
Abstract
This systematic review primarily aims to provide a summary of the game mechanics implemented in eHealth tools supporting young people’s self-management of their chronic diseases. This review secondarily investigates the rationale for implementing game mechanics and the effects of these tools. A systematic search was conducted in Embase, Medline, PsycINFO, and Web of Science, from inception until August 30, 2022. Studies were eligible if focus was on the utilization of gamification in eHealth self-management interventions for young people (age = 10–25 years) with chronic diseases. Primary quantitative, qualitative, and mixed-method studies written in English were included. We identified 34 eHealth tools, of which 20 (59%) were gamified tools and 14 (41%) were serious games. We found that 55 unique game mechanics were implemented. The most commonly used were rewards (50%), score (44%), creative control (41%), and social interaction (32%). In comparison with gamified tools, the number and diversity of game mechanics applied were higher in serious games. For most tools (85%), a general rationale was provided for utilizing gamification, which often was to promote engaging experiences. A rationale for using specific game mechanics was less commonly provided (only for 45% of the game mechanics). The limited availability of experimental research precludes to test the effectiveness of using gamification in eHealth to support self-management in young people with chronic diseases. In this study, we highlight the importance of reporting the rationale for utilizing specific game mechanics in eHealth tools to ensure a proper alignment with evidence-based practice and the need of conducting experimental research. PROSPERO: CRD42021293037.
Introduction
Chronic diseases are health conditions that last for longer than 3 months (e.g., cancer, chronic fatigue, and depression). 1 Currently, 15%–25% of the young people (defined as 10–25 years old2–4 ) from developed countries have chronic diseases.5,6 In adolescence and young adulthood, growing up with chronic diseases impacts all developmental domains. Self-management, the process allowing young people to maintain satisfactory daily functioning despite their chronic diseases, 7 is essential for alleviating the burden of these conditions, enhancing quality of life, and reducing health care utilization.7–9 These behaviors are used to manage several aspects of chronic diseases (e.g., symptoms, treatments, and lifestyle changes). 10 Examples of self-management are decision-making, taking action, and using resources, in order to take an active role in medical management, adoption of new behaviors, and coping emotionally. 11 Currently, there is a need for novel interventions in self-management that align with the interests of young people who grow up in a digital world.12–14
For supporting chronic disease self-management needs in young people, eHealth interventions, which utilize the internet and related technologies, are promising. eHealth interventions have demonstrated efficacy in enhancing self-management. 15 Particularly, these interventions have the potential to overcome barriers to care such as anonymity and accessibility, which may reduce stigma commonly experienced by the young people, as well as reduce treatment burden in terms of time and costs. 16 Gamification is the utilization of game mechanics (e.g., badges, unlocking milestones, and narrative). 17 In this context, there are two main possibilities. First, incorporating gamification into nongame contexts in eHealth interventions, that is, gamified eHealth tools, hereinafter referred to as gamified tools. Second, designing games for a primary purpose other than pure entertainment in eHealth tools, that is, serious games for eHealth, hereinafter referred to as serious games. 18 Game mechanics align with young people’s natural interest in play, which is important for their healthy development. 19 Although incorporating game mechanics into eHealth self-management interventions for young people with chronic diseases may be a particularly promising approach, previous systematic reviews focused on adults,18,20–24 and thus, a summary of the prior available evidence in youth18,20–24 is needed. Thus, it is important to provide an overview on game mechanics used in eHealth tools for youth and the reasons to use them, which will inform the development of new eHealth tools by the eHealth Junior Consortium (see, http://ehealthjunior.nl/). This consortium develops, evaluates, and implements eHealth tools for the well-being of young people with chronic diseases.
Objectives
Therefore, the primary aim of this systematic review is to provide an overview of gamified eHealth interventions supporting young people’s self-management of chronic diseases, with an emphasis on summarizing the game mechanics implemented in the interventions. The secondary aims are (1) to identify the developer’s rationale for implementing such game mechanics and (2) to investigate the effects of these interventions. To provide a comprehensive overview of the current state of the art, we included studies conducted in young people affected with a variety of chronic diseases (e.g., somatic and psychiatric) using gamified tools or serious games.
