
Abstract
Objective:
The objective of this study was to quantitatively determine intervertebral motions and changes in the intervertebral foramen (IVF) area, height, and width in the lumbar spine during the application of a chiropractic procedure.
Methods:
Eight unembalmed cadavers (five male and three female, age range 43–87 years) were procured for these experiments. Infrared light emitting markers were attached to L4, L5, and sacrum using metal rods to track the three-dimensional motion using the OPTOTRAK system. Five 4-sec cycles of flexion–distraction were performed over a 20-sec period by three clinicians. Vertebral movement data were collected using the marker data in three dimensions and the IVF by digitizing the IVF and computing the changes in area, height, and width. Vertebral motions were computed using three-dimensional kinematics in flexion, lateral bending, twisting, axial traction, and by digitizing the IVF contours; the dimensional changes in terms of height, length, and width were computed.
Results:
The flexion–distraction procedure created vertebral motions. Mean and standard deviation (SD) values of movements at L4–L5 were (1) 4.2° (0.78) in flexion and mean and SD values of vertebral separations were 1.10 (0.20) mm, respectively. Mean and SD values of vertebral movements at L5–S1 were 3.68° (0.69) in flexion and mean and SD values of vertebral separations were 0.80 (0.15) mm, respectively. Clinicians have created similar movements. Increases were observed in IVF dimensions in terms of area, height, and width at the L4–L5 and L5–S1. Mean and SD values of IVF changes in area, height, and width at L4–L5 were 21.12 (3.87)%, 12.13 (1.89)%, and 5.12 (1.88)%, respectively. Mean and SD values of IVF changes in area, height, and width at L5–S1 were 18.02 (2.97)%, 8.11 (1.68)%, and 4.11 (1.40)%, respectively.
Conclusions:
Intervertebral motions and IVF dimensional increases were noticed during the flexion–distraction procedure.
Introduction
Low-back pain
Low-back pain (LBP) is one of the most common and costly conditions among musculoskeletal disorders.1,2 The lifetime prevalence of LBP in the United States may be as high as 84%. 3 The prevalence of chronic LBP is ∼23%, disabling 11%–12% of the population. 3 Despite extensive research efforts, the causes of LBP are mostly not well understood and some LBP has distinct causes. 4
Chiropractic treatment options
Manipulative procedures have been used for the treatment of LBP and are recommended for patients with LBP. 5 Several types of chiropractic manipulative procedures are available for treating LBP, including high-velocity low-amplitude spinal manipulations, traction-based procedures, and instrument-assisted very high-velocity low-amplitude techniques. 6 One of the commonly used techniques is known as Cox flexion–distraction technique and is used by 63.7% of the chiropractors for treating LBP patients. 7 This technique uses a specially designed table to assist the clinician to deliver forces and movements to the spine. Several clinical studies have demonstrated its clinical effectiveness for treating LBP patients.8–11
Vertebral movements and intervertebral foramen (IVF) dimensional changes
One of the hypotheses of spinal manual treatments is that the vertebral motion occurs as a result of the application of force during manual treatment. This leads to improvements in the lumbar spine function. 12 There are different forms of manual treatments for the lumbar spine broadly classified as spinal mobilization, spinal manipulation, and traction-based spinal manual treatments. To study this phenomenon, several investigators have done experiments on cadavers by inserting bone pins into vertebral bodies of the thoracic spine in human cadavers, and then calculated the relative movements of the vertebral bodies during high-velocity low-amplitude posterior-to-anterior thrusts in the thoracic spine. 13
Other investigators have used infrared surface markers or accelerometers placed on the spinous processes of the vertebra and measured vertebral movements on human volunteers during posterior-to-anterior manual thrusts in the thoracic regions.13–15 All these studies reported relative movement of target and adjacent vertebrae during the manipulative treatment. This result illustrates that there is movement of the target joint during thrust (quick application of force) application beyond the movement achieved by the preload (initial force before delivering thrust) force.12,13 Most of these studies focused on thoracic high-velocity low-amplitude spinal manipulations.
