
Abstract
Introduction:
Although acupuncture and moxibustion are complementary or alternative therapies for glaucoma, studies on their effectiveness reported in the Cochrane Database of Systematic Reviews are inconclusive. Stress-free (SF) therapy is a type of moxibustion therapy that targets acupuncture points and increases blood flow in the ocular fundus. This study aimed at evaluating the clinical efficacy of SF therapy in treating normal-tension glaucoma.
Methods:
In addition to visual field test (mean deviation [MD]) and visual acuity measurement, blood tests were performed to measure the following in a man aged 63 years and a woman aged 69 years with glaucoma without ophthalmic intervention and with mild cataract: triglycerides (TG), arteriosclerosis index (AI) determined as the low-density lipoprotein/high-density lipoprotein ratio, total lipids (TL), and estrogen (estradiol-2 [E-2]). SF therapy was performed by the patients themselves for 45 min daily for 4 weeks at a total of four points: Zusanli Point (ST36), Point F (the intersection between the 1st or 2nd toe line of the left sole and the medial/lateral malleolus line), Point N (the intersection between the vertical line of the right pupil and the middle line of the nasolabial fold), and Point P (the center of the closed left eyelid).
Results and Discussion:
In both patients after SF therapy, TG, AI, and TL levels were reduced, while E-2 levels were elevated. These changes may improve lipid metabolism and decrease vascular resistance, affecting ciliary-regulated circulation of the visual field. Elevated estrogen has a protective effect on the retinal ganglion cells and improves blood flow. Estrogen therapy after menopause is associated with a reduced incidence of glaucoma. Thus, in our patients, estrogen (E-2) levels elevating from 15.5 pg/mL at baseline to 22.5 pg/mL after SF therapy may have contributed to the improved visual function.
Conclusion:
SF therapy improved the visual acuity and visual field (MD score) in two patients with normal-tension glaucoma.
Introduction
Although acupuncture and moxibustion are complementary or alternative therapies for glaucoma, studies on their effectiveness reported in the Cochrane database of systematic review are inconclusive. 1 Stress-free (SF) therapy is a type of moxibustion therapy that targets acupuncture points and increases blood flow in the ocular fundus. 2 This study was aimed at evaluating the clinical efficacy of SF therapy in treating normal-tension glaucoma.
In SF therapy, a moxibustion therapy device (controlled medical device certificate approval no. 224 AFBZX00075000; Japan) applies thermal stimulation at <48°C without causing burns to four points on the body surface, including acupuncture points, with pinpoint accuracy using thermoconductor probes of 1.5-mm diameter. SF therapy significantly reduces the oversecretion of stress markers (acetylcholine hormone and cortisol) that are elevated in response to stress, thus normalizing blood pressure, improving metabolism in diabetes, and increasing blood flow in the ocular fundus.2–8 In particular, it activates regulatory B cells (B-regs) that are involved in the suppression of inflammation by interleukin-10 in the peripheral blood lymphocytes. 8 Based on the above mechanism of action of SF therapy, we performed SF therapy in two patients with normal-tension glaucoma and observed improvement in the visual acuity, field, and function.
Methods
The study protocol was approved by the Bioethics Review Board (registration no. 1942). Furthermore, informed consent was obtained from each patient. There are no conflict of interest matters in this study.
We enrolled two patients, a 63-year-old man and a 69-year-old woman, with normal-tension glaucoma and mild cataract of Emily Little Grade (R/L: grade I). The patients had undergone no ophthalmological and internal medicine intervention before, and a routine health checkup had revealed abnormal visual function and elevated triglyceride (TG) levels (normal range: 35–149 mg/dL). The effects of SF therapy were evaluated based on the mean deviation (MD) score in Humphrey perimetry and visual acuity. Laboratory parameters, including TG, total lipid (TL), and estrogen (E2) levels, the atherosclerosis index (AI) determined as the high-density lipoprotein (HDL)/low-density lipoprotein (LDL) ratio, were also analyzed. To ensure consistency, all inspection data were collected at the same time of the day in consideration of the impact of measurement time and circadian rhythm on test values.
Furthermore, changes in visual function after SF therapy from those before this therapy were analyzed on the basis of the data obtained by the FT-10 tonometer (Tomey, Japan) measurement conducted under identical conditions, with circadian rhythm influences and so on taken into account. A blood sample of 8 mL was collected from the cubital vein and sent to the Showa Medical Science (Tokyo, Japan) for analysis. For SF therapy, we selected four stimulation points that are associated with increased ocular fundus blood flow 2 (Fig. 1): (1) Point P, upper part of the left closed eyelid; (2) Point N, intersection of the vertical line of the right pupil and the middle line of the nasolabial fold; (3) Point F, intersection of the first or second toe line of the left sole and the medial or lateral malleolus line, and (4) Zusanli point (ST36), midpoint between the tibial tuberosity and the fibular head.