Research questions
The primary research question is as follows: Which game mechanics have been implemented in eHealth interventions aimed to support young people in their chronic diseases self-management? In addition, the secondary research questions are as follows: (1) What was the rationale behind the implementation of each game mechanic? and, if possible, (2) What were the effects of gamified eHealth interventions on self-management and health-related outcomes?
Materials and Methods
The protocol of this systematic review was approved by the steering committee of the eHealth Junior Consortium, preregistered (PROSPERO: CRD42021293037), and published. 25 Importantly, two independent reviewers, a medical doctor (M.D.S.) and a psychologist (L.L.), were trained to participate in the key processes of the present systematic review by the guarantor of the review (F.E.L.). One of the reviewers (L.L.) was involved in the conceptualization, methodology, and development of the protocol of the review. Both independent reviewers (M.D.S. and L.L.) received explanations on the aim of systematic review, the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, protocol development, search strategy creation, screening, data extraction, quality assessment, synthesis, and reporting. They were provided with practice, feedback, and ongoing support by a highly multidisciplinary team including experts in systematic reviews, pediatrics, psychology, and psychiatry and game experts/designers. This support was particularly intense at the beginning of the training, including pilot testing and detailed consensus meetings to address discrepancies. Consensus meetings to address discrepancies were regularly arranged throughout the review process.
Inclusion criteria
Participants: Adolescents or young adults (between ages 10 and 25 years) with a chronic disease.
Interventions: Gamified eHealth tools or serious games for eHealth tools aiding self-management in young people with a chronic disease. Self-management behaviors are aimed at managing the disease and its effects (e.g., symptoms, treatment, physical and psychosocial consequences, and lifestyle adjustments). 10 An intervention was considered intended for self-management if it addresses at least one of the following behaviors: problem solving, decision making, using resources, forming a relationship with a provider, or taking action,26,27 performed in the domains of medical management, adopting new behaviors or roles, or psychosocial coping. 27
Comparator: For studies that included a comparison arm, we compared gamified interventions or serious games versus (1) usual care (comparator) or (2) nongamified (comparator) versions of eHealth interventions.
Outcome measures: To assess the effects of the interventions, we focused on three categories of outcomes: (1) self-management behaviors including problem solving, decision making, using resources, and forming a relationship with a provider and taking action 26 ; (2) effects of self-management on outcomes27,28; and (3) antecedents of self-management such as adherence to the eHealth tool, acceptability, and user’s experience.27,28
Studies: We included peer-reviewed articles and conference proceedings reporting primary data.
Search strategy
On August 30, 2022, we conducted an electronic search in Embase, Medline, PsycINFO Ovid, and Web of Science Core Collection. We used these databases because the topic of our review is at the intersection of biomedicine and psychology fields. Supplementary File S1 shows the search strategy. In brief, an experienced information specialist (W.M.B.) designed a search consisting of terms (both controlled thesaurus terms and terms in title or abstract) for chronic diseases such as asthma or diabetes, combined with gamification, eHealth or mobile phone applications, and self-care or coping behavior and limited to youth or adolescents. The search results were limited to articles in the English language only. To identify gray literature, the eHealth Junior Consortium members were emailed for unpublished eligible studies. To gain deeper insights in the tools identified from the included studies, we conducted a snowballing technique (using references and cites of the included studies) and a Google search (e.g., trailers and intervention websites).
Selection of studies
Metadata were imported into Mendeley Desktop, and duplicates were automatically deleted. Two researchers (M.D.S. and L.L.) independently screened records by title and abstract and then by full text for inclusion. Disagreements were resolved through discussion with a third researcher (F.E.L.).
Data extraction
The information to describe each of the eligible studies was extracted (1) by two researchers independently when presented in the main text (M.D.S. and L.L., or M.D.S. and M.M.H.; disagreements were resolved through discussion with a third researcher [F.E.L.]) or (2) by one researcher only when presented in supplementary files (M.D.S., who consulted with other researchers when needed). To guide the extraction of the game mechanics implemented in each eligible study, we used the framework of game design patterns by Björk and Holopainen 29 because it offers a comprehensive overview and description of game mechanics, including detailed definitions and examples. Thus, this framework was instrumental in guiding data extraction for the present review. Brief definitions of each game mechanic are provided in Supplementary File S2; for further details, readers are directed to the original source. 29 We carefully considered other frameworks, but we found that they were not adequate for this review because they focus on nonserious games, 30 the educational domain specifically 31 or broad groups of game elements, 32 or general drivers for engagement. 33 The rationale was extracted literally from the included study (see Supplementary File S3).
