilization applied to cesarean section (C-section) scars are to decrease stiffness and to reduce pain. Research investigating these effects is lacking.
Materials and methods:
The authors conducted a descriptive, exploratory, proof-of-concept clinical study. Women aged 18 to 40 years who had undergone at least one C-section were recruited. A trained osteopath performed standardized mobilization of the C-section scar once a week for 2 weeks. Scar quality and pain characteristics, viscoelastic properties, pressure pain thresholds, and tactile pressure thresholds were measured before and after each session. Paired Student's t-tests and Friedman's test with Dunn–Bonferroni adjustment were performed to assess the immediate and short-term effects of mobilizations. Kendall's W and Cohen's d were calculated to determine effect sizes over the short term. Simple bootstrapped bias-corrected and accelerated 95% median confidence intervals were computed.
Results:
Thirty-two participants completed the study. The Patient and Observer Scar Assessment Scale questionnaire revealed differences with small and moderate effects for stiffness (p = 0.021, d = 0.43), relief (p < 0.001, d = 0.28), surface area (p = 0.040, d = 0.36), flexibility (p = 0.007, d = 0.52), and participant opinion (p = 0.001, d = 0.62). Mobilizations increased elasticity (p < 0.001, W = 0.11), decreased stiffness (p < 0.001, W = 0.30), and improved pressure pain thresholds (p < 0.001, W = 0.10) of the C-section, with small to moderate effects. The results also showed decreased tone and mechanical stress relaxation time, as well as increased tactile pressure thresholds at the different measurement times (p < 0.05), but trivial effect sizes (W < 0.10). Creep showed trivial effect and no significant difference (p = 0.09).
Conclusion:
This study showed that two sessions of mobilization of C-section scar might have a beneficial effect on some viscoelastic properties of the C-section as well as on pain. Some variables of interest useful for future empirical studies are highlighted.
ClinicalTrial. Gov NCT04320355.
Introduction
Cesarean section (C-section) is one of the most performed incisional surgeries in the world and represents a quarter of all births in Canada. 1 Scar adhesion and intraperitoneal adhesions are among the most common complications of obstetric surgery. 2 Hesselman et al. report that the adhesion rate could be as high as 32% if one or more C-sections were performed. 3
Scar adhesion is defined as an abnormal formation of fibrous tissue between two tissues or two organs. Known postoperative scarring complications include hypertrophic scarring, keloid and scar adhesion, and the incidence of excessive scarring after C-section is reported to be around 41%. 4 –8 Adhesions can occur superficially, at the scar site, and these can result in persistent pain and discomfort such as tugging in the lower abdomen. 9
Treatments of C-section scars include laser therapy, scar resection, hormonotherapy, and different forms of manual therapies. Clinical practice guidelines support scar massage as a conservative treatment of postsurgical scars; however, the lack of consistency about when to initiate treatment, the optimal technique, and dosage might be a barrier to the integration of this therapy into current practice. 10 Possible effects of manual therapies at the tissue level may be observed as decreased stiffness and associated discomfort or pain, increased mobility between tissue layers, and changed tissue viscoelastic properties. 11,12
The modification of viscoelastic properties by external manual stress or strain might explain how changes in scar tissue occur at the cellular level, possibly due to mechanotransduction. 12 –14 Although manual therapy studies on C-section scars show encouraging results in scar mobility 15,16 and thickness, 17 underlying mechanisms by which these therapies improve tissue viscoelastic properties remain to be explored. 14,15,17
Manual therapies to treat C-section scars may also act on sensory mechanisms. Several sensory receptors and nerve fibers are located and intertwined through collagen fibers of the skin and subcutis. 18 –21 Located at different levels in the loose connective tissue, the mechanoreceptors confer perceptions of the intensity and the orientation of mechanically induced tissue stress and strain, while the nociceptors may be a source of local and referred pain. 22
Structural alterations of the skin and subcutis tissues with scarring result in reduced mobility and viscoelasticity that could cause compression of the sensory receptors and nerve fibers and disrupt their signaling. The viscoelastic properties could potentially be modified when the skin and scars are stressed and/or strained by manual therapies and this can affect the sensitivity threshold of the mechanosensitive and nociceptive receptors. 23,24
The purpose of this study was to explore whether soft tissue mobilization sessions induced immediate and short-term changes in C-section scar viscoelastic properties, pressure pain thresholds, and tactile pressure thresholds. The potential effects of the intervention on the scar quality and sensory characteristics of the C-section from the perspective of participants and evaluators were also investigated.