Stress-free therapy. (1) Stress-free therapy device equipped with four electrodes of a probe with a diameter of 1.5 mm. Controlled Medical Device Certificate (Approval No.: 224AFBZX00075000; Japan). (2) Point P (center of the closed left eyelid) and Point N (an intersection between the vertical line of the right pupil and the middle line of the nasolabial fold). (3) Point F (intersection between the 1st or 2nd toe line of the left sole and medial/lateral malleolus line). (4) Zusanli point (ST36) (midpoint between the tibial tuberosity and fibular head outside the left knee.
Using an SF therapy device (controlled medical device certificate approval no. 224 AFBZX00075000; Japan) equipped with four thermoconductor probes (1.5-mm diameter, temperature <48°C), heat stimulation was applied to the four points by the patient for more than 45 min daily for 4 weeks.
In addition, this study period has received no treatment other than SF therapy. The usage and treatment points of the treatment device at home were accurately confirmed by the photograph guide (Fig. 1), and daily changes in physical condition and confirmation of accurate SF therapy were recorded on the chart.
Results
Case 1: For the man with right-eye glaucoma (left normal), the MD score in the Humphrey perimetry (index of glaucoma progression) improved from −15.09 to −12.97 db in the right eye (Fig. 2), with enlargement of the circled visual field region in the figure. There was no change in intraocular pressure (IOP; 11 mmHg) or mild cataract of Emily Little Grade (R/L: grade I) in the right eye, but the corrected visual acuity improved from 0.8 to 0.9 in the right eye and from 1.2 to 1.5 in the left eye.
