
Abstract
Rhythmic embrocation (also called rub or, as originally in German, “Einreibung”) was developed by Dr. Ita Wegman and Dr. Margarete Hauschka in the 1920s as a care measure to stimulate recovery processes. It is based on contact with the client’s/patient’s skin, in which an oil, emulsion or ointment is applied by the therapist in rhythmic movements, and can be used, for example, as a partial embrocation on the feet. To date, no reports on its application to adults with intellectual, cognitive and/or physical disabilities exist. The aim of this survey is to provide a hands-on practical proof of concept of foot embrocation for adults with such disabilities, and who live in residential units. The data were collected by means of an anonymous retrospective survey among residential facility staff who had undergone training in therapeutic foot embrocation. Their training consisted of two learning units of four lessons each and a practice period. The residential staff were then able to gain further experience in applying foot embrocation over a period of up to three months, after which they were invited to participate in the survey. The survey was based on a questionnaire consisting of 36 questions mostly focused on their disabled clients, whom the trained staff could observe while carrying out their professional duties. Of the 53 questionnaires handed out to users, 37 were completed and returned by post. Almost all users found the eight lessons sufficient as training for foot embrocation. Half the clients were female, half male, and their most common disabilities were autism, trisomy 21, and epilepsy. They used a variety of verbal and non-verbal communication types. In most cases, the residential staff perceived the clients as being relaxed before the embrocation and appreciating it. Improvements in depth of breathing and circulation, activity and sleep were noticed by some users. Considering the short training period, the implementation of this therapy in residential facilities for people with disabilities seems promising. Adults with various disabilities living in residential facilities responded well to rhythmic foot embrocation performed by the facility’s trained staff.
Introduction
Rhythmic embrocation (also often called rub or, as originally in German, “Einreibung”) was developed by Dr. Ita Wegman and Dr. Margarete Hauschka in the 1920s as a care measure for stimulating recovery processes. Like other forms of external applications in Anthroposophic Medicine, 1 such as rhythmic massage therapy, pressel stream massage and compresses, rhythmic embrocation aims to stimulate salutogenic processes and autonomic self-regulation. 2 It is used in a variety of ways, for example, as a partial embrocation on the feet, legs, stomach, arms, back, on the organs or as a whole-body embrocation. During the embrocation, an oil, an emulsion or an ointment is rhythmically applied to the skin, following a clearly defined procedure and using the hands, which should be warm and supple. They should also establish a connection with the client’s skin by moving in clear patterns and gently gliding over the tissue without pressing, displacing or deforming it. After the embrocation, a therapeutic resting period should follow. Several aspects of embrocation might positively influence the client, namely the therapist’s touch, the substance applied and the calming environment. 2
A training in rhythmic embrocation according to Wegman/Hauschka can be completed at one of the national Anthroposophic Nurses Associations. The following are the countries where this is possible: Switzerland, Germany, France, Spain, Sweden, Japan, Taiwan, New Zealand, North America, and Brazil (Supplementary Table S1). All national associations of anthroposophic nurses are members of the International Council of Anthroposophic Nursing Associations (ICANA), an umbrella organization that supports its members in the development of anthroposophic nursing in their national health systems. Moreover, ICANA promotes and sponsors the International Forum for Anthroposophic Nursing (IFAN), an organization for certification and accreditation to ensure the quality of education and training programs in anthroposophic nursing.
The physiology and even biochemistry of touching processes have recently become much better understood. 2 For instance, a complex system of nerve fibers on the skin has been discovered, and evidence suggests that C-tactile afferents in the skin are, in particular, responsible for propagating the increased vagal activity that may mediate the positive effects of touching. At the hormonal level, important roles have been ascribed to oxytocin, which is crucial for social interactions and well-being. Interestingly, the importance of movement in successful applications is also becoming more apparent. 3
Disabled persons with daily support needs are intensively confronted with their own health-related limitations—including limited autonomic self-regulation—and dependency on others. While they might particularly benefit from salutogenic impulses provided by external applications, it is conceivable that they could have mixed feelings about them. Among the various types of embrocation, foot embrocation appeared to us to be the most appropriate: it can be done with a minimum of invasiveness, requires only a couple of minutes (not counting the therapeutic rest), and can be easily integrated into daily life, for example, after washing their feet or when a substance needs to be rubbed in. Other types of foot massage have been shown to result in reduced anxiety (e.g., in postmenopausal women 4 ) or to improve sleep and social participation (in autism 5 and cognitive, physical, or psychiatric impairments 6 ).