Materials and Methods
Design
This proof of concept, 25 descriptive pre/post clinical study included four evaluation time points: at baseline (presession 1), immediate (postsession 1 and postsession 2), and short-term (before the second session) treatment. One of the most complex aspects of manual therapy is determining optimal dosage. This is particularly true when treating people with chronic scars due to the multifactorial mechanisms of the scaring and to patients' considerations. Moreover, the literature shows heterogeneity regarding the number, frequency, and the duration of soft tissue mobilization of the C-section scar. The dosage parameters were chosen according to the scar healing stage as well as clinical guidelines. 10,26
Participants
To be enrolled, women had to be aged between 18 and 40 years and to have one or more Pfannenstiel C-section scars. Pfannenstiel incision is the most common method for performing C-sections and consists of an horizontal line above the pubic symphysis. Women were excluded if they had (1) a vertical scar; (2) diabetes; or (3) undergone or were undergoing treatment for cancer over the previous 5 years. Women were recruited by using social media and posters displayed at three primary care perinatal and pediatric clinics in the Greater Montreal area, Quebec, Canada. Ethical approval was provided by the CRCHUS Ethics and Research Committee (no. 2020–3351). All participants signed an informed consent form before enrollment.
Procedure/data collection
The experiment took place in three perinatal and pediatric specialty clinics. After informed consent was obtained by the primary author, the participants entered an evaluation room equipped with a treatment table. Participants first completed the sociodemographics questionnaire, scar clinical characteristics questionnaire, and the Patient Scar Assessment Scale (PSAS) questionnaire.
Participants were then invited to lie supine on the treatment table and to undress the lower abdominal area so that the C-section scar was clearly visible. The research assistant placed a pillow under the participants' knees to ease any tension of the tissues surrounding the C-section scar. She identified five points along the C-section scar at 2 cm intervals and marked them with a nontoxic pencil. The research assistant proceeded to make the measurements on each of these points (Table 1). All evaluations and mobilizations were performed by two different individuals who were blinded to any information that could influence their respective task.
Evaluation Time Points
C-section, cesarean section; OSAS, Observer Scar Assessment Scale; PSAS, Patient Scar Assessment Scale.
Outcome and instrumentation
Scar quality and sensory characteristics
The Patient and Observer Scar Assessment Scale (POSAS) questionnaire was used to assess scar and pain characteristics of the C-section. The evaluator assessed seven items: pigmentation; vascularization; surface area; relief; thickness; pliability; and overall opinion. Participants reported seven items: pain; itching; color; stiffness; thickness; irregularity; and their overall opinion. 27,28 Each item is scored on a scale of 1 to 10.
For linear scars, the POSAS shows good internal consistency (Cronbach's α > 0.86). The POSAS subscale shows good reliability with respect to the total result of the items (intraclass correlation coefficient [ICC] 0.88 [0.84–0.91], p < 0.001 and ICC 0.96 [0.94–0.97], p < 0.001), the items separately (ICC 0.65–0.83 [0.55–0.88], p < 0.001 and ICC 0.85–0.94 [0.79–0.96], p < 0.001), 27 excellent inter-rater reliability (ICC 0.96 [0.94–0.97] p < 0.001), and excellent test/retest reliability (ICC 0.96) for transcultural adaptation. 29 The literature does not report any minimal clinically important difference value for this questionnaire.
