
Abstract
Introduction:
During the luteal phase, women often experience various physical and mental symptoms related to irregularities in the autonomic nervous system. Aromatherapy has been reported to alleviate these symptoms and regulate autonomic nervous system function. However, many of them report transient responses in autonomic nervous system activity. We consider that diurnal fluctuations in the autonomic nervous system activity need to be modulated to improve symptoms and enhance quality of life. This study aimed to investigate the effects of aromatherapy on diurnal variations in the autonomic nervous system.
Methods:
Nineteen females (aged 20–22 years) without olfactory impairment were categorized into two groups as follows: those with severe symptoms (n = 10) and those with mild symptoms (n = 9) in the late luteal phase. Autonomic nervous activity was measured for 24 h, and symptoms were measured in the follicular and luteal phases. Similar measurements were made in the luteal phase after the participants performed the sniffing exercise for approximately 1 month using the essential oils most preferred by each participant.
Results:
Participants with severe symptoms in the late luteal phase preferred lemongrass and lavender vera, whereas those with milder symptoms in the late luteal phase preferred geranium bourbon. In the mild group, parasympathetic nervous activity at nighttime in the late luteal phase significantly decreased after the one-month sniffing exercise, correlating with significant symptom relief. No significant changes were observed in the severe group.
Discussion:
The results suggest that continued sniffing exercises can modulate diurnal variations in autonomic nervous activity, thereby expanding the potential application of aromatherapy.
Introduction
Women often experience physical and mental changes associated with hormonal fluctuations during their menstrual cycles. In the luteal phase, they may experience various physical and mental symptoms and, in some cases, be diagnosed with premenstrual syndrome (PMS), impacting their quality of life (QOL). Regulation of female hormone secretion involves the hypothalamus, which is also the center of the autonomic nervous system (ANS). Therefore, the ANS influences the physical and mental modulations associated with the menstrual cycle. 1 In managing PMS, low-dose pills are commonly prescribed. In addition, some individuals have adopted complementary and alternative therapies, such as yoga and aromatherapy. 2
Numerous studies have investigated the impact of essential oils. For instance, geranium essential oil has been reported to augment estrogen levels in menopausal women. 3 In addition, Matsumoto et al. found that lavender inhalation increased parasympathetic nervous activity. 4 However, they observed a transient response in ANS activity. We hypothesize that regulating diurnal variations in the ANS can improve subjective symptoms. Kouzuma et al. reported the efficacy of continuous acupuncture in regulating nighttime ANS activity and relieving menopausal symptoms. 5 However, we have not found any studies on aromatherapy examining the diurnal variation of the ANS. Yamakawa developed a simple and effective sniffing exercise that combines aromatherapy with deep breathing using a preferred essential oil. Some studies have reported that deep breathing can regulate the ANS.6,7 Although acupuncture requires the intervention of an acupuncturist, aromatherapy and breathing are easy self-care practices. In this study, we examined the effects of aromatherapy on diurnal variations in the ANS. Our findings will contribute to the established evidence supporting the benefits of aromatherapy and improve the social well-being of women.
Ethical considerations
This study was approved by the Ethics Committee of Kyushu University of Nursing and Social Welfare (Approval No. 02–029) and conducted in accordance with the Declaration of Helsinki.
Materials and Methods
Study sample
We recruited 31 young Japanese women; however, personal circumstances, sickness, and trouble with measurement prevented 12 individuals from providing data. Hence, 19 women aged 20–22, with menstrual cycles of 24–35 days and menstrual periods lasting 3–7 days, participated in this study. All participants reported normal olfactory function. The exclusion criteria included underlying conditions such as thyroid disease, diabetes mellitus, malignant neoplasms, manic depression, and taking hormonal medications, ANS-affecting drugs, or antidepressants within 2 months before study participation. All participants provided written informed consent.
