
Abstract
Introduction:
Pain or vaso-occlusive crisis is the hallmark of sickle cell disease (SCD). Standard treatment for SCD pain includes hydration, as well as nonsteroidal anti-inflammatory drugs and opioid pain medications. Although most studies show that opioids provide short-term relief, they are associated with side effects including constipation, opioid-induced hyperalgesia, and risk of dependence and addiction. The objectives of this study were to assess the prevalence of complementary and integrative medicine (CIM) use in a population of pediatric patients with SCD, the type of CIM used, and sociodemographic and health-related factors associated with their use of CIM.
Methods:
Parents of children with SCD were recruited to the study during clinic visits and hospitalizations. They were asked to complete a 22-item self-administered survey about their child's use of CIM. Descriptive statistics were used to generate frequencies or percentages for categorical variables. Chi square or Fisher's exact test was performed with a p-value <0.05 to test the association between CIM and sociodemographic characteristics in the collected sample.
Results:
Of the 99 parents who completed the survey, 86% reported using CIM. The most commonly used techniques were prayer (68%), massage (53%), heat (30%), relaxation techniques (24%), aroma therapy (23%), exercise (21%), and herbal medicine (16%). Nineteen percent of foreign born and 15% of U.S. born parents reported using herbal and folk remedies. Twelve parents reported using spiritual healing, reiki, or laying on of hands, and eight parents reported using acupuncture and mindfulness. Nine percent of parents reported using cannabidiol products and 4% of parents reported using cannabis for their child's SCD. Fifty-five percent of parents reported that CIM was helpful.
Conclusions:
Health care providers should be prepared to integrate CIM into their discussions with patients and families and provide more opportunities for families to learn about safe CIM approaches.
Introduction
Over the past 20 years, complementary and integrative medicine (CIM) use has increased in popularity in the United States. Complementary and integrative medicine, formerly known as complementary and alternative medicine, brings nonmainstream approaches and conventional medicine together in a coordinate way to promote the health and wellness of patients.1,2 It includes the use of nutrition, manual therapy, traditional Chinese medicine, and mind–body strategies. 3
Studies indicate that people who use CIM are more likely to be White, female, educated, married, and had higher income. 1 They are also more likely to have a chronic medical condition and their children are more likely to use CIM. 1 Examples of CIM include acupuncture, homeopathy, herbal remedies, yoga, Tai Chi, meditation, spiritual healing, and reiki.3,4
Sickle cell disease (SCD) is an inherited disorder of the blood that affects ∼100,000 people in the United States. 5 Pain or vaso-occlusive crisis (VOC) is the hallmark of SCD and is the most common cause for hospitalization.6,7 Standard treatment for VOC includes hydration, as well as nonsteroidal anti-inflammatory drugs and opioid pain medications.8,9 Although most studies show that opioids provide short-term relief, they are associated with side effects including constipation, opioid-induced hyperalgesia, and risk of addiction. 10
Numerous researchers have examined CIM in adults with SCD. Studies show that 92% of adults with SCD use CIM because of its multimodality treatment approach, limited side effects, and low cost. 7 The most common techniques used by these patients include prayer, relaxation techniques, and spiritual healing. 11 However, few studies have examined CIM in children with SCD. 12
The objectives of this study were to determine the prevalence of CIM in a population of pediatric patients with SCD, the type of approaches used, and sociodemographic and health-related factors associated with the use of CIM. It was hypothesized that the use of CIM would be common in children with SCD given the chronic nature of the disease and would be associated with parent gender, parent education, household income, and pain burden as measured by emergency department visits and hospitalizations.
Methods
Parents of children with SCD of all genotypes were recruited for the study during hematology clinic visits and hospitalizations. If they had a child between the ages of 0–22 years, they were given an information sheet that provided them with information about the study as well as a 22-item self-administered survey (Supplementary Data) about their use of CIM, the type of approaches used, and their child's pain experience. Parents were excluded if they had already completed the survey. The study was completely voluntary and participants were not compensated for their time.
The survey consisted of three parts. The first part included questions about the parent's age, gender, ethnicity, country of origin, marital and employment status, education level, and household income. It also included questions about the child's age, gender, and sickle cell genotype. The second part of the survey included questions about the child's pain experience as measured by the number of missed days from school (0 to >30 days) the previous school year, the frequency of SCD pain crises (a great deal to none at all) in the past year, the number of emergency room visits for SCD pain (0 to >5), and the number of hospitalizations for SCD pain (0 to >10) in the past year. The last part of the survey included questions about their use of CIM. The survey took ∼10 min to complete.
The study was conducted at Children's National Hospital which provides care to 1200 patients with SCD. A total of 109 parents were approached about the study and 10 parents declined to participate due to time constraints. The response rate was 91.7%. Most parents (95%) completed the survey during clinic visits. The study was conducted over a 6-month period (September 2020 to March 2021). Descriptive statistics were used to generate frequencies or percentages for categorical variables. Chi square or Fisher's exact test was performed with a p-value <0.05 to test the association between CIM and sociodemographic and health-related factors in the collected sample. All study procedures were approved by the institutional review board at Children's National Hospital.