Before this study, it was not known—at least to our knowledge—how disabled people in need of support, who live in residential units for persons with intellectual, cognitive and/or physical disabilities, would react to foot embrocation as developed by Dr. Ita Wegman and Dr. Margarete Hauschka. As it would be difficult to conduct a survey with adults with disabilities whose communication skills may be limited in different ways, we conducted a survey among residential facility staff who had been trained to administer this type of embrocation. Our aim was collecting and evaluating their experiences regarding training, application, and reactions of their clients.
Methods
Study Design
Residential facilities were contacted about the possibility of training their staff in foot embrocation. In those institutions that agreed to try out such a training, data were collected six or more months later, between April 2023 and February 2024, by means of an anonymous retrospective cross-sectional survey among the trained residential staff (often referred to as “users”). The survey covered their experience in applying foot embrocation with plant oils to disabled clients in need of support. The six participating institutions were: the Ekkharthof Association (in German “Ekkharthof Verein,” Lengwil, Canton Thurgau; 17 instructed users); the Residential Home Zürichberg (“Wohnheim Zürichberg,” Zurich, Canton Zurich; 10 users); the Work Home Neuschwende (“Werkheim Neuschwende,” Canton Appenzell Ausserrhoden; 8 users); the Gempen Sonnenhalde Öpfelsee (“Gempen Sonnenhalde,” Canton Solothurn; 7 users); the Sonnenhof (Arlesheim, Canton Baselland; 7 users) and the Humanushaus (Rubigen, Canton Bern; 6 users).
Ethics Statement
This study was carried out in accordance with Swiss laws and regulations. In compliance with the Swiss Federal Law on data protection (Human Research Act, Article 2) and since the data were collected in the context of a survey among professionals, no particular authorization was needed. This was confirmed by a jurisdictional declaration of the ethics committee of northwest and central Switzerland (“Ethikkommission Nordwest- und Zentralschweiz; Req-2022-01249, 26.10.2022).
Selection and Description of Participants
The present survey study was conducted in six institutions without specific sampling. All previously trained residential staff were invited to participate in the survey if they: (1) received training consisting of two learning units of four lessons each on rhythmic foot embrocation as developed by Dr. Ita Wegman and Dr. Margarete Hauschka, (2) completed a three-month training period, and (3) then gained professional experience in foot embrocation during a further up to three-month period in which they applied it to at least one disabled adult client. No further conditions or selection criteria were applied. The training was given by Therese Beeri, an expert in anthroposophic care and rhythmic embrocation according to Dr. Ita Wegman and Dr. Margarete Hauschka and a trainer with many years of experience. The questionnaire was deposited at the participating facility together with a cover letter. The residential staff were instructed in writing to think of the client they remembered best and had observed the longest when answering the client-related questions.
Questionnaire
The questionnaire was developed by an interdisciplinary team of three scientists and two therapists who use foot embrocation according to Dr. Wegman and Dr. Hauschka. The team evaluated and adapted the questionnaire in several test runs until it met all requirements—including good readability and clarity—and was coherent. The final questionnaire was in German and consisted of 36 high-level questions, mostly multiple-choice questions grouped in the following sections: (1) information about the client (adult in need of support), (2) information on reactions to rhythmic foot embrocation, including (3) aspects of autonomic function, such as those related to orthostatic-circulatory, rest/activity and digestive rhythmical regulation, 7 and other health-related quality of life items, (4) data about the residential employee, and (5) the residential employee’s comments on the rhythmic foot embrocation procedure. All questions about clients relate to the experiences of previously trained residential staff while applying foot embrocation to the client whom he/she remembered best and accompanied the longest. All data reflect the interpretation of the questions by the previously trained residential staff and their perception of the client’s reactions to embrocation.