Procedure
Each participant underwent two sessions as follows: the early follicular phase (3–5 days after menstruation ended) and the late luteal phase (3–5 days before menstruation began). In each phase, ANS activity for 24 h and symptom severity were measured. After the initial measurements were completed, ANS activity and symptoms were similarly measured in the late luteal phase after the sniffing exercise was performed for approximately a month. The sniffing exercise was performed twice a day, in the morning and evening, for 3 min, inhaling for 4 sec and exhaling for 8 sec while smelling their favorite essential oil. The essential oils used were from pine sylvestre (Pinus sylvestris), geranium bourbon (Pelargonium X asperum), lemongrass (Cymbopogon flexuosus), and lavender vera (Lavandula angustifolia) (supplied by Florihana Co., Ltd., Tokyo, Japan). Each participant inhaled the four essential oils in order, within a 90-sec interval, and chose their favorite oil during the luteal phase. The participants were blinded to the names and effects of the chosen essential oils until all the experiments were completed. However, before they participated in this study, it was explained to them that they could withdraw from the experiment if the smell of the essential oils made them feel nauseous.
The experiments were conducted between December 2021 and December 2023.
Heart rate variability analysis
The interval between the R and R’ waves was measured from lead II of the electrocardiogram using an Active Tracer AC-301A® (Arm Electronics Co., Ltd., Tokyo, Japan). For the heart rate variability (HRV) analysis, a fast Fourier transform was used to obtain the power spectrum (MemCalc/CHIRAM3 GMS Co., Ltd., Tokyo, Japan). The analyzed HRV spectrum spanned a frequency range of 0.04–0.4 Hz, with a low-frequency (LF) component at 0.04–0.15 Hz and a high-frequency (HF) component at 0.15–0.4 Hz. The HF component is an index of parasympathetic nervous activity, whereas the LF/HF power ratio measures sympathetic nervous activity.8–10 While measuring the ANS, each participant lived their usual life, being active during the daytime and sleeping at the nighttime, and described their daily activities such as diet, exercise, and sleep on a designated form.
Menstrual cycle symptoms
Physical and psychological symptoms accompanying the menstrual cycle were assessed using the Japanese version of the menstrual distress questionnaire (MDQ). 11 Developed by Kayashima et al., the MDQ features 47 items across eight domains as follows: moisture storage, concentration force, negative feelings, behavioral changes, pain, control, mood elevation, and autonomic dysregulation. Each item was scored from 0 (none) to 3 (severe). The MDQ scores were totaled for each domain during the early follicular and late luteal phases.
Menstrual cycle mental health
The participants’ mental health during the menstrual cycle was assessed using the strengths & difficulties questionnaire (SDQ). 12 Developed by Goodman, the SDQ features 25 items across five domains as follows: four domains on difficulties, emotional problems, conduct problems, hyperactivity/inattention, peer relationship problems, and one domain on strengths and prosocial behavior. Each item was scored from 0 (none) to 2 (applicable). The SDQ scores were totaled for each domain during the early follicular and late luteal phases.
Statistical analyses
The participants were divided into two groups as follows: those with an MDQ score exceeding 55 points (severe group [S group]) and those scoring less than 55 points (mild group [M group]) in the late luteal phase. ANS activity was also classified into daytime and nighttime based on each participant’s heart rate and behavioral record. However, the time slept for naps during the daytime and the time awakened to go to the toilet during the nighttime were excluded from the analysis. ANS activity may vary among individuals. Thus, the mean values for ANS activity in the late luteal phase before the sniffing exercise for 1 month were the baseline values and were standardized to 100%. The rate of change after the one-month sniffing exercise was compared within and among the groups using t-tests. MDQ scores were analyzed using Mann–Whitney U and signed-rank tests. All analyses were performed using Statistical Package for the Social Sciences version 25 (IBM, Armonk, NY, USA). Statistical significance was set at p < 0.05.
Results
Essential oil preferences and sniffing exercise implementation
Geranium bourbon was selected most frequently in the mild group (n = 9), whereas lemongrass and lavender vera were selected most frequently in the severe group (n = 10) (Table 1). The number of times the sniffing exercise was performed for 1 month in the mild group (728 ± 126 times) was slightly higher than in the severe group (678 ± 115 times), but there was no significant difference.