Risk of bias (quality) assessment
The Mixed-Methods Appraisal Tool 34 was used to assess the risk of bias of each eligible study (M.D.S. or L.L., who consulted with other researchers when needed).
Funding information
In line with the PRISMA statement, which advocates for transparent reporting and comprehensive documentation of the review process, we extracted the funding information from the included studies (M.D.S. or L.L., who consulted with other researchers when needed). This addition ensures transparency regarding potential additional sources of bias or conflict of interest in the included studies.
Data synthesis
A narrative (descriptive) synthesis was provided for the primary and secondary review questions. Gephi Graph Visualization and Manipulation software version 0.10 was used to create a network of game mechanics.
Results
Selection process
From 2357 records identified in the primary search, we included 34 studies.35–64,72–76 Using a snowballing technique, we included seven additional studies65–71 (Fig. 1 for flowchart). From the 41 studies included in this review, 34 unique eHealth tools with gamification were identified. The main characteristics of these tools are summarized in Table 1. Of the 41 studies, 24 focused on developing tools or investigating their usability/feasibility36,39,41–47,49,51,53,58–62,64–67,69,72,73, 15 on testing the effects of the interventions (eight were randomized controlled trials [RCTs]37,40,48,50,54,56,70,71, two were protocols for RCTs57,74, four had a pre-post design38,52,55,75 and one had a single case experimental design [SCED 63 ] and two were descriptives35,68). The quality assessment revealed that the different components within the mixed-method studies did not meet the quality criteria for each respective method, and none of the quantitative nonrandomized controlled trials adequately addressed confounders in design and analysis (see Supplementary File S4). A summary of the funding information from the included studies is presented in Supplementary File S5. When needed, a complementary Google search (e.g., trailers and intervention websites) was conducted to obtain additional information (see Supplementary File S6).
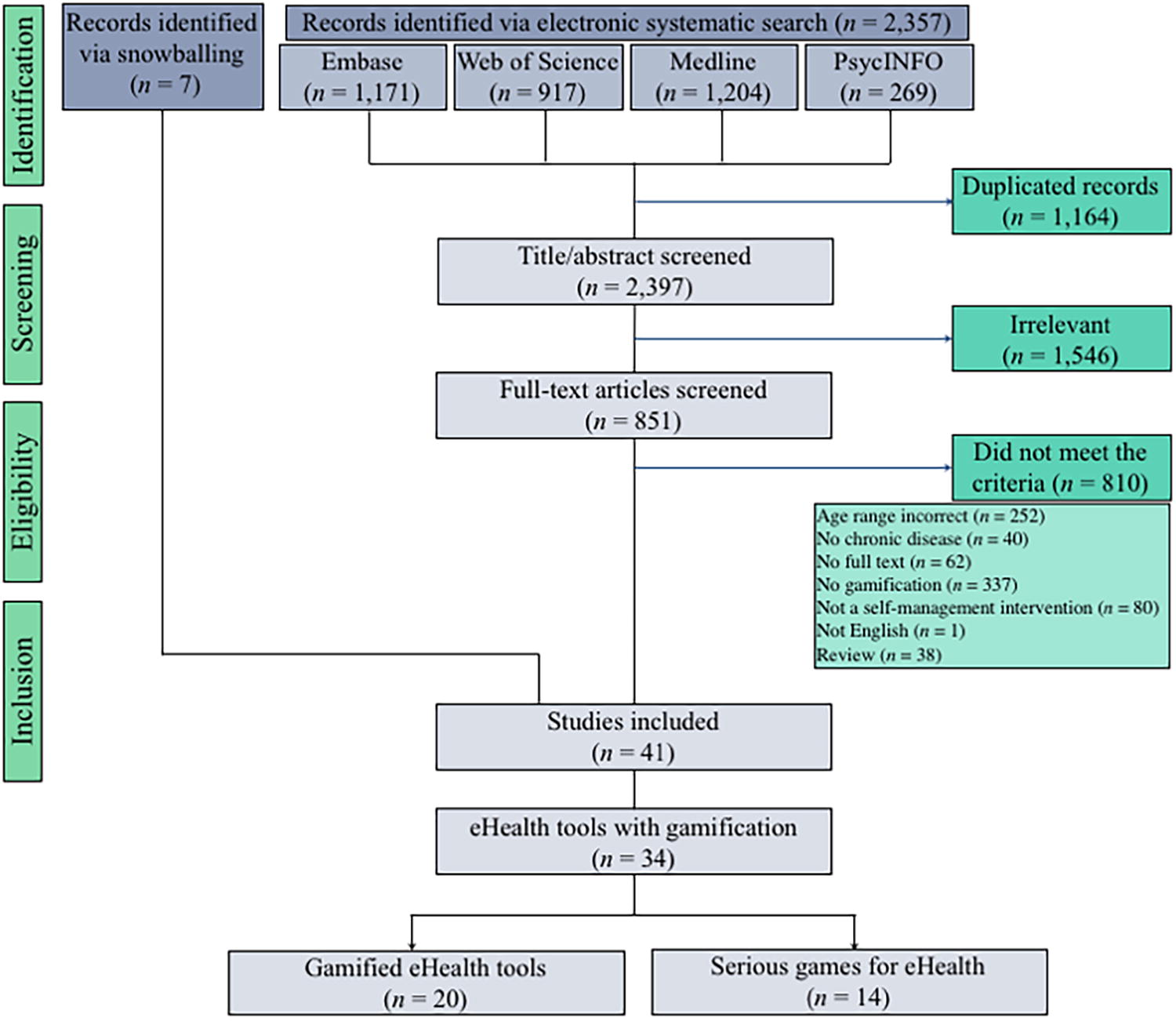
Flowchart of the selection process.