Viscoelastic properties
The viscoelastic properties assessed using the MyotonPRO (Myoton SA) covered five parameters: (1) resting tone (Hz); (2) elasticity (damping of oscillation frequency); (3) stiffness (N/m); (4) creep (Deborah numbers); and (5) mechanical relaxation time (m/s). The MyotonPRO was placed and held stable on the scar over the points that were identified. The tip of the mechanical lever arm situated at one end of the MyotonPRO was positioned perpendicular to the plane of the scar. The device was preset to distribute five mechanical impulses to the scar. The choice of using the MyotonPRO for the evaluation of the viscoelastic properties of the C-section scar is based on the fact that the technology of this device measures all five viscoelastic properties in a single measurement compared with other tools used for scars. 30
For the C-section scar, the MyotonPRO has a good to excellent intra- and inter-rater reliability for all properties (ICC 0.91–0.99 [0.87–0.99]) and standard error of measure (SEM) of 0.44 Hz for tone, 0.08 for elasticity, 6.76 N for stiffness, 0.04 (Deborah number) for creep, and 0.67 m/s for mechanical relaxation time. 31
Pressure pain thresholds
The algometer (Wagner digital model FDIX, Wagner Instrument, USA) is a tool consisting of a spherical dial with a calibrated stem to determine the pressure pain or discomfort threshold. The algometer indicates the pressure threshold in N/cm2. The algometer demonstrates good to excellent intra- and inter-rater reliability for a C-section scar (0.88 [0.84, 0.91] and 0.74 [0.67, 0.80]). 18 Its criterion validity with respect to the Numeric Pain Rating Scale (r = −0.551, p = 0.002) has also been documented. The instrument has a relative measurement accuracy of ±4–5 N/cm2 for C-section. 18 The algometer has an intrarater SEM of 1.35 N/cm2 for subjects with C-section scars 18,32 and minimal detectable change of 3.74 N/cm2. 18
Tactile pressure thresholds
Tactile pressure thresholds were measured with the Von Frey monofilaments (VFMs). This instrument is used to study normal, hypersensitive, or hyposensitive skin areas in connection with a-beta fibers. The filaments, of different diameters, provide a range of strength from 0.008 to 300 g. For the skin of the abdominal region, VFMs show moderate intrarater reliability (κ 0.40–0.54) and moderate to satisfactory inter-rater agreement (κ 0.52–0.64). 33 VFMs show good intrarater reliability (Lin coefficients 0.76–0.86 [0.35, 0.95]) and good to excellent inter-rater reliability (Lin coefficients 0.72–0.91 [0.46, 0.97]).
Intervention
Soft tissue mobilization
Mobilization was performed with a custom-made glove equipped with a force sensor (FlexiForce sensor, Tekscan) integrated on the surface of the thumb and connected to a computer (Fig. 1). The mobilization consisted of a combination of compression and tension forces (shear stress forces), which can be clinically translated as gliding strokes. These were applied parallel and perpendicular to the C-section scar with the thumb of the experienced osteopath. The experienced osteopath was the author of this study. The mobilization was applied by the therapist on each identified point on the C-section scar for a total duration of 10 min (∼2 min per point, rate of application of 1 Hz).

Gloves equipped with a force sensor (FlexiForce sensor, Tekscan).
The intensity of the compression applied to the C-section points was adjusted according to the stiffness perceived subjectively by the therapist. When assessing the perceived stiffness of a given point, the therapist applied a compression stress of 10% above the stress value measured by the sensor and displayed on the computer screen. This procedure was used to standardize the mobilization to the variability of stiffness in each participant's tissues. 34,35 The same procedure was used once a week for 2 consecutive weeks by the same therapist.
Analyses
Analyses were performed using SPSS Statistics for MAC, version 26.0 (IBM, Armonk, NY). Descriptive analyses of sociodemographic and clinical characteristics were generated. For continuous variables, the authors report means and standard deviations (SDs) when the distribution was normal; otherwise, they report medians and simple bootstrapped bias-corrected and accelerated 95% confidence intervals. The advantage of this method is that it corrects for bias and skewness in the distribution and is a more efficient method with a small sample. 36,37
The Kolmogorov–Smirnov test was performed for testing the assumption of normality. Paired t-tests and Cohen's d were generated to assess the difference and effect size in scar quality and pain characteristics according to the POSAS. For Cohen's d, an effect size less than 0.2 is considered small, between >0.2 and 0.5 moderate, and between >0.5 and 0.8 large. 38 The short-term treatment effect sizes for all other outcomes were obtained using Kendall W's. Kendall's W < 0.3 is considered small, between >0.3 and 0.5 moderate, and >0.5 large. 39 Friedman tests with Dunn–Bonferroni adjustment were used to assess the differences overtime. All statistical tests of hypotheses were two-sided and performed at the 5% level of significance unless otherwise mentioned.
Sample size
The sample size was calculated assuming that the experimental measures followed a normal curve, with sensitivity to detect a medium effect size (Cohen's d = 0.5) in the pre/post difference of the different variables of interest, and to achieve a statistical power of 80%, with a type I error of 5%. Using these parameters, the sample size required was 32 participants. Anticipating a 10% dropout rate, 38 women were recruited.
Results
Participants' sociodemographic and clinical characteristics
Recruitment flow diagram can be found in Figure 2. Thirty-eight women were recruited between October 2019 and May 2020. Thirty-two women completed the two study sessions. The sociodemographic and clinical characteristics of the participants are listed in Table 2.
