
Abstract
Background:
Orthopedic surgeries are of high clinical and economic importance. However, surgeries bear risks of complications and the evidence base for surgeries in orthopedics can be low. Moreover, the impact on quality of life due to an often painful and intense recovery period after surgery for the patient is not to be underestimated.
Objectives:
Integrative treatment strategies that delay or completely avoid surgical procedures can provide a valid alternative and such case reports provide practical examples.
Methods:
Different physical therapies, that is, extracorporeal shock wave therapy, cryotherapy, magnetic resonance therapy, and/or laser therapy have been combined with an oral enzyme combination (OEC) and an optimal supply of important nutrients to treat four patients with different musculoskeletal disorders.
Results:
The four patients were treated successfully with conservative holistic combination therapies and additional surgery could be avoided. The patients suffering from severe gonarthrosis and frozen shoulder experienced significant improvement of their general condition, including sleep quality, pain and mobility shortly after initiation of treatment. The patient with anterior talo-fibular ligament rupture was able to return to competition 19 days after injury and initiation of treatment. The patient with clavicular pseudarthrosis experienced almost complete mobility and freedom from pain after nine treatments.
Conclusions:
In this case series, treating patients with conservative treatment approaches led to remarkable improvements in general condition, quality of life and exercising. We conclude that conservative physical therapies, OEC and nutrients, especially when combined, are a valuable option that may prevent surgical interventions.
Introduction
In 2020, 15.8 million inpatient operations were performed in German hospitals. 1 Musculoskeletal surgeries accounted for the largest share, with a total of 4.4 million procedures, highlighting the clinical and economic impact of orthopedic interventions. Unfortunately, the evidence base for orthopedic surgeries compares unfavorably with other fields of medicine and there is also only a modest level of evidence for procedures in sports medicine, according to Lohmander and Roos. 2 Additionally, surgeries always bear risks of complications. In one of the most common orthopedic surgeries, total knee arthroplasty (e.g., due to gonarthrosis), the general complication rate in Germany in 2020 was 1.17%. 3 Although a low relative rate, with over 150,000 knee replacement surgeries in 2020, still a substantial number of patients experience complications. Moreover, the impact on quality of life due to an often painful and intense recovery period after surgery for the patient should be considered.
Therefore, conservative treatments are valid options that can delay or even avoid surgical interventions or provide an alternative approach when prior interventions have failed. Several physical therapies are well-established in orthopedics. For example, extracorporeal shock wave therapy (ESWT) has been shown to be an effective and safe therapeutic approach for different musculoskeletal disorders, such as pseudarthrosis and patellar tendinopathy. 4,5 Also, cryotherapy has long been used in orthopedics to reduce inflammation and pain as well as an aid in recovery. 6 Nuclear magnetic resonance therapy (MBST) and laser therapy are additional evidence-based and very promising options for physical therapy in orthopedics. 7,8
Besides physical therapies, an oral enzyme combination (OEC) consisting of bromelain (90 mg, adjusted to 450 FIP * units per tablet), trypsin (48 mg, 1440 FIP units or 24 μkat per tablet), and the flavonoid rutoside (100 mg per tablet) has shown favorable effects in orthopedic disorders. This fixed enzyme combination has been developed as an anti-inflammatory approach and has been explored for several indications.
In a metanalysis of six randomized controlled trials, OEC showed comparable pain reduction in knee osteoarthrosis to diclofenac, while having a superior tolerability and safety profile with a significantly lower risk of treatment-emergent adverse events, related study discontinuations, and changes in laboratory parameters. 9 Systemic anti-inflammatory effects of OEC were also demonstrated in a study on low grade inflammation in humans, where OEC significantly reduced serum interleukin-6 levels compared to placebo. 10 In a study with athletes, OEC had significant and favorable effects on fatigue, muscle soreness, and damage as well as immunological and metabolic markers after exhaustive eccentric exercise, indicating an application of OEC in supporting normal inflammatory processes for muscle recovery. 11
This case series describes the successful treatment of four patients with musculoskeletal disorders. We applied a combination of physical therapies, OEC, as well as an optimal supply of important nutrients such as vitamins, minerals and omega-3-fatty acids to maximize the body's own regenerative healing mechanisms and therefore therapeutic effect. Applied treatments are shown in Table 1. The patients' consent to a publication of their data has been given.
Conservative Combination Therapies for the Four Patients
ATFL, anterior talo-fibular ligaments; ESWT, extracorporeal shock wave therapy; MBST, magnetic resonance therapy; NHCC, neuroreflectory hyperbaric CO2 cryotherapy; OEC, oral enzyme combination.