Results
A convenience sample of 99 parents completed the survey about CIM. A majority of parents (85%) were female and 98% were Black or African American. The mean age of parents was 41.1 years (standard deviation [SD] = 9.1) and the mean age of children with SCD was 11.3 years (SD = 5.4). Nearly all children had hemoglobin SS (Hb SS) disease (72%) which is the most common form of SCD. Demographic characteristics are presented in Table 1.
Demographic Characteristics
DK, do not know; Hb SS, hemoglobin SS; Hb SC, hemoglobin SC; Hb S beta +, hemoglobin S beta plus thalassemia; Hb S beta 0, hemoglobin S beta zero thalassemia; SD, standard deviation.
Eighty-six percent reported using CIM for their child's SCD. The most commonly used techniques were prayer (68%), massage therapy (53%), heat (30%), relaxation techniques (24%), and aroma therapy (23%). Nineteen percent of foreign born and 15% of U.S. born parents reported using herbal and folk remedies. Twelve percent of parents reported using spiritual healing, reiki, or laying on of hands, and 8% reported using acupuncture and mindfulness. Nine percent of parents reported using cannabidiol products and 4% of parents reported using cannabis (see Fig. 1). CIM use was not associated with sociodemographic characteristics and health-related factors and pain burden was not associated with the use of CIM (see Table 2).
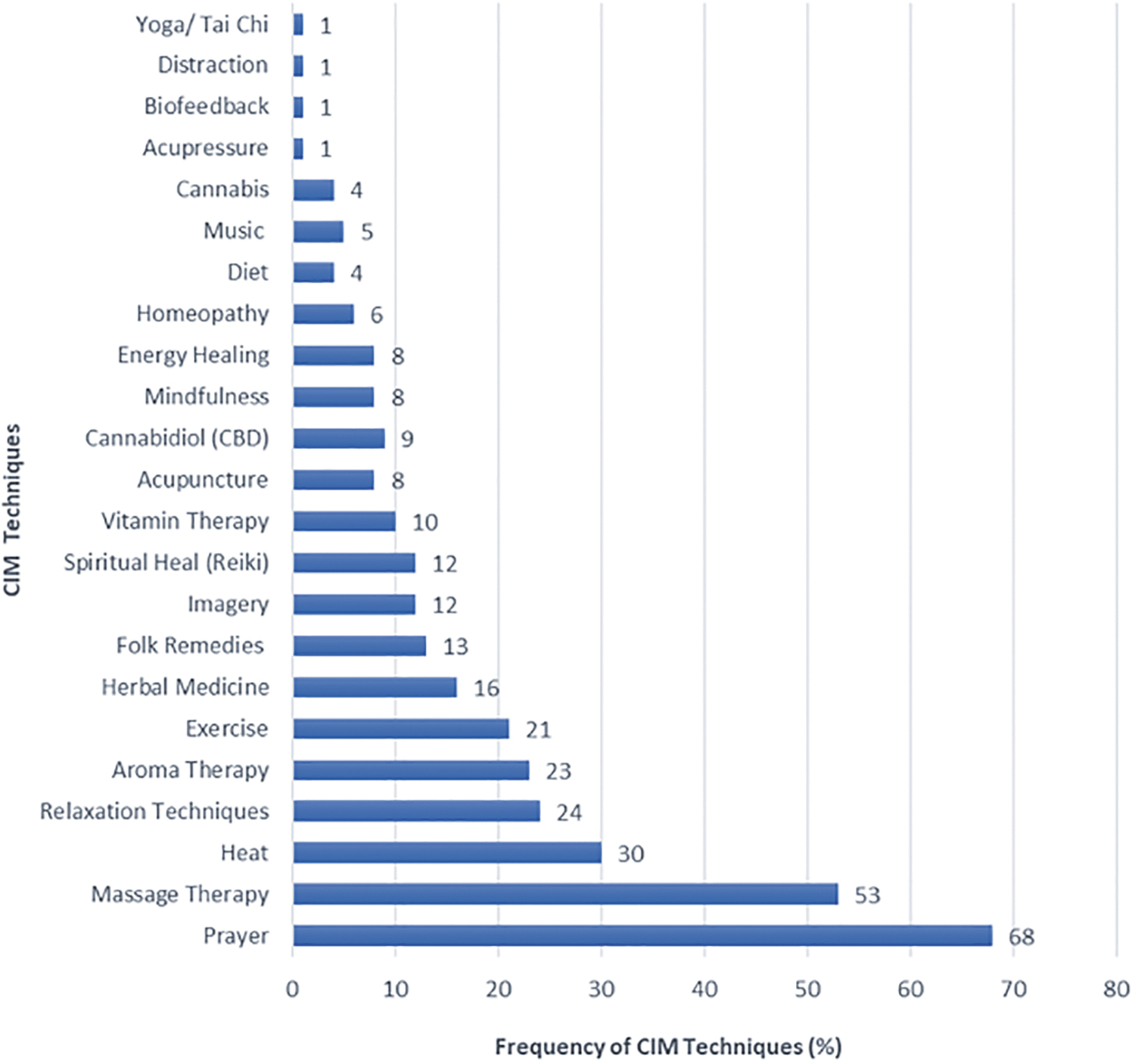
The frequency of each CIM technique. Sixty-eight percent of parents reported using prayer for their child's SCD. Fifty-three percent of parents reported using massage and 30% reported using heat. Only 1% of parents reported using yoga/Tai Chi, biofeedback, and acupressure. Most participants reported using more than one technique. CIM, complementary and integrative medicine; SCD, sickle cell disease.