Overview of the eHealth Tools Identified from the Included Studies
Note. *As some tools were described and evaluated in multiple studies (with different designs) and some studies described multiple tools, the number of supporting references does not always match the frequency of tools with specific characteristics.
The type and platform of one tool were unclear. 35
Characteristics of eHealth tools
Regarding the type of gamification, 20 tools were gamified36,37,39,41,44–47,50,53–56,58,59,61,62,64–67,69,72–75 and 14 tools were serious games.35,38,40,42,43,48,49,51,52,57,60,63,68,70,71 Tools were developed for a broad range of chronic diseases, including somatic,35,36,38,39,41,43–46,49–58,60–62,65,67,69,72–75 psychiatric,40,42,47,48,63,64,66,68,70,71 and those at the intersection of both (i.e., chronic pain).37,59
Most tools (n = 26) aimed at multiple self-management domains and behaviors.36–42,44–51,53–56,58,59,61–73 Twenty-nine tools supported taking action,36–47,49–51,53–56,58–64,66,67,69,71–74 such as taking medication44,49,60,73 or increasing physical activity.36,48,50 Using resources was targeted in 27 tools,36–39,41–55,59,61,63,64,66,68–75 for example, through monitoring disease activity or self-management behaviors.37,44–46,56,59,61,62,65,72,73 Ten tools supported forming a relationship with a provider39,45,46,50,51,54,55,59,64-66,69,72,74 and decision making, respectively.36,39,42,46,51,53,56,58,59,62,65,67,73 Only the anorexia nervosa companionship app targeted problem solving directly, with a module on how to manage emotional dysregulation. 47
Implemented game mechanics (primary research question)
We identified 55 distinct game mechanics; Figure 2 presents an overview. The most commonly used were rewards (n = 17 [50%]), score (n = 15 [44%]), creative control (n = 14 [41%]), and social interaction (n = 11 [32%]). In comparison with gamified tools, the number and diversity of game mechanics applied were higher in serious games (Fig. 3). A small group of game mechanics was combined in several tools; for example, 11 tools combined rewards and score (Fig. 4, see Supplementary File S7 for the more detailed figure41,43–46,51,53,55,56,60–62,69). Of the 55 distinct game mechanics, 51 were used in serious games compared with 27 in gamified tools, of which 23 were found in both.
