
Abstract
Objective:
There is a need to address the mental health insufficiencies among the home-quarantined COVID-19 patients. Telemedicine is reckoned as a productive means to stay connected with patients during pandemic. This study explores the role of Yoga and Naturopathy Interventions (YNI) as the telemedicine in improving depression, anxiety, stress, quality of life (QoL), and symptom scores among home-quarantined COVID-19 patients.
Methods:
This was a nonrandomized controlled study that included 112 COVID-19 patients who received either YNI (n = 56), which includes yoga therapy, naturopathic diet, steam inhalation, self-acupressure delivered across the day or simple sectional breathing (n = 56) through a telemedicine mode for 14 days, along with standard care. The allocation of the study participants to either YNI or Breathing was done by two of the investigators. At baseline and on the 14th day, the Depression Anxiety Stress Scale (DASS-21), World Health Organization (WHO) QoL, and Symptom scores were measured.
Results:
A generalized linear model was used to evaluate the effects of intervention on stress, anxiety, depression, and WHO-QOL scores. The YNI group had shown significant improvement in DASS-21 scores and the QoL domains as compared with the controls. The severity of cough was significantly reduced in the study group compared with the controls. However, the changes in the severity of other symptoms such as breathlessness, persistent pain, pressure in the chest, fever, headache, and loss of smell remained insignificant between the groups.
Conclusion:
YNI-based telemedicine was found effective in reducing depression, anxiety, and stress and improving the QoL in COVID-19 patients. However, limitations such as a small sample size and a lack of randomization warrant large-scale studies to strengthen these findings.
Trial Registration:
Clinical Trial Registry Number: CTRI/2021/05/033816.
Introduction
COVID-19 has posed a huge challenge to the health care delivery system across the globe, leading to various unprecedented changes in our lifestyle and health seeking approaches. Unlike the first wave of COVID-19, the second wave presented a surge in the number of cases that altered the management strategies for COVID-19. The World Health Organization (WHO) recommended home isolation for both adults and children (both confirmed and suspected cases) in the event of a deficit in supply of health care services as compared with demands. 1
According to reports, these home-confined patients require additional safe and effective monitoring. 2 Adding to this, a surge in anxiety, depression, and stress related to COVID-19, and its subsequent impact on quality of life (QoL) also warrants attention.3,4 Telemedicine has been identified as a potentially effective method of reaching out to patients during natural disasters and pandemics. 5 Furthermore, telehealth services have been reported to be suitable for addressing the mental health concerns of patients and their families in the comfort of their homes.6,7
Most of the studies on the utilization of telemedicine are restricted to the clinical monitoring and management of the COVID-19. 8 However, the mental health component of COVID-19 has not been addressed in these studies. Yoga and naturopathy as a combined intervention have been reported to reduce the mental health deficiencies associated with COVID-19, 9 and are regarded as useful as an adjunct therapy in the management of COVID-19. 10
However, no reports are available in terms of the utility of yoga and naturopathy in telemedicine mode. This seems vital in the midst of the disruptions inflicted by COVID-19 on the mental health and subjective well-being of home-quarantined patients. Furthermore, reports suggest positive effects of including yoga and naturopathy techniques such as meditation, postures (asanas), breathing practices (pranayamas), fasting, steam inhalation, diet therapy, hydrotherapy, and sun bath in the management of COVID-19.9–13 This study explores the impact of yoga and naturopathy interventions (YNI) delivered in telemedicine mode among mild to moderate home-quarantined COVID-19 patients.
Methods
Study design
The study was an open label nonrandomized parallel group study conducted at two housing societies in the same city in India. Apart from the convenience of executing the study, no other specific criteria were followed to choose these sites, as both investigators resided at the two respective locations. One housing society served as the interventional arm and the other as the control. The study was approved by the Institutional Ethics Committee (F. No. 12/SHMCNYS-IEC/Pl 7/2020-2021) and is registered under the clinical trial registry of India (CTRI/2021/05/033816).