Types of Essential Oils Used in Sniffing Exercise (n = 19)
Assessment of symptoms and mental health
In the mild group, the total MDQ score after the sniffing exercise decreased significantly compared with that before the sniffing exercise (p = 0.038). In particular, “negative feeling” after the sniffing exercise decreased significantly compared with before (p = 0.028). In contrast, there was no significant difference in the total MDQ scores before and after the sniffing exercise in the severe group.
In the late luteal phase before the sniffing exercise, there were no differences between the two groups in scores for “behavioral change,” “mood elevation,” and “autonomic dysregulation” (p = 0.053, 0.113, and 0.065, respectively). However, after the sniffing exercise, the scores were significantly different between the two groups (p = 0.003, 0.001, and 0.008, respectively) (Table 2).
Comparison of Menstrual Distress Questionnaire during the Menstrual Cycle of Each Group
p < 0.05, **p < 0.01, Mann–Whitney U test.
p < 0.05, Wilcoxon signed-rank sum test.
In the follicular phase, there were no significant differences between the two groups in five domains of the SDQ. In the late luteal phase before the sniffing exercise, there were no significant differences between the two groups in four domains of difficulty, but the score for “prosocial behavior,” indicating the strength of the severe group, was significantly higher compared with the mild group (p = 0.013). In the luteal phase after the sniffing exercise, there were no significant differences between the two groups in all domains.
In the mild group, there were no significant differences before and after the sniffing exercise in all domains. In contrast, in the severe group, the score for “conduct problem” before the sniffing exercise was significantly higher than that after the sniffing exercise (p = 0.007) (Table 3).
Comparison of Responses to the Strengths & Difficulties Questionnaire during the Menstrual Cycle of Each Group
p < 0.05, Mann–Whitney U test
+p < 0.01, Wilcoxon signed-rank sum test.
Heart rate variability
In both groups, the participants’ heart rates were in a consistent range of 80–85 bpm during the daytime and 65 bpm during the nighttime, independent of the sniffing exercise and menstrual cycle.
HF values during the nighttime were higher than during the daytime in both groups, independent of the sniffing exercise and the menstrual cycle. In both groups, before the sniffing exercise, the nighttime HF values in the early follicular phase were higher than those in the late luteal phase; however, the difference was not significant. In the mild group, the nighttime HF value in the late luteal phase after the sniffing exercise was significantly higher than before (p = 0.031). Daytime HF values were similar in both groups, regardless of the sniffing exercise or menstrual cycle.
In both groups, the LF/HF ratio during the nighttime was lower than that during the daytime, independent of the sniffing exercise and menstrual cycle. In the severe group, the nighttime and daytime LF/HF ratios were similar, regardless of the sniffing exercise and menstrual cycle. In the mild group, the LF/HF ratios during the nighttime and daytime in the late luteal phase after the sniffing exercise were lower than those before the sniffing exercise; however, the difference was not significant. (Fig. 1, Table 4).
