
Abstract
Background:
With a peak incidence in the 10–19 years age group, acute appendicitis (AA) is the most common surgical emergency worldwide. The standard treatment procedure remains appendectomy to avoid complications such as its rupture, peritonitis, and sepsis. The COVID-19 pandemic required the global population to stay indoors to stop the spread of the virus, which led to a decline in the number of patients visiting the hospital for non-COVID–19-related emergencies.
Case Presentation:
This is a case of a 9-year-old girl who tested positive for COVID-19 and developed AA in the meantime and benefited from individualized classical homeopathy.
Conclusions:
Further scientific investigation is necessary to establish the prognostic factors in AA associated with COVID-19, and the relevance of individualized classical homeopathy in treating this complex condition.
Introduction
Acute appendicitis (AA) is the most prevalent surgical emergency worldwide, with an incidence of one case for every 100 persons annually and a peak incidence in the age range of 10–19 years. 1 With the rise in COVID-19 cases (over 703 million cases of COVID-19 being reported, by March 2024), 2 people were advised to visit hospitals only in case of COVID-19-related illnesses and non-COVID emergencies. Studies observed a decline in the number of patients visiting hospitals due to fear of the infection, leading to a reduction in the number of uncomplicated cases of appendicitis visiting hospitals, and increased usage of nonsurgical methods of intervention for various conditions, including antibiotic treatment for appendicitis. 3
The standard treatment procedure for AA is an emergency laparoscopic surgery. Although the procedure has high success rates, the associated risks and complications such as the need for reoperation, infection of the surgical site, and bowel obstruction often follow. 4
We present a case of AA associated with COVID-19 where resolution of the condition was observed while being managed with individualized classical homeopathy. The case report follows the CARE guidelines as presented in Supplementary Data S1.
Case Report
The patient, a 9-year and 10-month-old female, had a telephonic consultation with the homeopath on January 23, 2022. It must be noted that the patient’s mother was a pediatrician.
Presenting complaint
The child presented with a headache, nasal congestion, and sneezing initially. The next day, she developed a fever of 39°C with chills. She also complained of pain at the root of the nose with a barking cough, redness of both cheeks, vertigo, and drowsiness.
Past medical history
Episodes of acute bronchitis and pneumonia that required antibiotic and inhalant steroids at the age of 5 and 6 years. Multiple episodes of febrile upper respiratory tract infections had occurred between the ages of 4 and 7 years, and recurrent styes between the ages of 4 and 6 years.
Family history
The father had allergic bronchitis, and the mother had urticaria and allergic rhinitis. The maternal grandfather died of lung cancer, the paternal grandfather had skin cancer, and the grandmother suffered from systemic lupus erythematosus and psoriatic arthritis.
Homeopathic case history
As the fever developed, she sought constant care and attention from her parents and was in a teary mood. When inquired about it, she explained that she was scared of dying. Homeopathic repertorization of the symptoms at first intake is presented in Supplementary Data S2.
Prescription
Pulsatilla nigricans 200 CH, one dose
Pulsatilla was indicated by her psychological state, in which she was afraid of death as her acute symptoms worsened and, as a result, wept and demanded her mother’s constant attention, along with the physical symptom, headache located above the root of the nose. 5
January 24, 2022:
The fever subsided and the cough reduced significantly.
January 25, 2022:
The patient tested positive for COVID-19 when she was subjected to reverse transcription polymerase chain reaction as per the protocol, as her parents tested positive for the same. The patient was afebrile, without any respiratory symptoms at this point.
On the same day, she developed progressing pain in the right lower quadrant of the abdomen, associated with nausea at the sight of food, and two episodes of projectile vomiting.
The child wanted to pass flatus or stools as she felt the pain would ameliorate by doing so but could not succeed despite exerting pressure. The mother examined the child at home and found tenderness, guarding, and a positive Blumberg sign soon after which they visited the hospital for further assessment.