Study participants
The participants were COVID-19 positive residents of the aforementioned housing societies, diagnosed through an reverse transcription polymerase chain reaction (RT-PCR) test, and classified as mild to moderate COVID-19 cases as per the criteria of the Indian Council of Medical Research (ICMR). They were advised to stay home in quarantine until their RT-PCR test results turned negative, or for 14 days, by the respective state health authorities. The participants were invited to participate in the study through digital flyers circulated through WhatsApp groups.
As randomization was not possible due to COVID-19-related restrictions, the allocation of the study participants to the intervention arm or the control arm was done by the two investigators who were residing at the same housing society chosen for the study. All the participants signed a digital informed consent for participating in this study. All the mild and moderate COVID-19 positive cases under hospital care, patients who required supplementary oxygen therapy, and COVID-19 positive pregnant and lactating mothers were excluded from the study.
The study participants were contacted through telehealth, that is, interactive audio–video software (www.zoom.us). The licensed and “A”-class registered medical practitioners with a 5.5 year full-time medical degree (Bachelors of Naturopathy and Yoga) and >8 years of professional experience provided the interventions. These medical practitioners are authorized to provide yoga and naturopathy therapies for COVID-19 as per the protocols released by the Central Council for Research in Yoga and Naturopathy, Ministry of AYUSH, Government of India. 14 The intervention group received a daily protocol of Hatha Yoga therapy, Naturopathy diet, steam inhalation, and self-acupressure for 14 days along with the standard protocol recommended by the ICMR, which included symptomatic management of fever using Tab.
Paracetamol 650 mg four times a day, Tab. Ivermectin 200 mcg/kg once a day, for 3–5 days, and inhalational Budesonide 800 mcg twice daily for 5–7 days for a persistent cough. 15 In contrast, the control group, in addition to the ICMR protocol, received daily practice of sectional breathing (Vibhagiya Pranayama) for 15 min. It is a combination of abdominal breathing (10 rounds), upper lobar breathing (10 rounds), and full yogic breathing (4 breaths/min). 16 The detailed intervention plan is tabulated in Table 1 and the study flow diagram as per the consolidated standards of reporting trials is depicted in Figure 1.