Few studies reported on the vertebral movements in the lumbar spine during manual therapy. These studies include vertebral movements during instrument-assisted very high-acceleration/-velocity thrusts.16–18 Few researchers reported on the movements during posterior-to-anterior spinal mobilizations, during traction type of loading conditions.19,20
There has been considerable interest in the understanding of the dimensional morphology of intervertebral foramen (IVF) and changes associated with these IVF dimensions in terms of height, width, and area during normal physiological movements.21–25
Flexion–distraction is another form of manual treatment and has evidence for treating low-back and lower extremity pain by randomized clinical trials.9–11,26 This involves repeated slow applications of forces that involve flexion and traction movements to the lumbar spine and no reports on the vertebral motions or the IVF changes were reported in the peer-reviewed literature. Because the spinal nerves pass through the IVF, these dimensions are of importance to understand the relative space they use in relation to IVF dimensions.
Objective of this study
The objectives of this study were to quantitatively determine (1) intervertebral motions and (2) changes in IVF area, height, and width in the lumbar spine during the application of a chiropractic procedure known as the Cox flexion–distraction.
Methods
Unembalmed cadavers
Eight unembalmed whole cadavers were used in this study (five males, three females; aged 43–87 years). The unembalmed cadavers were freshly frozen at −20°C immediately after death and thawed at room temperature for experimentation. The cause of death varied from heart failure to stroke. As this study used cadavers and did not involve human volunteers, institutional review board has determined that they do not need to review this study protocol.
However, all the research personnel followed all safety protocols developed by Occupational Safety and Health Administration (OSHA) by wearing appropriate protective equipment. A radiologist reviewed radiographic films of the degenerated disks and graded their status based on disk height and osteophyte presence. The degeneration level of the study's disks was mostly degeneration grade 3 (one specimen: grade 1, two specimens: grade 2, and five specimens: grade 3).
Intervertebral movement measurements
The results reported here are an extension of the preliminary results reported in a book chapter.27,28
An anatomy specialist dissected necessary paraspinal musculature to permit accurate insertion of metal rods into the vertebral bodies of L4, L5, and sacrum. Four infrared light-emitting diode markers were attached to the rods that were pinned to each of the vertebral bodies approaching posterolaterally. Figure 1 shows a photograph of the cadaver with the metal rods and infrared markers.

A photograph of a cadaver in a prone position showing the dissection and insertion of metal rods and infrared markers to monitor vertebral motion.
The placement of the cadaver was similar to a prone treatment position on a zenith-Cox treatment table (Model 90; Williams Healthcare Systems LLC, Elgin, IL, USA) used in treating LBP patients. The application of the chiropractic treatment procedure consisted of five 4-sec cycles of table movement in the downward direction in ∼20 sec with hand contact superior to the segment of interest. This process was repeated three times.28,29
The vertebral movements were monitored at L4, L5, and sacrum during the administration of the procedure by three experienced clinicians. Two of the clinicians have extensive clinical experience using this technique in private practice (30 and 10 years) treating LBP patients using the same procedure used in this research. One of the clinicians is highly experienced in teaching this technique to students for 20 years. An optoelectronic system consisting of three infrared cameras was used (OPTOTRAK Model 3020; Northern Digital, Inc., Canada).
A research assistant operated the computer to collect the three-dimensional position of the infrared marker data during the chiropractic procedure that was administered by an experienced licensed clinician. The data were collected during three separate applications of the flexion–distraction chiropractic procedure with 30-min intervals between each trial. All three clinicians carried out the flexion–distraction chiropractic procedure immediately after one another for each of the trials. Then there is a gap of 30 min between each trial of all clinicians.
Using the three-dimensional kinematic data, the relative movements between the L4 and L5 vertebrae and between the L5 vertebra and sacrum were calculated using the software provided by OPTOTRAK rigid body analysis software (First Principles; Northern Digital, Waterloo, Canada). In addition, custom-written software was used to convert to the vertebral coordinate system.
Data collection was carried out at 100 Hz sample rate and was saved as ascii data.
Each of the vertebrae was attached with four infrared markers representing a rigid body (for each vertebrae), the relative movements of each of the vertebrae relative to the inferior vertebrae were computed using the three-dimensional relative kinematic data using the standard rigid body kinematics in terms of three vertebral rotations and three translations.
After the completion of the experiments, the lumbar spines were dissected from the whole cadaver and IVF contours were digitized at 10 points (Fig. 2) using the infrared digitizing probe supplied by the OPTOTRAK system and IVF. The digitizing probe has several infrared markers and has a tip that can be placed on different points of the vertebrae foramen contour, and by placing the tip of the stylus and pressing a button on the computer, the digitized point was obtained by the OPTOTRAK software. All the digitized points were referenced to the vertebral center as the origin and local XYZ (positive X-axis pointing left laterally, positive Y-axis pointing superiorly, and positive Z-axis pointing anterior to vertebral body) axes system. Ten points on each of the IVF were digitized (as shown in Fig. 2).