Laboratory findings:
Leucocyte count: 10,150 cells/uL (reference range [RR] 4500–11,000 cells/uL)
Neutrophilia: 88.8% (RR 40–60%)
Lymphopenia: 7.4% (RR 20–40%)
A high neutrophil-to-lymphocyte ratio (NLR): 12 (RR 0.78–3.53)
CRP: 4.85 mg/dL (RR <6 mg/dL)
Abdominal ultrasonography (USG) revealed an aperistaltic uncompressed segment reaching 7.6 mm in diameter in the peri-cecal area in the right lower quadrant of the abdomen, with an increase in echogenicity and minimal free fluid in the form of smearing in the adjacent omental tissue. Numerous well-circumscribed hypoechoic mesenteric lymph nodes, the largest of which was 15 × 9 mm in size, were observed in the mesenteric area in the right lower quadrant of the abdomen (as shown in Fig. 1).

USG abdomen as on January 25, 2022, revealing an aperistaltic uncompressed segment reaching 7.6 mm in diameter in the peri-cecal area in the right lower quadrant of the abdomen with an increase in echogenicity and minimal free fluid in the adjacent omental tissue. Numerous well-circumscribed hypoechoic mesenteric lymph nodes, the largest of which was 15 × 9 mm in size, were observed in the mesenteric area in the right lower quadrant of the abdomen. USG, ultrasonography.
Appendicitis inflammatory response (AIR) score: 9/12.
Diagnosis (ICD 10)
U07.1-COVID-19, virus identified.
K35.8-AA without mention of localized or generalized peritonitis. 6
Prescription
Based on the totality of the symptoms presented during the episode of appendicitis (repertorization in Supplementary Data S3), she was prescribed Natrum Sulphuricum 200CH, one dose, on January 25, 2022.
Follow-up
January 25, 2022:
After the remedy, the patient was able to sleep for about an hour, followed by an improved appetite and general condition. Nausea and abdominal pain decreased.
On auscultation, bowel sounds had increased, and she was able to pass flatus with ease within 3 hours.
The AIR score was 5/12.
January 26, 2022:
A follow-up abdominal USG revealed a hypoechoic tubular structure with a diameter of about 8.8 mm that does not change shape with compression, which is significant in terms of AA, as a diameter >5.7 mm is an optimal criterion in diagnosing AA in children. 7 A remarkable increase in inflammatory edematous echo in adjacent mesenteric fat planes and free fluid was also noted in the right lower quadrant (as shown in Fig. 2).
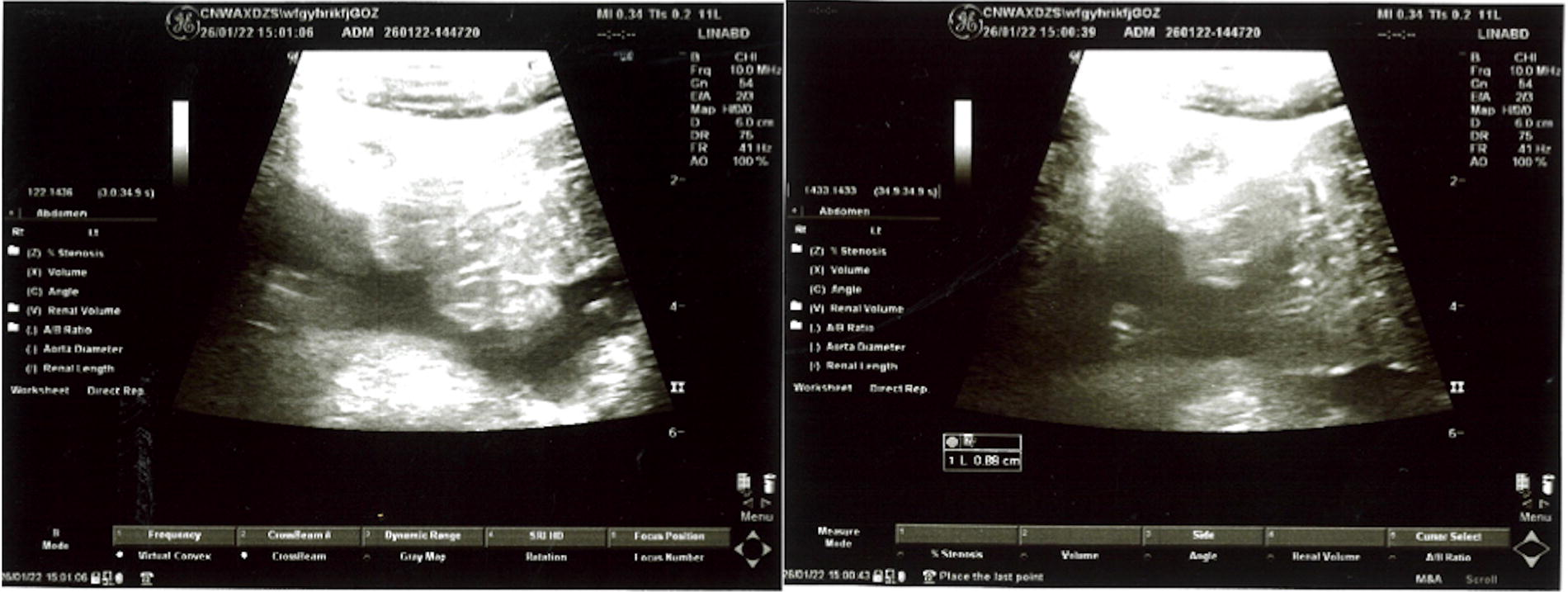
Abdominal USG as on January 26, 2022, revealing a hypoechoic tubular structure with a diameter of about 8.8 mm that does not change shape with compression, an increase in inflammatory edematous echo in adjacent mesenteric fat planes, and free fluid in the right lower quadrant. Several lymph nodes are noted in the mesenteric area, the largest being 16 mm. Abdominal CT with contrast on the same day shows an erect appendix of 1 cm diameter, with thick and opaque walls.