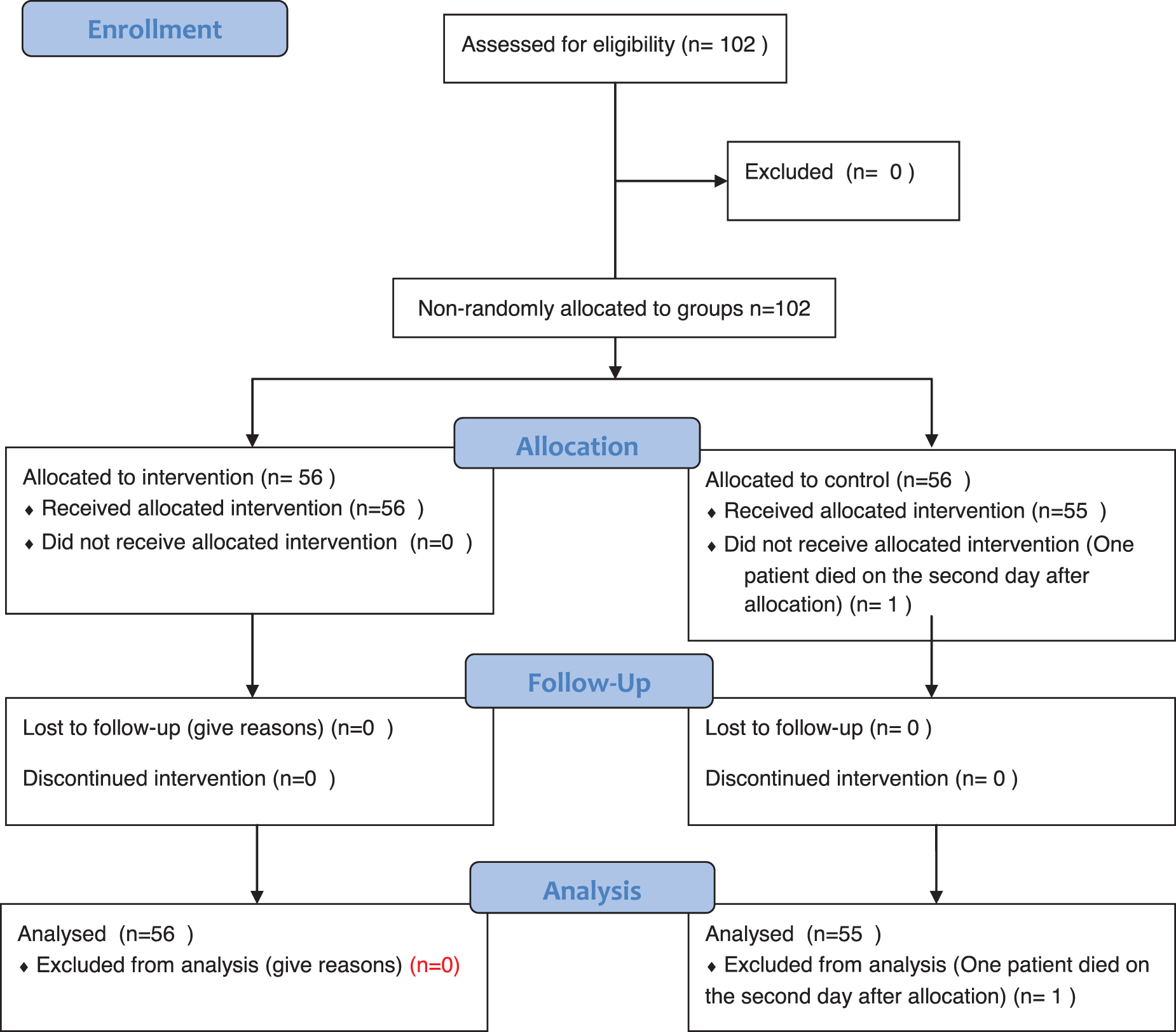
Study flow diagram.
Summary of Yoga and Naturopathy Interventions Advised Through Telemedicine
Outcome measures
The primary outcome compared the effects of YNI advised through digital mode on the depression, anxiety, and stress scores measured through the depression, anxiety, stress score questionnaire (DASS-21). The secondary outcomes analyzed the impact of the YNI on improving the QoL measured through WHO QoL questionnaire brief version 17 and symptoms of COVID-19 such as cough, breathlessness, persistent pain, pressure in the chest, fever, headache, loss of smell, and any other symptoms through a Likert scale (1-no symptom, 2-mild, 3-moderate, 4-severe, and 5-extremely severe). Both DASS-21 and WHO QoL scores were measured at the baseline and at the end of the 14th day, whereas changes in symptom scores were measured on days 1, 7, and 14.
Statistical analysis
The data were coded and entered in Microsoft Excel 2010. The normality of the distribution for continuous variables (i.e., stress, anxiety, depression, and WHO-QoL scores) was assessed using the Kolmogorov–Smirnov test. Considering the non-normal distribution and baseline differences between the intervention and control groups, a generalized linear model was used to evaluate the effect of the intervention on the stress, anxiety, depression, and WHO-QoL scores captured as continuous variables.
These generalized linear models have been used in previously conducted randomized controlled trials to compare the differences among psychological domains. 18 The intervention status was a covariate, and the model that accounted for the main effects of the intervention, the interaction effect of the intervention and baseline differences was offset for the baseline scores of the respective dependent variables. The effect estimates for the outcome scores in the intervention group with reference to the control group were reported as adjusted mean differences (β coefficients).