What is already known about this topic:
- Musculoskeletal disorders like ligament ruptures chronic adhesive capsulitis are often preferably approached by surgery
- Surgery bears a risk of complications and an intense recovery period and should be delayed or even avoided if possible
What this paper adds:
- Presented cases were treated successfully with individualized conservative combination therapies
- Such approaches, tailored to the individual patient, may provide further options to be considered in delaying or even avoiding surgeries
Cases
Severe Gonarthrosis
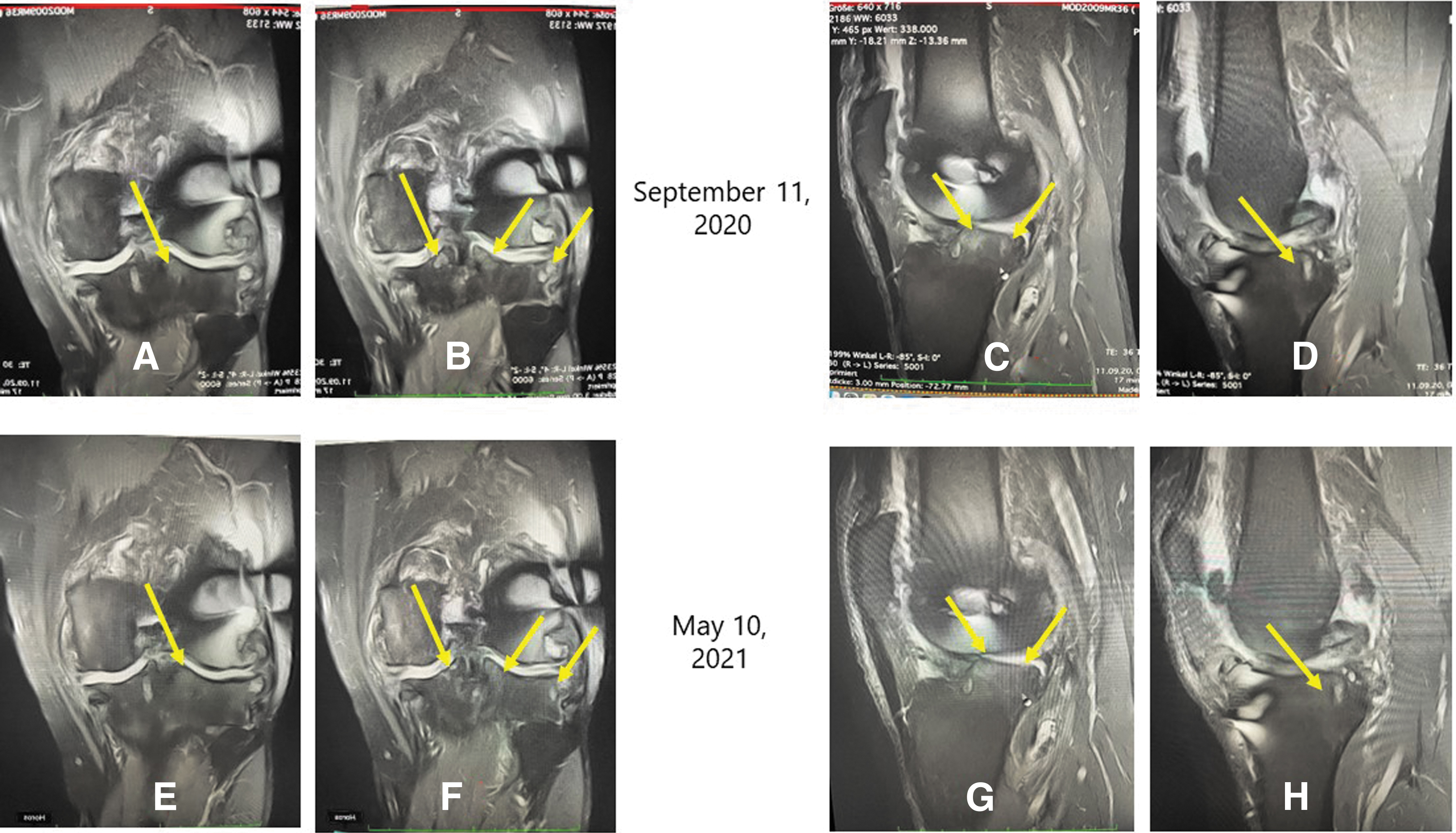
A 54-year-old male former professional soccer player presented with knee instability, exostoses, and grade 4 gonarthrosis (right knee) and grade 3 gonarthrosis (left knee) after anterior cruciate ligament (ACL) rupture of the right knee and three follow-up surgeries (ACL reconstruction and lateral and medial partial meniscus resections). Magnetic resonance imaging showed advanced activated pangonarthrosis with grade 4 chondropathy on the right, tendinopathy of the patellar tendon, joint effusion, and Baker cyst. The patient stated that he was suffering from massive pain with accompanying sleep problems, significantly limited walking distance, and limitations in recreational sports activities such as cycling. Before the patient presented to our practice, he was advised to receive a double sled prosthesis or total knee replacement.