Laboratory findings:
Leucocyte count: 5200 cells/uL (RR 4.5–11,000 cells/uL)
Neutrophils: 66.7% (RR 40–60%)
Lymphocytes: 25% (RR 20−40%)
NLR: 2.66 (RR 0.78–3.53)
CRP was 64.53 mg/L (RR <6 mg/dL)
Emergency appendectomy was advised for the patient at the hospital, but as the pain and discomfort progressively decreased, the parents refused the surgical intervention. The child’s energy continued to increase, and she gained back her appetite.
The AIR score was 4/12.
January 28, 2022:
The patient had no complaints of abdominal pain, discomfort, constipation, or difficulty in passing flatus. Her appetite and energy were normal, and she was able to perform her day-to-day activities with ease.
February 26, 2022:
Control abdominal USG revealed an appendix of diameter 4.2 mm (RR: 4.2–12.8 mm), and several lymph nodes in the mesenteric area, the largest of which was approximately 14 mm in diameter, were observed (as shown in Fig. 3). No inflammatory signs of the appendix were noted in the control abdominal USG.

Control abdominal USG taken on February 26, 2022, revealing an appendix of diameter 4.2 mm, and several lymph nodes in the mesenteric area, the largest of which is approximately 14 mm in diameter.
The clinical course of the treatment is provided schematically in Figure 4 and the laboratory findings are compared in Table 1.

Clinical course, appendicitis inflammatory score, and individualized homeopathic treatment timeline.
NLR, neutrophil-to-lymphocyte ratio; USG, ultrasonography.
Discussion
Besides self-limiting symptoms such as nausea, vomiting, diarrhea, and anorexia a small number of patients developed gastrointestinal pathologies along with COVID-19 infection, including AA. The manifestations were hypothesized to be from direct viral injury/cytokine storm/inflammatory immune responses/alteration in gut bacteria due to imbalance in gut secretions/acute hypoxia/dysbiosis due to infection of the lung. 8 Furthermore, viral infections of the lung modify the gut microbiota composition and create a more proinflammatory state through disruption of the gut–lung axis, making the patient susceptible to inflammatory diseases of the gut. 9 Previous studies have shown the association between COVID-19 and AA, as viral infections could cause lymphoid hyperplasia of the appendix, leading to appendix obstruction and ulceration of the mucosa, resulting in secondary bacterial infection. Still, an association between COVID-19 infection and the development of AA is yet to be established. 10
Although she presented with high fever and cough 2 days prior to the development of abdominal pain, the patient did not have any other COVID-related symptoms.
Initially, Pulsatilla cleared up the fever and cough, and the inflammation got localized to the appendix. This is a phenomenon observed often, clinically (although no evidence has been recorded), during complex infectious states under homeopathic treatment, that the infection goes from being systemic to a localized one. This is the right direction and makes it simpler to treat the next issue (localized infection).