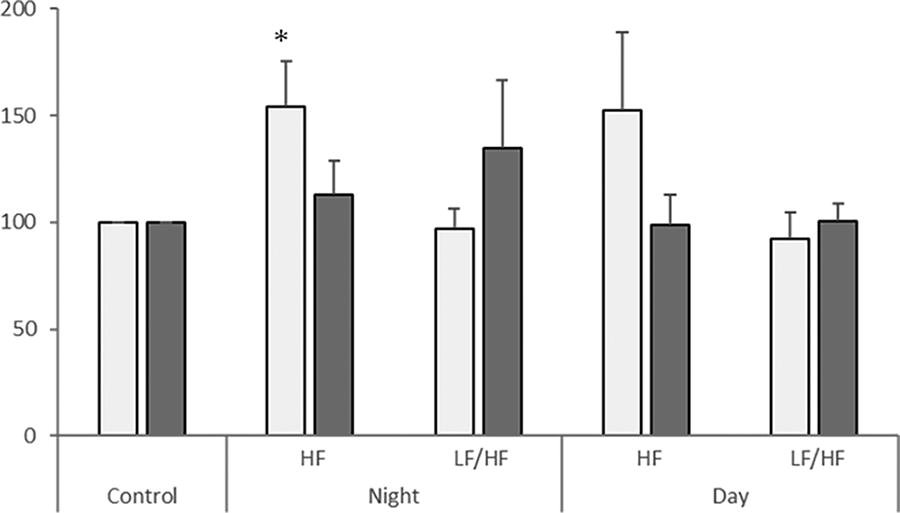
Changes in ANS activity after the sniffing exercise relative to before the sniffing exercise. Mean ± standard error (SE). Control: The mean values for ANS activity in the late luteal phase before the sniffing exercise for one month were the baseline values standardized to 100%. Night: The rate of change of ANS activity during the nighttime after the sniffing exercise for one month during the nighttime. Day: The rate of change of ANS activity during the nighttime after the sniffing exercise for one month during the daytime. HF, high frequency; LF/HF, low frequency/high frequency; white bar, mild group (n = 9); gray bar, severe group (n = 10). *Significant difference (p < 0.05) compared to the control (paired t-tests). ANS, autonomic nervous system.
Changes in Diurnal Variation of the Autonomic Nervous Activity Associated before and after Sniffing Exercise of Each Group
LF/HF, low frequency/high-frequency; SE, standard error; Comparison, Comparison of before and after sniffing exercise in the late luteal phase.
Discussion
In the present study, nighttime parasympathetic nervous activity increased after the one-month sniffing exercise compared with that before the exercise, and symptoms were relieved in the mild group. This suggests that the sniffing exercise, using each participant’s favorite essential oil for a month, regulated ANS activity and relieved symptoms. Hayano et al. demonstrated that parasympathetic activity during sleep was lower in older individuals than in younger ones, implying a greater reliance on sympathetic activity due to decreased parasympathetic activity in older age, particularly when activity was less pronounced. 13 Increased parasympathetic activity during nighttime is likely to increase dependence on parasympathetic nervous activity during the day, reducing the likelihood of excessive sympathetic activity. Higher levels of parasympathetic activity at rest have been associated with a reduced risk of sudden cardiac death. 14 Therefore, maintaining high levels of parasympathetic nervous activity at rest is thought to inhibit the activation of respiration and circulation by various stimuli to the body, thereby regulating bodily functions. This study observed no changes in sympathetic activity during the daytime before and after the sniffing exercise. The degree of sympathetic nervous activity during the day may have been influenced by the participants’ daily activities. In this study, the amount of daily activity was not measured. Normally, the heart rate increases depending on the amount of activity. However, the heart rates during daytime and nighttime were similar regardless of the sniffing exercise or menstrual cycle in both groups. This suggests that the amount of daily activity during the measurement was also similar regardless of the sniffing exercise or menstrual cycle. In addition, the degree of stress affects ANS activity. In the SDQ, one domain in the severe group increased after the sniffing exercise, but the total difficulty scores in the two groups were the same regardless of sniffing exercise or menstrual cycle, so stress in daily life may not have affected the present results. Higher levels of physical activity have been reported to improve sleep quality and reduce levels of anxiety and depression. 15 Low-intensity physical activity has been reported to mitigate the adverse effects of sleep deprivation. 16 These suggest that there is an association between the amount of physical activity and sleep. Activity level may influence sympathetic activity during the daytime, whereas sleep quality may be related to parasympathetic activity during the nighttime. Therefore, future studies should include a detailed analysis of each participant’s activity levels.