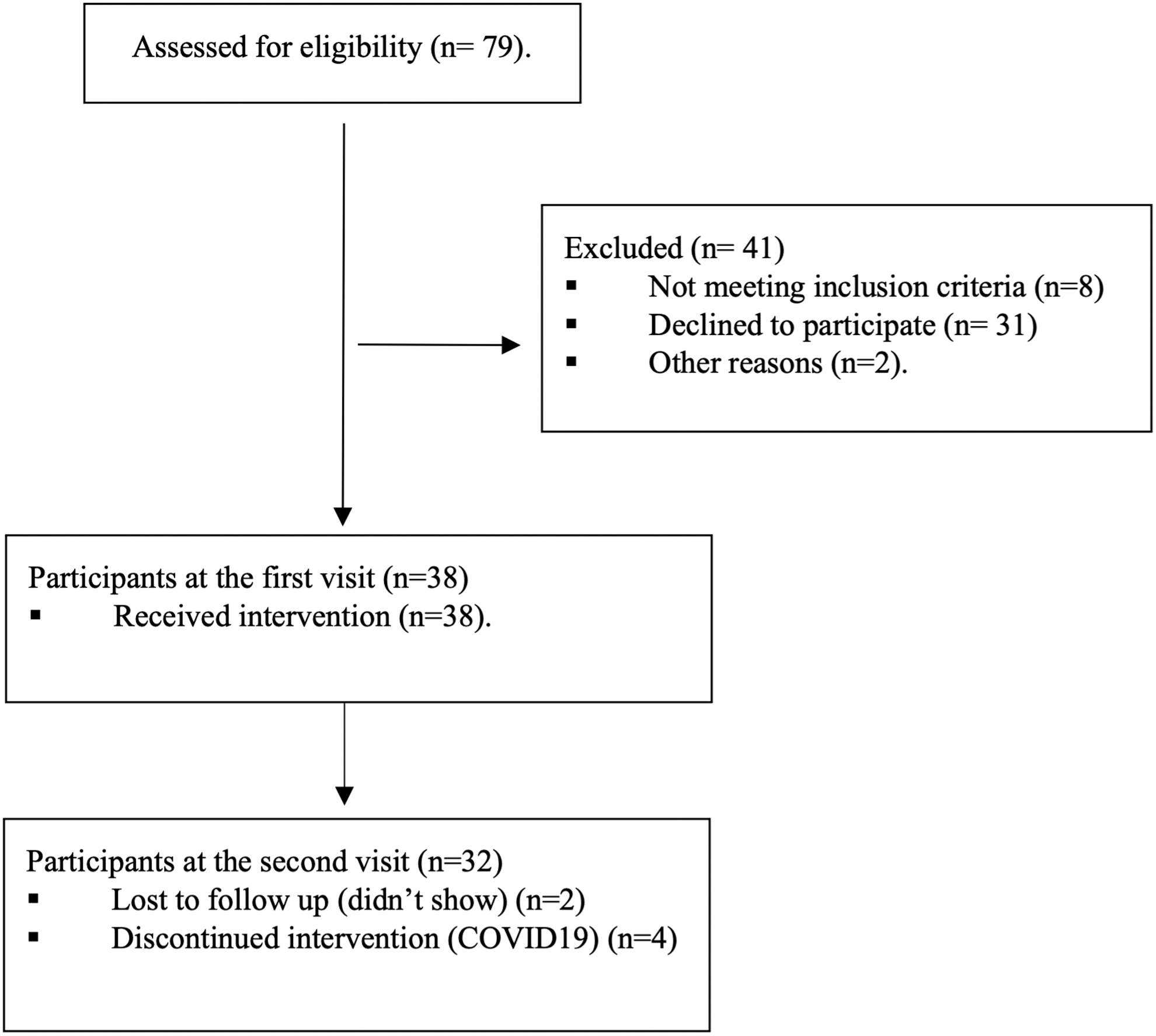
CONSORT flow diagram of the 79 participants assessed for eligibility for participation, 70 were eligible and 38 agreed to participate.
Sociodemographics, Clinical Characteristics of Participants, and Scar Characteristics
The participant demographic data and C-section characteristics are presented for all 38 who were recruited into the study. Data did not show any differences for the 32 participants who completed the study.
C-section, cesarean section; IQR, interquartile range.