Furthermore, the patient’s blood report showed a high NLR of 12 suggestive of a high bacterial infection state, and less likely a viral infection. 11 Considering that NLR >8 is independently predictive of complicated appendicitis, 12 we can deduce that the girl is likely to have suffered from acute bacterial appendicitis. The first prescription for appendicitis (Natrum Sulphuricum) immediately brought about reduction in symptoms though the appendix was still inflamed as apparent from the USG next day. However, this also resolved, but it is not apparent in how long a period due to the lack of immediate follow-up USGs. But a significant decline in the NLR (12–2.66) was observed, and the follow-up abdominal USG (taken after a month), was also suggestive of complete resolution of AA.
Conventionally, the symptoms of malaise, tiredness, and sickness-related depression are given little consideration in terms of treatment, despite studies proving that they are strategically organized efforts of the neuroendocrine system to combat the infection. 13 In contrast, homeopathy considers these as vital, providing a holistic approach to sickness and health. 14 Homeopathic interventions have proven to be beneficial in treating chronic and debilitating conditions, but no scientific studies are available on treating AA.15–17 The studies available on treating COVID-19-associated appendicitis are minimal and have recorded the usage of conventional therapies for treating the same.8,11
Though surgical intervention still remains the gold standard, a study shows a higher mortality rate in individuals undergoing surgery with preoperatively diagnosed SARS-CoV-2 infection. 18 Also, recent studies have established that the appendix acts as a reservoir of commensal intestinal flora and as a site for host-symbiotic bacteria interaction. It also suggests a possibility that the appendix might have developed ahead of the cecum, implying that the immunological importance was established before the digestive one. 19 Thus, retaining the appendix might serve in replenishing the gut microbiota following its depletion due to causes such as antibiotic treatment, lifestyle changes, and dietary imbalances.
Although there is a possibility of spontaneous resolution in this case, the child showed remarkable improvement both symptomatically and in her general well-being within a span of 24 hours after the medicine, with recovery initiated within a few hours of it. A recent study conducted comparing the efficacy of antibiotics versus placebo in AA treatment showed the duration of sick leave being 4.7 and 5.3 days, respectively, 20 indicating a faster rate of recovery in this case. It is noteworthy that AA was managed without any conventional medicinal intervention, a significant feat for an overburdened health care system during the pandemic.
In this case, it must be noted that the patient was in constant care of a pediatrician, her mother, and an early detection and timely intervention worked in the favor of resolution of AA without its due progression to further complications. The mother, however, did not participate in the homeopathic treatment except to report the developments to the homeopath. Homeopaths in India are medically trained and hence qualified to handle such cases. It is not possible to replicate this without expertise. The main limitation of this case is that the applicability in a broader clinical sense is restricted to this peculiar scenario. Hospitalization may be necessary for most children with AA and more so if complicated by the presence of an infection such as COVID-19. The homeopathic prescription was based on the mother’s description and examination, which in this case was good enough, with the mother being a pediatrician. The mother was also able to monitor the case for any signs of danger and was constantly vigilant. In other children, such clear description, analysis, and monitoring of the condition may not be possible while at home. While internet consultation worked well in this case, this may not be adaptable to every case of AA.
The Modified Naranjo Criteria for Assessing Causal Attribution of Clinical Outcome to Homeopathic Intervention (MONARCH) score was assessed to be 8/13, indicating a likelihood of homeopathic intervention causing the benefit (Table 2).
Modified Naranjo Criteria for Assessing Causal Attribution of Clinical Outcome to Homeopathic Intervention
Conclusions
Individualized classical homeopathy may have been beneficial in managing AA associated with COVID-19 infection in this 9-year-old. The condition, though exhibiting signs of severe infection, resolved in 2 days avoiding the need for the otherwise recommended surgical excision. This is significant in the light of heavy health care burden during the COVID-19 pandemic. Further scientific studies, especially in hospital setups are needed to investigate the role of individualized classical homeopathy in treating similar severe acute infections.
Footnotes
Authors’ Contributions
M.M.: Conceptualized and resourced the patient data. E.E.S.: Resourced the patient data. S.M.: Resourced, worked on the original draft preparation, and co-administered the project. P.D. and A.B.: Curated the data and prepared the original draft. G.V.: Supervised and administered the project. All authors read and approved the final article.
Consent for Publication
Written informed consent was obtained from the patient’s legal guardian for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Availability of Data and Materials
All data generated or analyzed during this study are included in this article and its supplementary material files. Further enquiries can be directed to the corresponding author.
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
No funding was availed for this study.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.