Data Collection
A total of 53 envelopes, each containing an information sheet, the questionnaire and a pre-paid return envelope, were handed out to the previously trained residential staff potentially eligible to participate in the survey. It was emphasized that the envelopes should be sealed after inserting the completed questionnaires to ensure anonymity. The reported data were treated confidentially and were not passed on to third parties. Data were entered manually into RedCap and checked by RedCap’s own plausibility routines to minimize human input errors. All data was then exported from RedCap and later imported into an SPSS database (version 29.0 for Windows, IBM® SPSS® Statistics).
Statistical Analysis
Descriptive statistical analyses were performed using IBM® SPSS® Statistics (version 29). No variables were modified. Data are shown as numbers, missing answers are indicated in Tables 1–5 and in Figure 1. In the tables and figures, the various answer categories are depicted in the same sequence as in the questionnaires.
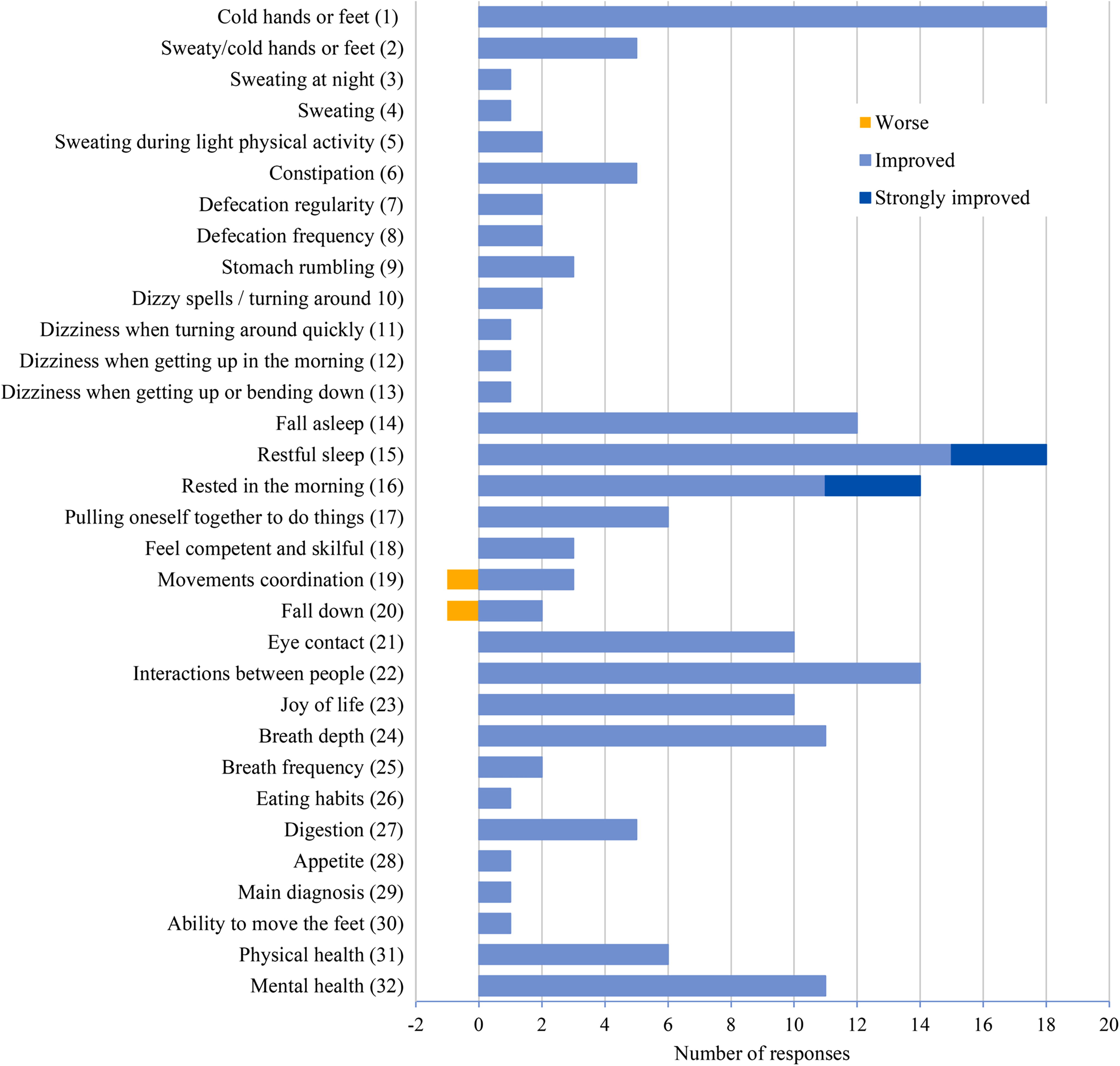
Changes in aspects of autonomy regulation and quality of life of the clients as perceived by the users. Possible answers were “I don’t know,” “it got worse,” “stayed unchanged,” “improved,” and “strongly improved.” The number of responses for “it got worse” is shown as negative values and in orange, the number of responses for “improved” and “strongly improved” are shown in light and dark blue, respectively. Remaining answers were either “unchanged” (given by between 6 and 20 users, depending on the question) or “I don’t know” (6 to 15 users); the number of missing answers varied between 6 and 23.