Case 2: For the woman, the MD score in Humphrey perimetry improved from −2.75 to −1.98 db in the right eye (Fig. 3) and from −2.87 to −1.04 db in the left eye (Fig. 4), with enlargement of the circled visual field region in the figure. There was no change in her cataract Emily Little Grade (1/1), but her IOP decreased from 15 to 14 mmHg in the right eye and from 21 to 16 mmHg in the left eye. The corrected visual acuity improved from 1.0 to 1.2 in the right eye and from 1.0 to 1.2 in the left eye.
Laboratory findings included elevated TG exceeding the reference range (35–149 mg/dL) in both patients before treatment and TG levels within the reference range after treatment (from 169 to 134 mg/dL in the man and from 457 to 186 mg/dL in the woman). The mean TG decreased from 313.0 ± 203.6 mg/dL before SF therapy to 160.0 ± 36.8 mg/dL after SF therapy. Similarly, the mean HDL/LDL ratio or AI decreased from 3.0% ± 0.2% to 2.7% ± 0.1%, and TL decreased from 858.5 ± 299.1 to 720.0 ± 100.4 mg/dL, indicating improvement in these parameters in both patients (Table 1). In addition, the estrogen (estradiol-2 [E-2]) levels were increased from 15.5 ± 4.9 to 22.0 ± 1.4 pg/mL after SF therapy (Table 1).
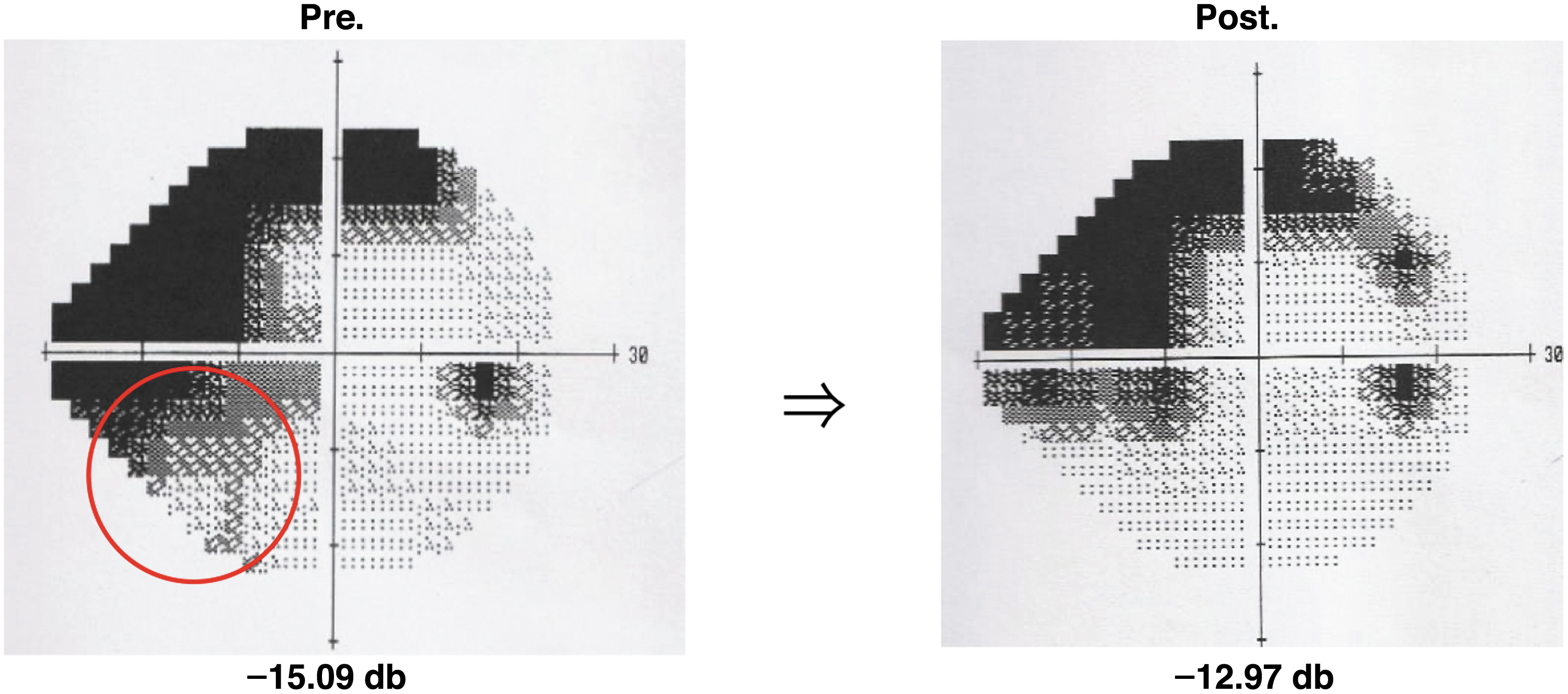
Changes in the Humphrey perimetry. Changes in the MD score in the right eye of the 63-year-old male patient. MD, mean deviation.

Changes in the Humphrey perimetry. Changes in MD score in the right eye of the 69-year-old female patient.
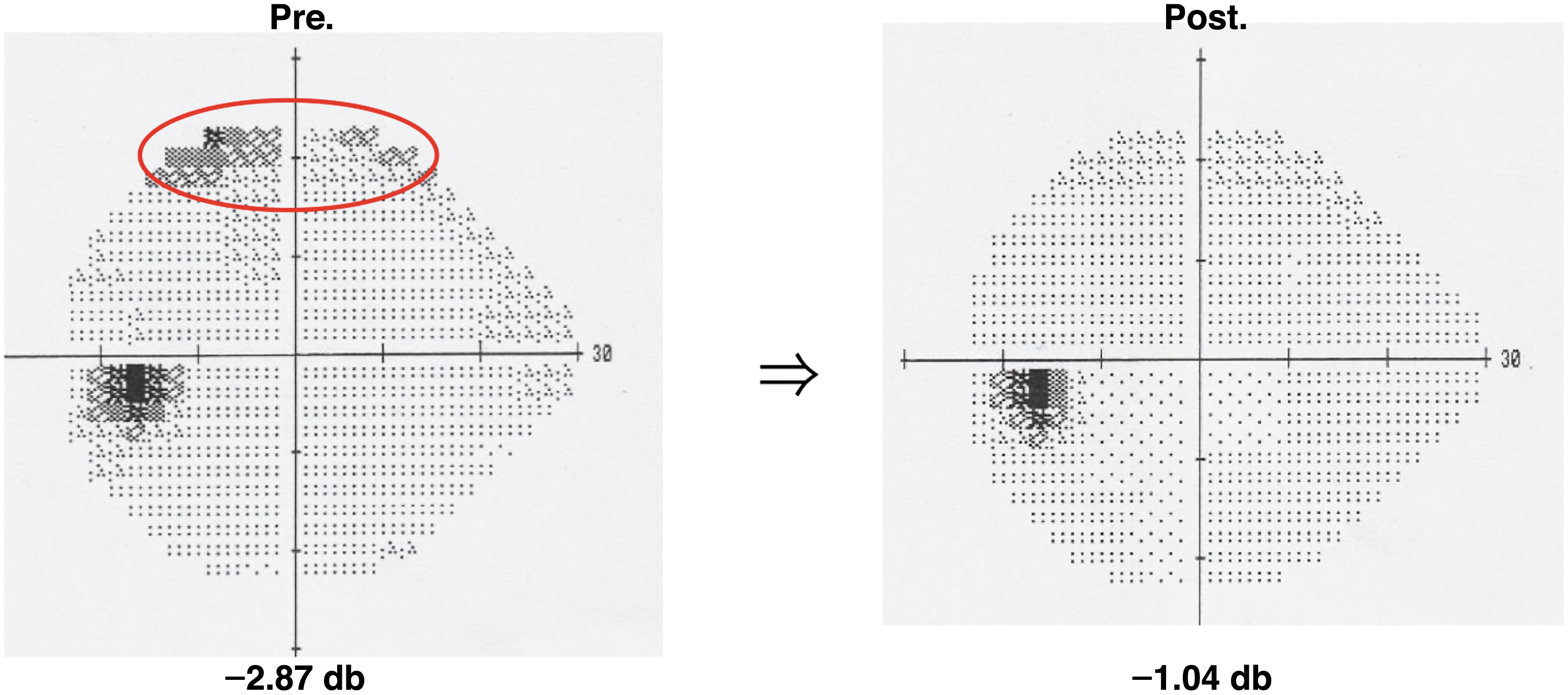
Changes in the Humphrey perimetry. Changes in the MD score in the left eye of the 69-year-old female patient.