Complementary and Integrative Medicine Use by Sociodemographic and Health-Related Factors
SCD, sickle cell disease.
Fifty-five percent of parents reported that CIM was helpful. Of the parents who responded to the disclosure question, 75% had discussed their use of CIM with their child's hematology provider. Every parent (N = 99) indicated that more opportunities should be provided for families to learn about safe CIM approaches. Seventy-three percent reported that they did not know whether their health insurance covered some evidence-based CIM approaches such as acupuncture and massage therapy.
Discussion
In this study, 85% of parents reported using some form of CIM for their child's SCD. Other studies have reported the use of CIM in children with SCD to be <70%. 13 However, many of those studies were conducted in the late 1990s and CIM use has increased exponentially since then. The most common CIM techniques used were massage therapy, heat, aroma therapy, and relaxation techniques. More than half of parents (80%) reported using prayer, which is consistent with other studies that have documented the high use of prayer by Black or African American parents of children with SCD.11,12
In addition, most parents relied on minimal risk techniques for their child's SCD, which is also consistent with other studies that have shown that these parents are more likely to use mind–body approaches than other forms of CIM. 7 And lastly, sociodemographic and health-related factors and country of origin were not associated with the use of CIM, which may reflect the growing popularity of CIM in the United States.
Few studies have examined cannabis and cannabinoids in youth with SCD. Of the parents who completed the survey, 9% reported using cannabidiol products and 4% reported using cannabis to treat their child's SCD. These results are different from a recent study reporting that cannabis use is prevalent in adolescents with SCD. 14 The infrequent use of cannabis and cannabinoid products in this study may stem from the negative connotations associated with these products, including their psychoactive effects.
In addition, patients who participated in this study were younger (mean age was 11.3 years) than those who participated in previous studies,14,15 which may also explain the infrequent use of cannabis in this population. Furthermore, parents are often unaware of their child's use of cannabis, which may have led to the under-reporting of cannabis use. And lastly, parents may have feared repercussions if they admitted to cannabis use for their child's SCD.
Of those who responded, 55.8% reported that CIM helped a lot and 36% reported that it helped some. These findings are consistent with other studies that have examined the use of CIM in children with SCD. Most parents (75%) reported that they had discussed their use of CIM with their child's hematology providers, which is different from other studies that have reported that most parents do not discuss their use of CIM. 4 In this study, most parents reported that they were eager to discuss their use of CIM with their child's provider. Every parent reported that more opportunities for families to learn about CIM should be provided and most parents reported that they did not know whether their health insurance covered some evidence-based CIM approaches.
There are several limitations to this study. First, this study was a cross-sectional study with a small sample size that was conducted at a single site. Second, only English-speaking parents were recruited for the study, which may limit the generalizability of these findings. Third, the measurements used in this study focused exclusively on parent-only report of the use of CIM instead of both parent and child report. In addition, parents may have interpreted some of the survey questions differently than was intended and wording of questions may have introduced bias. And lastly, parents may have provided socially desirable responses to the survey questions about cannabis.
Conclusions
Despite these limitations, important clinical conclusions can be drawn from the study. Parents often use CIM for their child's SCD. The most commonly used modalities in this study were prayer, massage therapy, heat, and relaxation techniques. Most parents reported that CIM was helpful. As a result, health care providers should be prepared to integrate CIM into their discussions with patients and families and provide more opportunities for families to learn about safe CIM approaches. Providers should also encourage parents to speak with their insurance representative to learn whether some CIM approaches such as massage therapy and acupuncture are covered by their plan.
Footnotes
Authors' Contributions
L.T. contributed to conceptualization, methodology/design, data collection, supervision, interpretation of results, and writing—original draft. S.M. was involved in interpretation of results and writing—reviewing and editing. A.Z. carried out data analysis and interpretation of results. D.S.D. contributed to conceptualization, methodology, interpretation of results, and writing—reviewing and editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.