Characteristics of the Clients Who Received Foot Embrocation by the Instructed Users (N = 37)
Which others: developmental delay due to traumatic experiences; FAS and mental developmental delay; fragile X syndrome; early childhood disability; birth-related impairment; mental handicap; mental developmental delay; hydrocephalus; cognitive developmental delay; complex deformities of the feet (orthopaedic shoes); constipation and hysteria; Sturdge Weber syndrome; and suspected autism spectrum.
Which others: three-sentence language, through loud, differentiated breathing; is very good at copying the speech of others and it seems as if could speak very well (sometimes gives appropriate answers, often the answer does not match the question); with sounds, laughter; with occasional syllables, gestures; non-verbal (facial expressions…); speaks in “sentences”; and slurred speech.
Which others: … connected with the verbal language; eye contact; through facial expressions and gestures; clapping, jumping up, slapping, hitting someone on the head, smiling, repeating sequences of sounds; body tone, mimic, noises; laughter, movements with right arm/hand or with the right foot; facial expressions (n = 3); facial expressions (smile…); shouting; screaming, body language.
Results
Of the 53 questionnaires handed out to residential staff trained in embrocation, 37 were completed and returned via post by February 29, 2024 (overall response rate: 70%). The trained residential staff who participated in the survey reported working in one of the following Swiss institutions: 13 participants at Ekkharthof Association (in German “Ekkharthof Verein,” Lengwil, Canton Thurgau); 7 at Residential Home Zürichberg (“Wohnheim Zürichberg,” Zurich, Canton Zurich); 6 at Work Home Neuschwende (“Werkheim Neuschwende,” Canton Appenzell Ausserrhoden); 5 at Gempen Sonnenhalde (“Gempen Sonnenhalde,” Canton Solothurn); 4 at Humanushaus (Rubigen, Canton Bern); and 2 at Sonnenhof (Arlesheim, Canton Baselland). No questionnaire was excluded from the present work. The analysis was, therefore, performed using data provided by 37 users on their experiences with embrocation applied to 37 clients.
Clients’ Health Status and Preparation for the Embrocation
Approximately half of the clients were female (n = 20) and half male (n = 17), their health status being mostly perceived as good (n = 20) or less good (n = 12) by the residential staff. Their most frequent handicaps were autism (n = 13), followed by trisomy 21 (n = 7) and epilepsy (n = 6). The types of verbal and non-verbal communication used varied considerably (Table 1). Only in 14 cases, the verbal communication was considered to be good; in 13 cases, the clients’ communication was by making noises (n = 13) or pointing to something (n = 9).
When asked about possible requirements for performing rhythmic embrocation on the clients (Table 2), most residential staff reported that it had to be announced (n = 31), applied when a resident had an inner centered attitude (n = 22) and carried out in the presence of an accompanying person (n = 15). Fourteen clients had shown signs of tension before embrocation (n = 14), even though most (n = 20) were not tense. In contrast, in most cases, the residential employee perceived the clients as relaxed, because they were either lying still (n = 14) or had a relaxed facial expression (n = 8).