Blood Findings' Data
AI, arteriosclerosis index; AV, average; E-2, estradiol-2; SD, standard deviation; TG, triglyceride; TL, total lipid.
Discussion
A study that randomly performed visual function tests on individuals aged ≥40 years living in Tajimi City, Japan (n = 3870), found that the main causes of reduced visual acuity were age-related cataract and glaucoma. The average IOP in the Japanese population is 14.5 mmHg, with a normal range of 10–20 mmHg. 9
With this background, we investigated whether SF therapy could be a complementary or alternative treatment option to improve and prevent glaucoma in two patients with normal-tension glaucoma. The results showed that improvement in the MD score of Humphrey perimetry was accompanied by TG levels decreasing to the reference range, and an improvement in TL levels and the HDL/LDL ratio (AI) estrogen (E-2) levels was also elevated.
Consistent with our findings, a meta-analysis showed that elevated TG is a risk factor for glaucoma progression. 10 Furthermore, reduced estrogen secretion is associated with accelerated optic nerve aging. 11 Thus, SF therapy might improve visual function and TG, TL, and AI by increasing estrogen secretion.
Estrogen (E-2) has also been suggested to protect retinal ganglion cells and improve ocular fundus blood flow.12–14 Paula et al. 15 reported that the incidence of primary open-angle glaucoma was low in patients who received hormone therapy with estrogen after menopause. These results suggest that the improvement in the visual field MD score (glaucoma progression index) by SF therapy seems to have involved an increase in estrogen (E-2) from 15.5 ± 4.9 to 22 ± 1.4 pg/mL, which has reduced the AI, because estrogen (E-2) has an antiarteriosclerotic action. 16
Meta-analyses17,18 have shown that glaucoma is often complicated by arteriosclerosis, dyslipidemia, and diabetes, suggesting its association with metabolic abnormalities. SF therapy decreases stress markers and improves diabetes and metabolism2–7 ; these effects are likely to have contributed to the reduced TG and TL levels and HDL/LDL ratio (AI) (Supplementary Table S1 and Supplementary Table S2).
The increase in the levels of estrogen (E-2) may be attributable to the improvement in visual acuity and visual field. Estrogen (E-2) has been suggested to protect the retinal ganglion cells and to lower IOP. 10
In patients with these glaucomatous disorders, SF therapy may have improved lipid metabolism and vascular resistance by decreasing TG and TL levels and the HDL/LDL ratio (AI) and by improving optic nerve conditions by increasing estrogen (E-2) secretion, which affects ciliary-regulated circulation of the visual function.
Although the Cochrane database of systematic reviews has not reached a reliable conclusion to support the effectiveness of acupuncture or moxibustion for glaucoma in relation to visual function assessment or drug therapy, the benefit of SF therapy can be confirmed by accurately evaluating visual function and other arteriosclerotic factors. We plan to further accumulate cases to analyze the relationship among visual function, arteriosclerotic factors, and estrogen levels.
Conclusion
Our study suggested that SF therapy was a useful complementary/alternative therapy for improving visual function in two patients with normal-tension glaucoma.
Footnotes
Acknowledgment
The authors would like to thanks the Ryotokuji University Grants Commission for supporting this research.
Authors' Contributions
Author contribution statement detailing each author's participation in the work. K.I.: Writing, editing, experimentation, analysis of data, and data collection. S.K.: Experimentation. T.N.: Editing, writing, and coconceptualization. K.R.: Validation of data, editing of the article, conceptualization, study design, and editing.
Author Disclosure Statement
The authors declare no conflict of interest.
Funding Information
This study has been supported by the Ryotokuji University Grants Commission via No. 201 (June 2020).
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.