Schematic diagram of intervertebral foramen contour and the 10 points digitized.
Mean values of the vertebral movement at the distracted position relative to the initial prone position were computed for the three trials. From these the average and standard deviation (SD) values for all the eight cadavers were obtained.
From these 10 points, the changes in the IVF area, height, and width were computed using the vertebral movement data and the digitized points. The IVF height was calculated by the separation distance from the top point of the superior vertebra to the bottom point on the inferior vertebrae. Width was calculated from the posterior point to the anterior point, and the area was calculated by formulating triangles from three points at a time and computing the area and summing the area of all the triangles.
Results
Vertebral movements
Figure 3 shows a typical plot of vertebral movements at the L4–L5 joint during the chiropractic procedure (five 4-sec applications of the flexion–distraction). The graph shows the vertebral movements in three dimensions (three rotations and three translations) as a function of the duration of the procedure. The major movements were flexion angle, anterior translation, and longitudinal distraction.
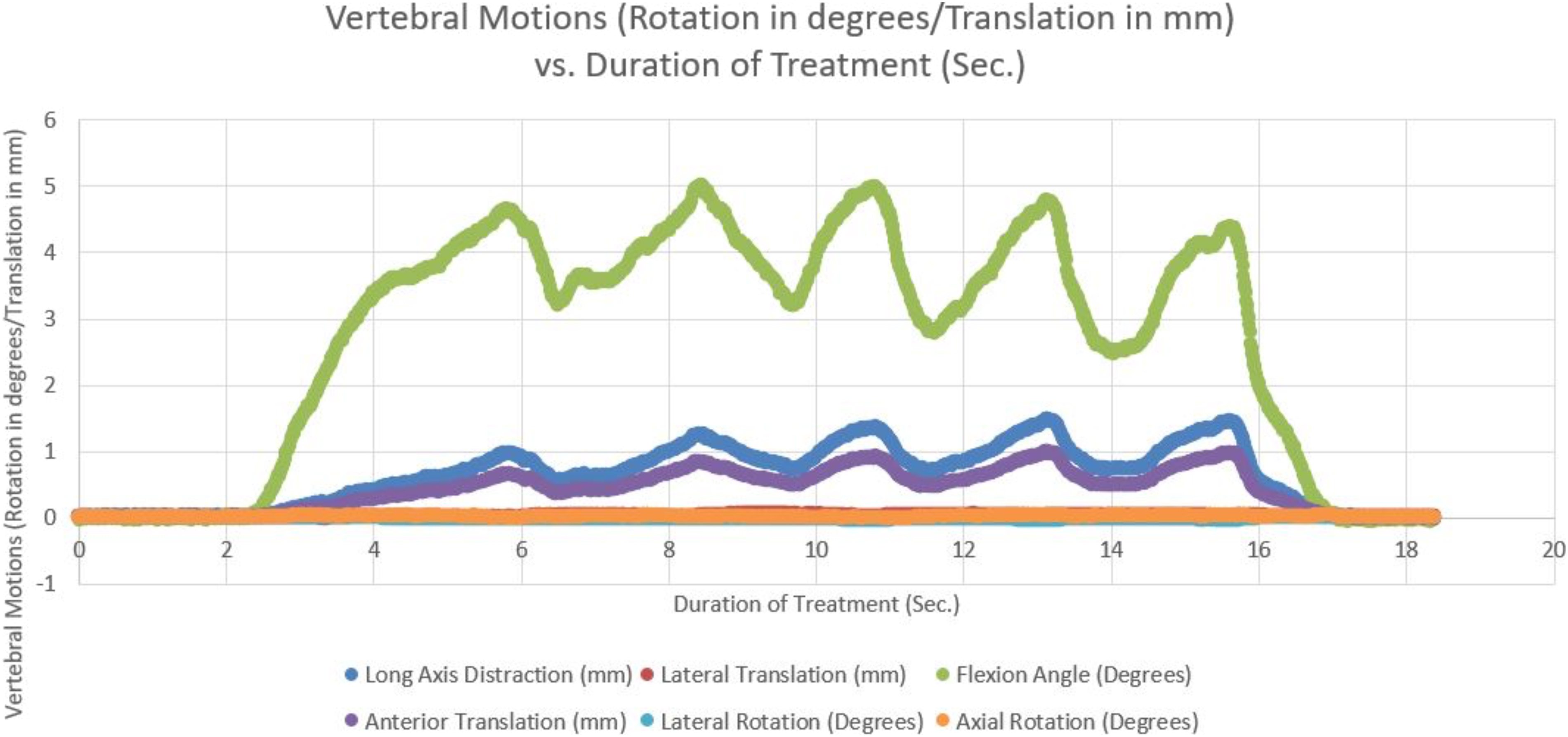
A typical graph showing movements of vertebrae in three dimensions during the chiropractic procedure.