We proposed and applied a conservative therapeutic approach with the following combination therapy: The patient received MBST once daily, as well as two hyaluronic acid injections each in the right and left knee. At treatment initiation, we applied radial ESWT and laser on both knees twice a week. In week 3, we reduced radial ESWT and laser to once a week, and finally, from week 5, to once every other week. Additionally, the patient took 4 × 3 tablets OEC daily (equals around 1.080 g (5400 FIP units) of bromelain, 0.576 g (17,280 FIP units) of trypsin and 1.200 g of rutin) from treatment initiation until week 4, and 3 × 3 tablets daily from week 5. Also, we added vitamin D3 (vegetarian) 7000 IU, vitamin K2 (all-trans menachinon-7) 200 μg, magnesium oxide 300 mg, in a combined capsule format once weekly for the first six weeks as well as undenatured collagen type II (daily dose of 1 tablet containing 40 mg) to the treatment approach.
On the fourth day after treatment initiation with MBST, laser, OEC and radial ESWT, the patient experienced significant improvement of his general condition (including sleep quality and pain) with first careful attempts at exercising on a bicycle. The patient started normal exercise load at the beginning of week 3, when he was pain free. Treatment was considered successfully finished after four months with complete disappearance of symptoms and the ability to resume an intense training workload. The patient did a transalpine crossing on his mountain bike of about 2.300 km almost six months after the treatment. Results were confirmed by MR images before and eight months after initiation of conservative combination therapy (Fig. 1).
MRI images before
Frozen Shoulder (Adhesive Capsulitis)
A 33-year-old male amateur strength athlete presented with severely limiting shoulder pain that he was suffering from since early 2018. The diagnosis at that time was acromioclavicular (AC) joint osteoarthritis. Although the patient was initially treated with cortisone injections and physiotherapy, his condition continued to deteriorate with pain throughout the shoulder and radiating along the biceps tendon in the further course. His mobility was massively restricted in all planes (abduction max. 40°). In addition, he was no longer able to work due to the pain and lack of mobility. Through a second MR image, he was diagnosed with frozen shoulder (adhesive capsulitis). Before the patient presented to our practice, he was advised to have further cortisone injections, additional oral cortisone, and surgery was suggested four weeks after starting cortisone treatment, because there was no benefit.
Our conservative approach consisted of the following therapies: we applied radial ESWT with a large 36 mm-applicator from all sides into the shoulder capsule (initially max. 1.2 bar, increase to 2.5 bar), laser, neuroreflectory hyperbaric CO2 cryotherapy (NHCC) and bioadaptive impulse therapy three times in the first 13 days, then once a week. Additionally, the patient took 4 × 3 tablets OEC daily, as well as omega-3 fatty acids (2000 mg daily) and anthocyanins in the form of wild blueberry and black currant (1 capsule daily containing 105 mg extract containing 40 mg anthocyanins each) extract.
The patient experienced significant improvements in sleep quality and mobility 13 days after the initiation of treatment. Further improvement occurred 30 days after the initiation of treatment (with a mean pressure of 2.5 bar possible), after which the patient was able to resume moderate exercising. From the seventh treatment onwards, “active ESWT” was possible, that is, ESWT during stretching of the capsule by the therapist. After eight treatments, the patient was able to resume moderate bench pressing. The treatment was continued prophylactically with radial ESWT every four to six weeks for six months at the patient's request. The patient has been completely symptom free and fully able to work and do sports again.
Rupture of Anterior Talo-Fibular Ligaments
A 26-year-old male professional soccer player presented with upper ankle distortion with complete anterior talo-fibular ligaments rupture and massive joint effusion due to an acute injury during a previous soccer game. There also was an urgent suspicion of a capsule tear. We applied an immediate conservative therapeutic intervention consisting of the following treatment regimens:
The acute treatment within one hour after the injury included laser therapy, cryotherapy (NHCC and compression), OEC (5 × 5 tablets daily), anthocyanins (wild blueberry and black currant extract, 1 capsule daily containing 105 mg extract containing 40 mg anthocyanins each), vitamin D3 (vegetarian) 4000 IU, vitamin K2 (all-trans menachinon-7) 200 μg, magnesium oxide 300 mg, in a combined capsule format once every two days. We added radial ESWT (1.5 bar, 20 Hz, 5000 ESWs) and cryotherapy (NHCC and compression) to the treatment approach 12 hours after the injury (Fig. 2). The patient was able to walk without pain 24 hours after the injury and the swelling went down almost completely. In the following days, we further treated the patient with daily radial ESWT (constant working pressure increase up to 3 bar), cold compression therapy, OEC (4 × 5 tablets daily), anthocyanins, the combination of vitamin D3, vitamin K2 and magnesium as described earlier, in addition to omega-3 fatty acids (2000 mg daily) and stabilization exercises.