The chi-square test was used to find out the difference in frequency of the parameters of symptom scores. In the absence of prior randomization due to operational reasons (travel restrictions, adherence, and trust issues), propensity score matching (PSM) was used to eliminate the effects of confounding factors while estimating the treatment impact. The propensity score refers to “the probability of treatment assignment conditional on observed baseline characteristics.” 19
PSS allows nonrandomized trials to estimate a casual effect similar to that of the randomized control trial by eliminating confounding effects while assessing the impact of the intervention on the outcomes. 19 The grouped variables based on the medication and yoga were matched by age, sex, and symptoms such as cough and breathlessness, using PSS. Nearest Neighbor Matching Method was used for PSS. In this method, one observed propensity score from the control is matched twice with the observations made from the propensity score in the study arm, that is, patients were matched (Control:Study) at a ratio of 1:2 using the nearest neighbor technique, without replacement.
Furthermore, a caliper of 0.15 standard deviations (SDs) was enforced, where n was determined by the relative sizes of the matched comparison groups. This method is adapted basically to reduce the estimation bias between the intervention and the control group. This study used incomplete matching to include the maximum of samples in the analysis.
Statistical software R version 4.1.2 was used for performing PSS. SPSS 22.0 (IBM Analytics, New York, NY) was used for the analysis of the treatment effects. The significance level was set at 0.05.
Results
The study included 56 patients (males = 27, females = 29) with an average age of 39.98 (SD 16.67) years in the interventional group, and 56 patients (males = 30, females = 26) with an average age of 39.62 (SD 9.01) years in the control group. Because of the death of one patient shortly after enrollment, the final analysis included 56 interventional group participants and 55 control group participants.
Comparison of DASS-21 scores
The findings indicate that the intervention resulted in a significant reduction in stress, anxiety, and depression scores in the study group as compared with the control group. The greatest decrease was observed in depression scores, with an adjusted mean difference of −21.75 for depression scores postintervention in the study group compared with the control group (Table 2).
Comparison of Depression, Anxiety, Stress, and Quality of Life Scores Between the Groups
The β coefficients are the adjusted mean differences estimated for the intervention group in comparison with the control group after offsetting for the baseline differences.
QoL, quality of life; SD, standard deviation; WHO, World Health Organization.
WHO health-related QoL comparison
The postintervention scores across the four dimensions of WHO QoL (i.e., physical health, psychological health, social relationships, and environmental health domain) reported a significant improvement in the intervention group compared with the control group after offsetting for the baseline differences between the groups. There was a significant positive improvement in the postintervention scores of WHO QoL with the adjusted mean difference ranging from 46.26 to 74.46 for the intervention group compared with the control group (Table 2).
Comparison of symptom scores
The scores for the symptom, based on the Likert scale for the severity, were measured in both the interventional group and the control group.
Interventional group scores
There were no patients in the interventional group who had a cough, pain, or pressure in the chest at baseline, and this remained constant at the end of the 7th day. There was a significant difference in the symptoms of breathlessness among the participants. All cases showed absolutely no symptoms of breathlessness postintervention on day 7 (χ 2 = 24.3, df = 4, p = 0.00001). Similarly, there was a significant difference in the severity of fever among the participants. No symptoms of fever were present postintervention on day 7 (χ 2 = 104.3, df = 4, p = 0.000).
The severity of headache among the interventional group also significantly decreased by the end of the 7th day as compared with baseline (χ 2 = 34.57, df = 4, p = 0.000). Similar results were observed in the loss of taste and/or sensation among the interventional cohort. None of the participants had a loss of taste and/or smell at the end of 7 days (χ 2 = 20.99, df = 4, p = 0.000). There was complete remission of other reported symptoms such as weakness. However, this difference was not found to be statistically significant (χ 2 = 2.12, df = 4, p = 0.710).
Control group scores
The control group did not have symptoms such as breathlessness, persistent pain, pressure in the chest, or loss of taste/smell sensation. When compared with baseline, the number of participants with mild and moderate cough increased significantly on day 7 (χ 2 = 35.8, df = 4, p < 0.001). The control group had also shown a significant reduction in the severity of fever (χ 2 = 82.04, df = 4, p < 0.001) and headache (χ 2 = 55.75, df = 4, p < 0.001) on day 7.
On comparing the day 7 scores between the interventional and control groups, barring the symptom of cough (χ 2 = 79.98, df = 4, p < 0.001) none of the other symptom scores showed a statistically significant difference. The detailed symptom scores are tabulated in Supplementary Data.