Table 1 provides the mean and SD values of the vertebral movements occurred in the final distracted position based on the eight cadavers for three clinicians and the average of all three clinicians. Based on the results of this study, the three clinicians had similar results.
Mean Vertebral Movements (Rotations in Degrees/Translation in Millimeter) During a Chiropractic Procedure
SD, standard deviation.
Table 2 provides the mean and SD values of the changes in IVF area, height, and width in the initial prone position before the treatment and in the final distracted position based on the data from eight cadavers.
Mean Intervertebral Foramen (Height, Width, and Area) Dimensional Changes During a Chiropractic Procedure
Discussion and Conclusions
This study measured the vertebral movements in the lumbar spine on unembalmed cadavers during the flexion–distraction procedure. The flexion–distraction treatment was based on the hypothesis that the vertebrae flex, separate, and create increased foraminal spaces to provide an opportunity to reduce pressures in the nerve roots.
Vertebral movements during high-velocity thrusts and using activator type of instrument resulted in vertebral movements of <1 mm.17,18 Posteroanterior (PA) forces applied at the L5 spinous process during lumbar spinal mobilization by Kulig et al showed extension movements of 3.6° at L5–S1 and 1.9° at L4–L5. 19 Studies under traction to lumbar spine reported on the reduction of lumbar lordosis and separation of vertebrae of the order of 1 mm. 20 All these studies used PA forces or traction type of loading.
The vertebral movements observed in this study were higher in flexion and distraction compared with the movements observed in the other studies.16–20
IVF dimensions and the changes observed are comparable with the other research studies during flexion movements.21–24
The vertebrae moved in flexion and traction, separating from each other, thereby, increasing the foraminal area, height, and width, which returned to their original values when the spine was unloaded to the initial prone position. Randomized clinical trials have demonstrated the pain reduction and improved function while LBP and lower extremity radiating pain were reduced significantly.8,11 The opening of the IVF could potentially reduce the pressures in the nerves and potentially contribute to reduction of pain. This speculation needs to be investigated with in vivo clinical and translational studies.
Also the changes observed in this study were transient and one needs to be cautious in interpreting the results. Randomized clinical trials have also shown improved function after flexion–distraction treatment, and studies investigating these clinical improvements should be investigated with in vivo basic science studies to find relationships. Future studies should aim to measure intervertebral motion during in vivo situations on LBP patients and correlate with clinical improvements.
The following limitations should be noticed. The study was conducted on cadavers, and some of the musculatures were dissected to place the metal rods and sensors. The sample size of this descriptive study was very small, and studies with larger sample sizes need to be undertaken. The cadavers were mostly from deceased individuals with elderly and degenerated spinal conditions. In vivo conditions could influence the results of the study, and studies are planned to measure the intervertebral separation using ultrasound while administering this treatment procedure.
Conclusions
The Cox flexion–distraction chiropractic procedure created vertebral movements at L4–L5 and L5–S1 levels. It also increased IVF dimensions at L4–L5 and L5–S1 levels based on unembalmed whole cadaver experiments. These changes were transient. Further in vivo studies are needed to validate the observations and their effect on clinical situations.
Footnotes
Data Availability Statement
All data sets presented in this study are available upon request.
Ethics Statement
The specimens were acquired from the body donation organizations Anatomy Gifts Registry program (AGR, Chicago IL, USA) and Science Care (Science Care, Inc., Phoenix, Arizona, USA), which declared that written informed consent of the donors was obtained before decease.
Authors' Contributions
M.R.G. and A.G.P. contributed to funding acquisition, discussion, and article review. G.D.C. was involved in study design, specimen preparation, and experimental testing, discussion, and article review. All authors contributed to the article and approved the submitted version.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors acknowledge the financial support of Health Resources and Services Administration (HRSA) through Grant No. 1R18 AH10001-01A1. Financial donations were received from numerous chiropractic physicians and Williams Healthcare Systems Incorporated who donated the chiropractic table.