Requirements to Perform Rhythmic Foot Embrocation (N = 37)
What else: …a sufficient degree of calm and contact; the person initially looked several times during a foot embrocation; a comfortable lying position, before that usually a walk (motor restlessness, urge to run); a good place to sit; consent before I started rubbing; not react to the initial restlessness of the client (“You may be restless now and find peace. I am here”); peace, being undisturbed; calm atmosphere; and stillness.
Which others: with excessive tension, the embrocation was ineffective; depending on the situation, the client was previously tense (psychological tension); walked restlessly around the room; the client used the situation to talk; it caused effort to be verbally calm; partly strong physical tension (spasticity); sometimes restless, nervous, tearful; restless, tearful, aggressive.
Which others: lay quietly with slight tension; if not tense, smiled.
As autism was the most common disability (n = 13), a sensitivity analysis was conducted for this subgroup only. The answers to the question about what was required in order to apply the embrocation to the client (multiple answers possible) revealed that announcing the treatment (n = 10) and an inwardly centered posture during the treatment (n = 10) were required to perform the embrocation in this subgroup, while eye contact, speaking softly or humming a melody did not seem to help (n = 1 in each case). The presence of an accompanying person who was seen as trustworthy by the clients was perceived as helpful in some cases (n = 7).
Perceived Clients’ Reactions to Foot Embrocation
As presented in Table 3, most trained residential staff (24 out of 37) dedicated themselves to the client for three or more months and (23 out of 37) applied one embrocation per week. When asked how many embrocation applications were performed in a day, only one employee responded “twice,” while 30 answered “once.” In most cases (21 out of 37), the residential staff perceived that the client clearly improved after the rhythmic embrocation, most frequently for the moment (20 out of 37) or for a day (11 out of 37).
Information on the Application of Rhythmic Foot Embrocation (N = 37)
Which other oil: foot cream; cinnamon wine root oil; orange oil; almond oil; Solum (n = 9).
Whether habits or needs developed during the embrocation appointments was reported very differently (Table 4). Seventeen trained residential employees denied that habits or needs had developed. Of the remaining staff, 8 stated that new habits or needs developed in part of the sessions (i.e., sometimes) and 11 noted them every time. Features common to most reported habits/needs seem to be related to relaxation/calm and the clients’ desire for additional, regular embrocation.
Reactions to the Rhythmic Foot Embrocation (N = 37)
Habits that were manifested sometimes: says is calmer; stayed lying down for a while afterwards even if it was not bedtime; wanted the treatment to be done regularly; wished to lie down a little longer; sometimes asked when would get another one; got oil for embrocation; fell asleep.
Habits that were manifested every time: the oil used had to be dried off the feet with terry towels; always shows when sees me that wants another embrocation; found the embrocation pleasant and wants it again; was able to lie relaxed for a surprisingly long time and seemed calm and content; asked every evening for an embrocation and says that it does a lot of good; lies relaxed in bed for about 20 minutes; has a long rest; after the weekly foot bath that we always do, now insists on the foot embrocation; asks when I will give her another embrocation; wants to walk and stand more; wishes to be covered up and have a rest after.
Other signs of anxiety about touching: gently move both feet apart during the embrocation.
Other positive reactions (from the client) about touching: on the digestive tract, which began to “work”; eyes closed with “mmh” sounds (sign of well-being) and smiling; relaxed face; “dreamy” look.
Characteristics of Instructed Users Who Applied Foot Embrocation to Clients (n = 37)
One user answered that 10 lessons are needed, another that 16 lessons are needed.
Fear of being touched was hardly noticed. Instead, various positive reactions to the embrocation were perceived: in breathing, in the musculature in general, in relaxation (legs or feet), and most frequently through facial expression, gestures and verbal statements. Several survey participants made use of the possibility to report reactions that were not mentioned in the questionnaires (Table 4). Interestingly, no one mentioned tickle reactions, which might be expected outside of a therapeutic setting. In most cases, no change was noticed in the relationship with the client, but when a change was noticed it often occurred between the third and the tenth embrocation session.
Most users (29 out of 37) had the impression that their own quality of touch during rhythmic embrocation had improved over the course of the embrocation sessions and 35 out of 37 reported that the oil was well tolerated by the client’s skin. In almost all cases, embrocation was performed with peat oil, lavender oil or “Solum,” a mixed oil composed of raised bog peat (Solum uliginosum), horse chestnut (Aesculus hippocastanum), field horsetail (Equisetum arvense), and lavender essential oil.