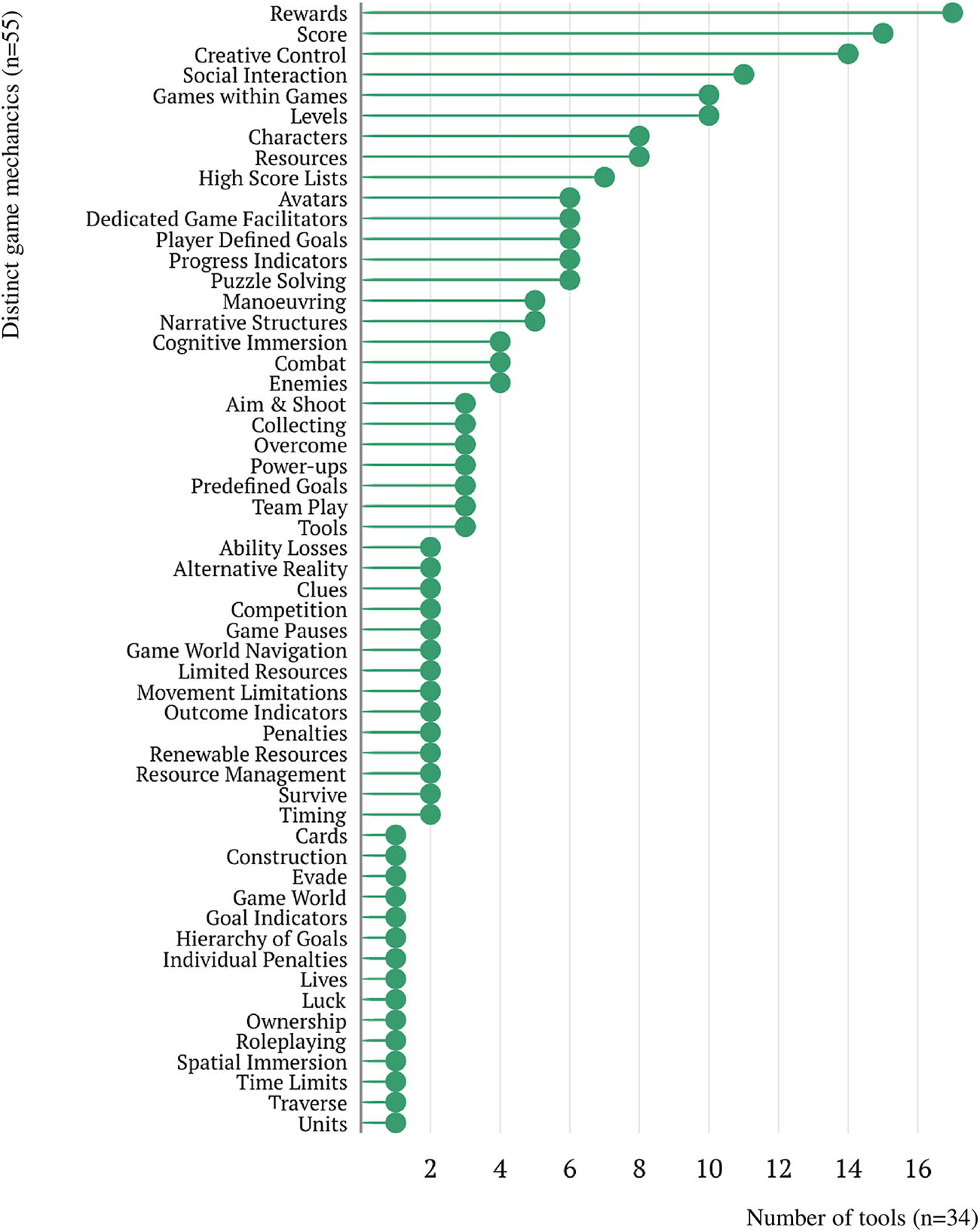
Number of tools using specific game mechanics. The total number of tools and distinct game mechanics is included between brackets.