Patient and Observer Scar Assessment Scale
Comparisons between the average values of all items of the POSAS can be found in Table 3. Paired t-tests revealed significant differences with small and moderate effects between results in stiffness (p = 0.021, d = 0.43), irregularity (p < 0.001, d = 0.69), color (d = 0.31), thickness (d = 0.30), and overall opinion of participants (p < 0.001, d = 0.62) for the PSAS. The mobilizations had small and moderate effects for pliability (p = 0.007, d = 0.52), surface area (p = 0.04, d = 0.36), pigmentation (d = 0.23), and relief (d = 0.28) for the Observer Scar Assessment Scale.
Comparisons Between Patient and Observer Scar Assessment Scale Presession 1 and Presession 2
CI, confidence interval; OSAS, Observer Scar Assessment Scale; PSAS, Patient Scar Assessment Scale; SD, standard deviation.
Viscoelastic properties
The results for all viscoelastic properties are presented in Tables 4 and 5. None of the viscoelastic property measures fulfilled the assumption of normality.
Descriptive Statistics for Viscoelastic Properties, Pressure Pain Thresholds, and Tactile Pressure Thresholds at Each Measurement Time
Results of session are reported with median and simple bootstrapped bias-corrected and accelerated 95% of median confidence interval.
Proportion of Individual Change That Exceeds Standard Error of Measure of the MyotonPRO
Frequency of 38 participants for postsession 1 (immediate effect) and of 32 participants for postsession 2 (short-term effect).
Tone
The mobilizations had limited effect on tone (W = 0.05). Friedman tests revealed a statistically significant decreased tone immediately after each session (p = 0.001 and p = 0.016, respectively) and over the short term (p = 0.002) with a median change of 0.35 Hz. This is below the SEM for the MyotonPRO, estimated to be 0.44 Hz.
Elasticity
Treatment had a small effect on elasticity, with Kendall W = 0.11. Friedman tests revealed statistically significant differences immediately after each session (p = 0.01 and p < 0.001, respectively), as well in the short term (p < 0.001), which corresponded to an increase in elasticity of median change of 0.09. This is slightly above the SEM value, estimated to be 0.08.
Stiffness
Mobilization had a moderate effect (W = 0.30) on stiffness, with a median decrease of 16.50 N/m. This is greater than the SEM for the tool, estimated to 6.76 N. Friedman tests revealed statistically significant differences immediately after each mobilization and over the short term (all p < 0.001) after Dunn–Bonferroni adjustment was applied.
Creep
Trivial effects on creep were observed (W = 0.06) over the short term, with a median increase of 0.02. Creep did not change statistically nor according to the SEM (estimated at 0.04) at any measurement times (all p > 0.05).
Mechanical stress relaxation time
Although statistically significant increases were observed immediately after the second mobilization (p < 0.001) and over the short term (p < 0.04), the median change of 0.39 m/s was clinically trivial (W = 0.05) and below the SEM estimated to be 0.67 m/s. Mechanical stress relaxation time did not increase immediately after the first session (p = 0.087).
Pain and sensory thresholds
Pressure pain thresholds
The mobilizations had a small effect (W = 0.10) on pressure pain thresholds. Improved pressure pain thresholds appeared to be delayed, as they were found to have significantly increased only over the short term (p < 0.001) with a median change of 1.70 N/cm2. This change is greater than the SEM value of 1.35 N/cm2 reported for the algometer.
Tactile pressure thresholds
The mobilizations had a trivial effect (W = 0.04) on tactile pressure thresholds. Friedman tests revealed statistically significant increases after the second session (p = 0.005). There was no statistically significant difference immediately after the first session and over the short term (all p > 0.05).
Compressive forces
A mean of 3.96 N (SD 1.44) of force was applied during standardized mobilization of C-section scar with a minimum of 0.90 N and a maximum of 7.42 N.
Discussion
Although manual therapy studies have explored the effects of soft tissue mobilization mobility and thickness, to our knowledge, this study is the first to establish quantifiable measures of the viscoelastic properties of the C-section scar. Stiffness and pressure pain thresholds were found to be the most responsive variables.
Scar stiffness continuously decreased after each mobilization and over the short term by 16.05 N/m. This decrease in stiffness is statistically and clinically relevant, with moderate effect (W = 0.30). Observations are consistent with the expected behavior as observed by Seliger et al., Buhimschi et al., and Kiener et al., 40 –42 who found that stiffness is present following a C-section, although they focused on uterine scars. The authors observed that stiffness is also present within the superficial scar tissue layers. Similarly, the POSAS tool demonstrated that both participants and the evaluator perceived a change in the items related to stiffness. Such convergence of data strengthens the hypothesis that soft tissue mobilization can modify stiffness.