Perceived Changes in Aspects of Autonomic Regulation and Quality of Life
All or almost all participants answered the questions covered in Tables 1–5. In contrast, there were more missing answers to a composite question on changes in 32 aspects of autonomic regulation and quality of life (Fig. 1 and Supplementary Table S2). A similarly high number of participants answered that the aspects “did not change” (Supplementary Table S2). Comparable results were obtained after excluding the survey participants with up to approximately 3 months of experience (sensitivity analysis; data not shown). Nevertheless, the number of participants who observed changes (improvement or worsening) in autonomous regulation and quality of life varied markedly. The higher numbers of improvements concerned breathing (breathing deeply), activity (joy of life, interactions with people, eye contact), sleep (rested in the morning, restful sleep, falling asleep), and circulation (cold hands or feet). Only one participant (out of 37) mentioned a case of worsening: the client’s coordination and falling became “worse.” No participant answered that an aspect had become “much worse.”
Information on the Embrocation Users, How They Evaluated Their Training and Their Comments
Most of the survey participants were women; they had a mean age of 48.4 ± 12.1 years old (ranging from 16 to 62 years of age). The majority were married (n = 13), had a high level of education (higher professional college; n = 16), and were born in Switzerland (n = 18) or Germany (n = 10). Almost all were currently responsible for four clients at the time (n = 33) and most worked 80%–100% (n = 22). Almost all participants found the eight lessons sufficient as a training for foot embrocation (n = 33), and more than half felt that the embrocation treatment was a success for the client in focus (moderately/clearly/strongly; n = 25). Table 5 provides detailed information on these and additional characteristics.
Twenty-three survey participants made use of the opportunity to make a final comment; one even sent a letter with the questionnaire. In summary, it can be said that most of the comments consisted of positive impressions of the use of embrocation. In several cases, difficulties in finding the time needed to apply the embrocation were mentioned. The interested reader may consult the Appendix for a rough translation of the comments received (Supplementary Table S3).
Discussion
Main Findings
The survey results show that the residential staff trained in foot embrocation often perceived the clients as benefiting from this therapy. The clients that the trained residential staff were thinking of while answering the survey questions were an equal number of females and males, with autism, trisomy 21, and epilepsy as their most common disabilities. To communicate they used a variety of verbal and non-verbal strategies. That these clients benefited from the foot embrocation treatment was strengthened by staff reports on active requests for embrocation from the clients. Improvements often remained for up to a day and were noticeable via positive changes in breathing depth, circulation, rest/activity regulation and sleep quality. It is evident that the residential staff perceived a wide range of beneficial reactions to embrocation. Almost all users noticed an improvement in their own quality of touch during the course of the various embrocation sessions. A logistical problem was, however, noticed by several staff members: namely, the lack of time to perform the embrocation.
Interpretation of Findings
Our results suggest that foot embrocation encourages an additional form of communication through touch, which is particularly valuable in these residential facilities where verbal communication may be limited. Rhythmic foot embrocation performed by the residential staff also appears to promote a sense of togetherness and shared well-being between residents and caregivers, strengthening social bonds that could be crucial for both professional fulfilment of the residential facilities staff and the emotional health of their clients. As far as these are concerned, some improvement in social bonds was to be expected, since it has been previously shown that another form of foot touch, that is, foot massage, leads to the central release of oxytocin, 8 a hormonal key-player in the biochemistry of social interactions. Touch-based therapies as a possibility to promote the central release of oxytocin deserve in our opinion particular attention, especially in view of disappointing results from studies on pharmaceutical oxytocin (e.g., the use of oxytocin nasal spray in autism spectrum disorder 9 ).
With respect to the expectations regarding autonomic self-regulation (cf. 7 ), some improvements of rest/activity regulation were observed by the trained residential staff (Fig. 1). The one case of perceived worsening (of movement coordination and falls) might have been associated with an impulse furnished by the embrocation for a change in the usual patterns of movement. The relatively low number of reported changes suggests that no improvements were noticed at the level of orthostatic-circulatory or digestive regulation (thermoregulation). However, our results do not allow us to clarify whether changes—improvements or worsenings—were not noticed because there was insufficient contact between staff and clients or because they did not occur.