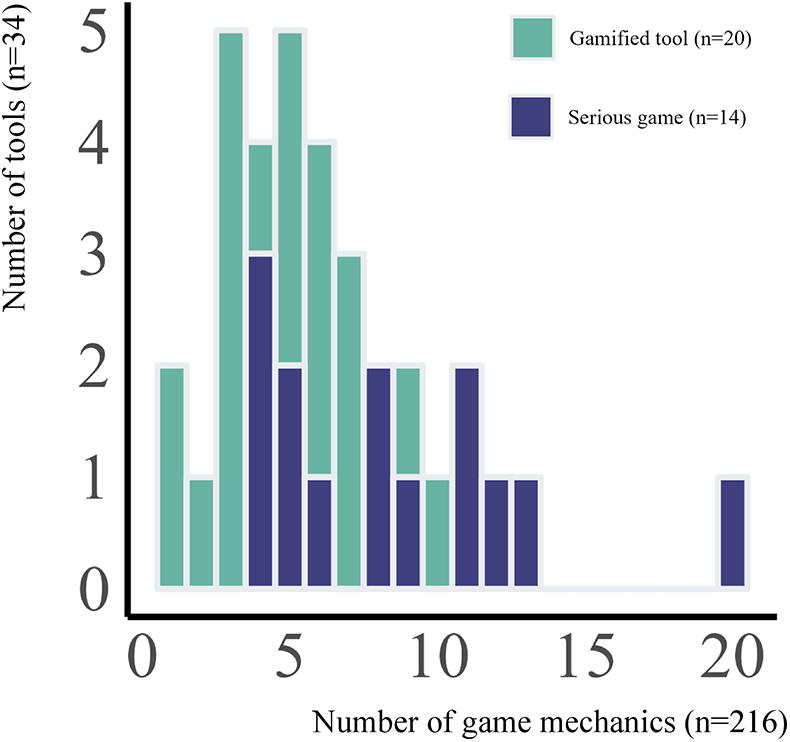
Number of game mechanics implemented per tool. The total number of tools per category is included between brackets. The median number (range) of game mechanics implemented per tool for gamified tools was 5 (1–10) and for serious games was 8 (4–20).
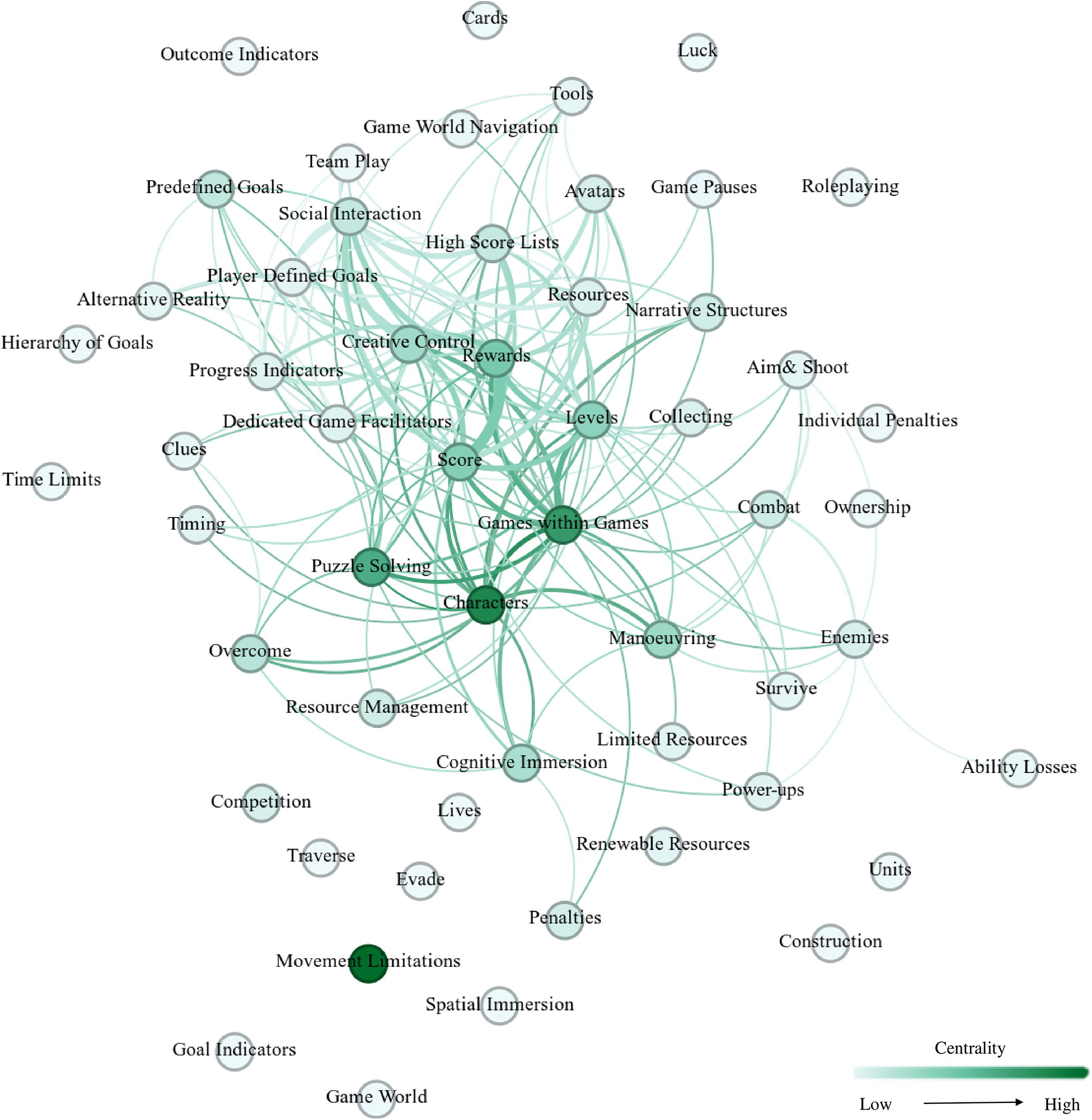
Combinations of game mechanics. All nodes represent a game mechanic (see label). Links between nodes represent common use in a tool. The thickness of the links represents the frequency of co-occurrence (the thicker the link, the more often the connected game mechanics are used in the same tool). For readability, we chose to filter out links with a weight of only 1 (see Supplementary File S7 for the unfiltered network). The color of the node reflects betweenness centrality (the frequency of the node being on the shortest path between other nodes; the darker the node, the larger the dependency of other nodes). The high betweenness centrality of some game mechanics (e.g., Games within Games, Puzzle Solving, and Characters) reflects their frequent use in serious games, causing co-occurrence in tools with a large variety of other rare game mechanics (e.g., Lives, Evade, and Units). This is contrasted by the relatively low betweenness centrality of the common game mechanics Rewards and Social Interaction, illustrating their main occurrence in gamified tools.
Rationale for gamification (secondary research question)
A rationale for implementing gamification in general was provided for 29 eHealth tools (85%, Table 2 depicts an overview, whereas Supplementary File S3 contains detailed information). The most common rationale for gamification was promoting engagement,37,38,40,41,44,45,47,49,55,57,59,62–64,67,68,72,75 behavioral change,43,46,47,60,64,68,75 and effectiveness.40,43,55,60,68,71 For serious games in specific, authors saw games as an effective tool to learn,35,38,42,48,60,68,70,71,76, specifying special needs of children with specific psychiatric diseases42,63 and explaining the preference for game-based learning by the young age of the users. 