Another variable of interest is the pressure pain threshold; they found incremental increases in pain threshold when pressure is applied to the C-section throughout the experiment. The incremental increases of 1.70 N/cm2 over the short term fall above the SEM report for the algometer of 1.35 N/cm2 and suggest that this variable could be considered clinically relevant regardless of the small effect (W = 0.10). 18 These observations are consistent with the findings reported in the literature and suggest that participants could tolerate more pressure after soft tissue mobilization. 15,18
A possible explanation for pain can be related to neural sensitization, which plays an important role in wound healing. This sensitization could have a lasting effect even after the remodeling and scar maturation phases. It has been shown that wound healing leads to increased innervation in the first weeks of scar composition and then gradually returns to normal or lower levels. 43
In the case of painful scars, it is plausible that a higher density of nerve fibers persists (such as in the case of adhesion) and that the different receptors responsible for the neural transmission of pressure are in much closer proximity. This proximity would lead to inappropriate cross stimulation and could result in an increase in the sensitivity of the region. 43 It is possible that the changes in viscoelastic properties brought about by the soft tissue mobilization, particularly the reduction of stiffness, could contribute to reducing this cross stimulation and thus modify neuronal messages.
Other observations following tissue mobilization include decreased tone and increased elasticity and mechanical stress relaxation time after the sessions. That said, although these variables showed statistical differences at all measurement times, the results do not exceed the SEM and were therefore trivial or small effects. To observe more significant changes in these parameters, more cycles of mobilizations, greater compression and/or shear force intensity, or longer mobilization times may be required.
Finally, concerning the tactile pressure thresholds, the participants experienced hypoesthesia after mobilization. These results are in line with Beyaz et al. 44 who identified hypoesthesia in 19% of women with Pfannenstiel incision scars, an average of 14 months after surgery. It is possible that stimulation of large-diameter afferent fibers, such as A-alpha, would block information from small fibers such as A-delta and C at the dorsal horn of the spinal cord level. Furthermore, clinical sensitivity studies of keloid scars show deficits characterized by a lower density of epidermal nerve fibers, and normal and mature scars appear to have less innervation than unscarred skin. 43
Limitations
The procedure used to evaluate tactile pressure thresholds may be subject to response and/or anticipation bias. To reduce the risk of response bias, the authors first explained to the participants how to respond to the stimulus by telling them when it was a direct sensation, as they kept their eyes closed for the duration of the test. It is also difficult to say if the mobilization could have an effect on the viscoelastic properties of the tissues that are deeper. Indeed, instruments used for this study only allowed them to observe changes in superficial tissue.
Implications for future research
Future studies should explore the mid- and long-term efficacy of mobilization of C-section scar tissue, particularly on stiffness and pressure pain thresholds. Studies with a greater number of sessions or mobilizations should be performed to examine whether the reduction of stiffness and pressure pain thresholds could be maintained and if other outcomes may be improved following additional mobilizations. Finally, the impact of age of scar and number of scars on the effects of soft tissue mobilization should be explored in future trials.
Conclusion
This study found that two sessions of soft tissue mobilization could have an effect on the viscoelastic properties and pain thresholds of C-section scars. This is the first study that the authors know of to demonstrate objectively the potential for the use of soft tissue mobilization to improve viscoelastic properties with treatment of C-section scars. This study provides sufficient evidence and variables of interest to move on to comparative study designs.
Footnotes
Acknowledgments
The authors thank all the women and research team members who participated in this study for their valuable contributions. They also thank Meg Sears for language editing.
Authors' Contributions
All authors, I.G., N.G., and I.G., participated in the conception and design of the study. I.G. participated in the acquisition, analyzed, and interpreted the data. I.G. provided the first draft of the article, and all authors, I.G., N.G., and I.G., participated in the critical revision and provided content to the final version. All authors, I.G., N.G., and I.G., approved the final version to be submitted.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was funded by the “Canadian Complementary and Alternative Medicine Research Fund” (CCRF) and the European Society for Research in Pediatric and Perinatal Osteopathy (SEROPP). These funding organizations did not participate in the elaboration of the study protocol and had no influence on the conduct of research protocol design, execution of the study, analyses, or authorship of findings.