Previous work on physiological aspects of rhythmic massage therapy, a related form of external application from Anthroposophic Medicine, revealed some improvements in both short- and medium-term aspects of autonomic regulation in patients with mixed diagnoses, 10 which were accompanied by a reduction in symptoms and an increase in health-related quality of life. 11 Improvements in autonomic regulation were also observed in healthy subjects exposed to a standardized stressful situation as a result of rhythmic massage therapy. 12
Future Perspectives
Considering its simplicity and the minimal training required for effective treatment, rhythmic foot embrocation seems to offer disproportionate benefits, making it an addition to other care practices in residential facilities. In particular, rhythmic foot embrocation appears—as initially suggested by its pioneers—to stimulate recovery processes and could be used as a non-invasive approach to stress management, as a help for coping with everyday stressors and even as a contribution to increased resilience. The expected ease with which therapeutic touch could be administered in the form of foot embrocation suggests a scalable option for improving quality of life and fostering deeper, empathetic connection in care settings. However, as some of the residential staff reported difficulties related to the tight timetable for various activities of the daily routine, it appears to be important to discuss in advance in each residential facility how much time and which time slot should be reserved for rhythmic foot embrocation.
From a research perspective, the present survey points toward the need to find out more about which adults with intellectual, cognitive and/or physical disabilities would benefit most from foot embrocation. In addition, it would be interesting to find out more about the mechanisms that might be involved, for instance whether foot embrocation results in increased blood levels of endogenous oxytocin or in reduced amounts of stress hormones. Since such studies require repeated blood withdrawal, they should be restricted to persons without intellectual or cognitive disabilities. Finally, it should be considered that the impact of rhythmic foot embrocation could go far beyond the immediate physical benefits. Additional studies are needed, however, to characterize any possible long-term aspects.
Strengths and Limitations
In view of the sparse information on rhythmic foot embrocation performed on disabled people in need of support, the considerable number of participants (N = 37) in this study can be seen as a strength. A limitation of our survey is that it merely shows the reactions of the clients to the embrocation as perceived by the survey participants, that is, by the trained residential staff. The high response rate (questionnaires returned, most answers filled-in, and free-text comments) together with the very positive feedback provided by the participants is testimony of a marked need for the trained residential staff to communicate their experiences. However, only a minority of the trained residential staff could answer the questions on their patients’ autonomic regulation. 7 The results of this exploratory, descriptive analysis provide a detailed insight into the practice of and the experiences when administering foot embrocation at the participating institutions, but they cannot be generalized in the absence of a hypothesis, control group, appropriate sample design, and inferential statistics.
Conclusions
Taken together, our results show that people with various disabilities and living with assistance in residential facilities reacted well to rhythmic foot embrocation performed by trained residential staff. Given the short training time needed (two units of four lessons) and the positive reactions observed, the implementation of this therapy in residential facilities for disabled people appears feasible and highly recommendable.
Footnotes
Acknowledgments
The authors thank Ms. Ortrud Hoyer (Ekkharthof Association) for her initial motivation to run the project as well as for support and interesting discussions. The authors are indebted to all residential staff who agreed to apply foot embrocation and filled in the questionnaires, making this survey possible. Finally, the authors thank all foundations that financially contributed and thus enabled this project.
Author Disclosure Statement
A.P.S.W.; D.K. AND T.B. report financial support was provided by Dr Hauschka Foundation (Bad Boll, Germany) and all other foundation mentioned under funding. T.B. reports financial support was provided by all residential facilities mentioned in the paper. Other authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Funding Information
This project received donations from the following foundations: Dr Hauschka Foundation (Bad Boll, Germany), Foundation “Freie Gemeinschaftsbank” (Basel, Switzerland), H-M-Foundation (Pfäffikon, Switzerland), the Patients’ Organisation Anthrosana (Arlesheim, Switzerland) and the Foundation for Support of Anthroposophic Institutions (Ottikon, Gossau, Switzerland).
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3▪
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.