38 Moreover, in rationales within serious games, the young age was brought into connection with their interest in games 63 and technology 60 in general. 38 Games are tailored to the special needs of children with diseases42,63 and intellectual and social maturation levels. 38 A rationale to use a specific game mechanic was provided for 97 instances (45%, Table 3). Most of these rationales were directly related to increasing engagement with the tool or the targeted self-management behavior. Although for more than half of the tools, the design of the self-management intervention was based on a behavioral change,36,39,44,46,50,51,54,58,60,61,65,67 learning theory,40,52,63 or a psychological therapy,40,42,47,48,68,70,71 only seven tools36,40,46,48,50,51,58,67,68,70 directly linked the implementation of specific game mechanics to this theoretical basis. For instance, ATOMIC, 36 COOL Passport, 50 and Reactivate 46 were based on the social cognitive theory. 77 Consequently, they used game mechanics that were largely similar. However, how the mechanics were linked to theory constructs differed; for example, social interaction was used in all three tools but for different reasons: for self-efficacy and outcome expectations, 36 social support,36,46 or self-judgment. 50
eHealth Tools with Gamification for Chronic Disease Self-Management in Youth and Their Rationale
Additional information on implemented game mechanics was found with Google search for the following tools: L’Affaire Birman, MyREADY Transition BBD, and Pain Squat+ (S6). CF, cystic fibrosis; DM1, diabetes mellitus type 1.