Treatment of the ankle with cryotherapy and ESWT. ESWT, extracorporeal shock wave therapy.
The patient experienced a rapid increase of possible training load (also using supportive tape) and was able to return to competition 19 days after injury and initiation of treatment, completely avoiding surgery.
Clavicular Pseudarthrosis
A 26-year-old female patient, very good swimmer in all techniques, presented with a persistent pseudarthrosis of the clavicle after an accident four years ago, when she fell 4 m through a glass roof. Back then she was diagnosed with a complicated fracture of the clavicle on the right side, complete rupture of ligament structures of the right AC joint and upper ventral serial rib fracture, right side. Despite eight surgeries (four times osteosyntheses), she experienced four pseudarthroses with continued pain and feeling of pressure in the fracture area when moving and also at rest, furthermore increasing limitation of movement of the entire right arm (abduction up to a maximum of 130°, anteversion up to almost 140°), lymphedema, feeling of heaviness of the arm, and alternation between hypesthesia and hyperesthesia in the scar area. She was diagnosed with persisting pseudarthrosis in the medial third of the clavicle and complex regional pain syndrome of the right arm with significant swelling, pain and coloring.
We applied the following therapeutic intervention: radial and focused ESWT (from the second treatment already possible with 2.5 bar radial, from the third treatment additionally focused ESWT possible), laser treatment, cryotherapy (NHCC and compression), as well as OEC 3 × 3 tablets daily, vitamin D3 (vegetarian) 4000 IU, vitamin K2 (all-trans menachinon-7) 200 μg, magnesium oxide 300 mg, in a combined capsule format once every two days and anthocyanins (30 mL tart cherry juice per day, equals to 300 mg of anthocyanins). After five treatments, the patient was pain-free for the first time.
After nine treatments, the patient experienced almost complete mobility and freedom from pain even during exercises with increasing bone consolidation visible on computerized tomography (CT) scan (Fig. 3). Three months later the patient was able to swim in butterfly technique again. A remarkable result, considering no consolidation for four years.
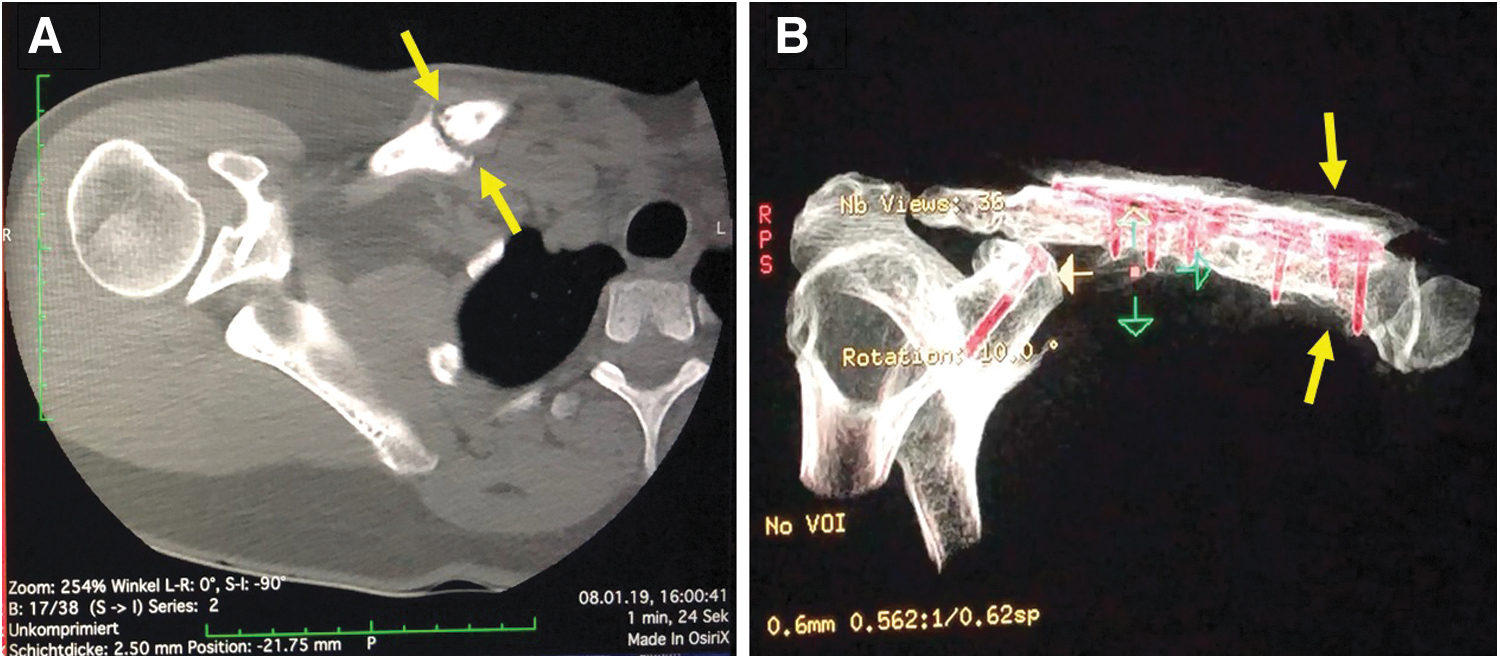
After four years of no consolidation, the patient experienced increasing bone consolidation visible on CT scan and almost complete mobility and freedom from pain.
Discussion
In this case series, the treatment of patients with conservative regenerative combination approaches consisting of oral enzymes, nutrients and individualized adapted physical therapy, for example, ESWT and cryotherapy, resulted in impressive outcomes in four patients with musculoskeletal disorders. The musculoskeletal injuries presented here are all associated with inflammatory tissue reactions that cause pain and limited range of motion which leads to poorer quality of life and in some cases, inability to work. All four presented cases (either acute or chronic conditions) were common indications for surgical intervention but have been treated successfully with individually adapted conservative approaches.