In the present study, some symptoms, such as “negative feeling,” and the total MDQ score decreased after the sniffing exercise in the mild group. The occurrence of physical and psychological symptoms during the luteal phase is associated with progesterone. In addition, all the participants in this study had higher total MDQ scores during the luteal phase than during the follicular phase. It has been reported that severe physical and mental symptoms in the luteal phase are associated with high sympathetic and low parasympathetic activities, 17 suggesting a link between these symptoms and ANS function. In the mild group, increased parasympathetic nervous activity in the night and symptom relief were observed after the one-month sniffing exercise. This may be attributed to the continued practice of deep and slow breathing exercises using one’s favorite essential oils. Vierra et al. reported that 4-7-8 breathing exercises increase parasympathetic nervous activity. 6 This study demonstrated similar results, although with a slightly different breathing pattern. We adopted the 1:2 exhalation to inhalation breathing pattern, which may influence the regulation of ANS function.
However, significant changes were not observed in the severe disease group. We found that parasympathetic nervous activity during the nighttime was altered in the mild group but not in the severe group. In the method used in this study, essential oils were taken in through inhalation. Therefore, the amount and duration of exposure of the participants to the essential oils were minimal. In addition to inhalation, application and ingestion are other ways to apply essential oils, and these methods may have a greater effect than inhalation. Although the present study cannot explain the specific mechanism of the impact of essential oils on ANS activity, it may be necessary to increase the amount and duration of exposure to essential oils in the severe group.
The differences in ANS activity in the two groups may have been influenced by each participant’s choice of essential oil. Most participants in the mild group chose geranium bourbon, whereas those in the severe group mostly selected lemongrass or lavender vera. While lemongrass essential oil has been reported to have anti-inflammatory properties, 18 there are no reports on its effects on ANS activity. Further investigation into the effects of lemongrass on ANS activity is necessary. Lavender essential oil is known for its relaxing properties. 4 Participants in the severe group had more symptoms of “concentration force,” “negative feelings,” and “pain” in the late luteal phase, which may have prompted their selection of lavender to alleviate these symptoms. While lavender essential oil has been shown to increase parasympathetic nervous system activity, 4 the present results differ. Although most participants in the severe group used lavender vera, no change in ANS activity or relief of symptoms was observed. This may stem from differences in the methods used to assess transient responses and diurnal variations in ANS activity. Lin et al. found that while inhalation of sandalwood and lavender increased parasympathetic activity at low-stress levels, it had no effect on ANS at high-stress levels. 19 This study yielded similar results. The biological irritation caused by inhaling essential oils is slight; therefore, the effects may be more pronounced in cases of mild symptoms or low stress. In the mild group, parasympathetic nervous activity increased, and symptoms were alleviated after the one-month sniffing exercise. Continued use of the preferred essential oil in sniffing exercises may prevent symptom exacerbation at mild levels. However, these results were comparisons before and after the one-month sniffing exercise and not with a control group. In a study involving sensory intervention, such as a sniffing exercise using a favorite essential oil, comparative verification with a control group would be necessary.
Diversified complementary and alternative therapies, including acupuncture, moxibustion, yoga, supplementation, aromatherapy, and breathing techniques, can enhance quality of life by considering individual symptoms, lifestyle, and preferences.
Limitations
First, this study was limited to a small sample size of 19 young women and did not involve a randomized comparative study with a placebo control group. Therefore, our findings provide only one possible explanation for the effect of aromatherapy on the ANS, and a comparison with a control group is necessary. Second, our results identified preferences for four types of essential oils. A more detailed examination of individual preferences for different essential oils would be needed. Finally, ANS activity should be evaluated, including the level of activity in daily life.
Conclusions
In young women, performing a sniffing exercise for one month increased parasympathetic nervous activity during the night and provided symptom relief in the late luteal phase.
Footnotes
Acknowledgments
Authors’ Contributions
N.K.: Conceptualization, data curation, formal analysis, and writing—original draft. T.Y.: Conceptualization, data curation, and writing—review & editing.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available because of privacy restrictions, as the databases contain information that could compromise the privacy of the research participants. Deidentified datasets are available from the corresponding author upon reasonable request.
Author Disclosure Statement
The authors declare that they have no conflicts of interest.
Funding Information
This study was supported by