Discussion
With the growing number of COVID-19 cases in India during the second wave, only critical patients were admitted to the hospitals, whereas patients who were asymptomatic or had mild symptoms were advised to undergo home quarantine. Reports suggest beneficial effect of telemedicine-based monitoring among COVID-19 patients who were under home quarantine. 8 Furthermore, COVID-19 has induced a detrimental impact on mental health indices and the well-being of both infected and noninfected individuals. 20
An earlier report suggests the efficacy of YNI in improving anxiety and depression in COVID-19 patients who are admitted to the hospital. 9 Furthermore, yoga has been reported to reduce anxiety, stress, and fear while improving coping capabilities during COVID-19. 21 This study indicates similar prognostic effects on stress, anxiety, and depression through telemedicine-based home delivery of YNI. These findings should be viewed as a first step toward developing a telehealth-based module for a larger population of people who have restricted social behavior due to COVID-19.
Similarly, QoL has emerged as one of the major indices to assess well-being during COVID-19, where QoL is found to be compromised.22,23 This study has shown significant improvement in all QoL domains in the intervention group as compared with the control group. This improvement in QoL is encouraging and necessitates the need to establish a support system that can complement the standard of care.
Both the intervention and control groups have shown a significant reduction in symptoms on day 7, whereas the number of cough cases has considerably increased in the control group. This demonstrates the effectiveness of guided yoga and naturopathic interventions in alleviating COVID-19 symptoms, particularly cough. However, no statistically significant difference was observed between the cases and the controls, which may be due to the difference in severity of symptoms between the groups or the small sample size.
This is the first study to look at the role of yoga and naturopathic interventions as adjuvant therapies for improving mental health and QoL, as well as relieving symptoms, in mild and moderate COVID-19 patients who are quarantined at home. However, there is abundant room for further progress in this arena, where the goal should be to generalize and validate the findings. The limitations of this study, such as the smaller sample size and nonrandomization due to operational restrictions owing to COVID-19, need to be considered while reckoning the results. Future studies should consider using a randomized controlled design with a larger sample size and more precise inclusion criteria to overcome the limitations of this study.
Despite these limitations, the reduction in anxiety, stress, and depression along with the predominant improvement in QoL signifies the need for devising telemedicine-based YNI among home-quarantined patients. This fact has been supported by the patients who underwent YNI at the hospital and who opined that the presence of a yoga and naturopathy physician and their treatments made a significant difference in their psychological well-being and morale. 13
Conclusion
This study's findings suggest that yoga and naturopathy-based lifestyle interventions delivered through telehealth have a positive impact on the mental health and QoL of mild and moderate COVID-19 patients. However, robust randomized trials with adequate sample sizes are warranted to ensure generalization.
Footnotes
Acknowledgments
We thank Dr. Prakash Babu Kodali, PhD, assistant professor, department of public health and community medicine, Central University of Kerala, for his guidance and support in data analysis. We also thank Prof. (Dr.) Jyoti Keswani, head, department of yoga, for her support in reviewing the article. We would like to acknowledge the support of all study participants and Ms. Roshan H. Hirani, former director, Agakhan Health Services India.
Authors' Contributions
Each author contributed to this research and article preparation, and approved the final version of the article. P.M.K.N. drafted the article and substantially contributed to data collection. N.J., K.D.B., V.R., G.R.T., and H.S. also substantially contributed to data gathering and project designing. P.M.K.N., N.J., K.D.B., V.R., G.R.T., and H.S. substantially contributed to conception and design, and critically revised the draft article for important intellectual content. Conceptualization, methodology, data curation, and writing—reviewing and editing by P.M.K.N. Conceptualization, visualization, and investigation by N.J. Data curation and validation by K.D.B. Data curation and investigation by V.R. Methodology and conceptualization by G.R.T. Methodology, conceptualization, and execution by H.S.
Data Availability
The data will be provided on reasonable request through mail from the corresponding author.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.