Conservative physical treatments have been shown to be effective on their own. 4 –6 The combination of multiple conservative treatment approaches, adapted to individual cases, therefore has the potential to show an even greater positive effect on healing, inflammation and recovery. For example, a recent case series showed that a combination of ESWT and NHCC is safe and effective in the treatment of painful conditions such as patellar tendinopathy and pulled muscle (M. triceps surae). 12 The application of NHCC has also recently been shown to significantly reduce CRP levels and muscle tone when used in patients after shoulder rotator cuff reconstruction surgery, stabilizing the inflammation process. 13
OEC has been reported to exhibit anti-inflammatory action similar to diclofenac in a pooled reanalysis 9 and has shown good results in another case in combination with ESWT. 14 However, the mechanism of action is not yet fully understood. Thereby it is assumed that the anti-inflammatory effects of OEC are based, among others, on its ability to decrease neutrophil migration and secretion of proinflammatory cytokines, reduction of platelet aggregation and exhibition of fibrinolytic activities. 9 Through binding to alpha-2-macroglobulin and an increase in the level of this unspecific antiprotease, the clearance of proinflammatory cytokines during inflammation is enhanced. 15 We therefore hypothesize that a combination of physical therapies and anti-inflammatory OEC acts synergistically to improve outcomes.
Besides physical therapies and OEC, nutritional status is of great importance for proper wound healing and recovery. In the case of orthopedic surgeries, it was shown that the preoperative nutritional status of patients is linked to wound healing, surgical site infections, pressure ulcers and thrombosis, and even postoperative mortality. 16 Therefore, we added nutritional supplements such as vitamin D3, vitamin K2, magnesium, cherry juice, anthocyanins, and omega-3 fatty acids to the combination of physical therapy and OEC, that is, nutrients that can positively influence inflammatory processes and bone health. 16 We thereby pursued an integrative approach that supports synergistic effects of several individual treatments with the goal of suppressing inflammation and reinforcing self-healing processes, adapted in strength and dosage to the individual patient's complaints.
Conclusions
We conclude that our combination of conservative treatments with OEC and nutrients is a valuable option for several musculoskeletal disorders that can prevent surgical interventions and also offer a promising alternative, if prior treatments have failed.
Footnotes
Acknowledgments
Medical Writing assistance was provided by Dr. Meike Janto and Dr. Michael Wördehoff, co.medical, Berlin (Germany) on the bases of the draft manuscript by the author.
Author Disclosure Statement
P.S. has received consultancy honoraria from Nestlé S.A., who additionally sponsored the article processing charges.
Funding Information
No funding was received for this article.▪