Rationale for the Use of Specific Game Mechanics
Rationales are summarised. For detailed rationales extracted directly from the included studies, see Supplementary File S3.
Importantly, involving patients in codesign processes yielded rationales for implementing certain game mechanics, as these were most appealing to the target population.41,50,59,61,65 In serious games, a broad range of game mechanics facilitated the practice of self-management skills. For this rationale, FUN QUEST, among others, included characters, avatars, roleplaying, and narrative structures. 38
Efficacy of gamification and serious games (secondary research question)
We did not perform meta-analyses because only eight RCTs were included and primary outcomes and control conditions were diverse (Supplementary File S8). There was no effect observed in six (75%) RCTs37,50,54,56,70,71 and positive effects in two RCTs, both testing a serious game.40,48 A consistent finding across studies with and without control groups was that higher engagement was associated with larger effect sizes.37,39,55,56,64 Studies gave little insight on mediators for engagement. The effect of gamification in general could only be deduced from the study on TEENCOPE, which was compared with a nongamified eHealth intervention and did not perform better in engaging. 54 The effect of specific game mechanics on engagement or other outcomes was not assessed in any of the included studies.
Discussion
In this systematic review, we observed that 55 distinct game mechanics were implemented in 34 eHealth tools. The most used were rewards, score, creative control, and social interaction. We also showed that the most common rationale for gamifying eHealth tools was to provide young people with an engaging experience. Experimental research is scarce, precluding to quantify the effects of gamified eHealth interventions in improving young people’s self-management of chronic diseases.
Implemented game mechanics (primary research question)
A total of 55 distinct game mechanics were implemented in the included studies, 216 times in total altogether. Rewards, score, and social interaction were frequently used. A previous review also identified these game mechanics as common in eHealth tools for medical education. 24 The common use of the same game mechanics in diverse populations, with different characteristics and needs, may raise concerns, 78 particularly in relation to effectiveness and integration.79,80 Tailoring the game mechanics in eHealth tools to support self-management, considering the age and specific needs associated with a particular chronic disease, may be important for optimal outcomes.79–81 However, the present review does not allow us to determine which specific combination of game mechanics may best suit a particular disease, as the studies included involved a wide range of diseases.
From the 34 eHealth tools included in this review, 20 (59%) were gamified and 14 (41%) were serious games. Of the 55 game mechanics implemented, 4 were unique in gamified tools, 28 in serious games, and 23 were utilized in both types of tools. In general, the level of gamification (i.e., the number and diversity of implemented game mechanics) was higher in serious games in comparison with gamified tools. In line with prior literature, 24 the use of gamification for self-management purposes may have been insufficient in certain gamified eHealth tools, as it was solely based on point or reward systems.37,61 However, other gamified eHealth tools integrated point or reward systems with additional mechanics such as creative control36,39,44,47,55,59,65,69 or social interaction.36,39,45,46,50,55,56,59,62,65,69 While these types of gamified tools may be more effective, the current state of the art does not provide firm conclusions. The lack of concrete insights might be explained by the paucity of efficacy studies. In addition, RCTs have been suggested to be unappropriated to assess complex interventions like mHealth. 82 For gaining insight into the working mechanism of game mechanics, more adaptive study designs might be a solution. Examples are a SCED 83 (n = 1, 1 study found in this review 63 ) and a multiphase optimization strategy trial, which allows for testing individual intervention components and their combinations. 84 Even with these adaptive designs, it needs to be considered that a game mechanic is not a sole entity and depends on its integration in the tool and combination with other mechanics.
Rationale for gamification (secondary research question)
One of the secondary aims of this review was to identify the rationale for gamification in self-management facilitated by eHealth. This aim was conducted at two levels: the general rationale for using gamification in eHealth tools and the rationale for implementing a specific game mechanic. We found that providing a general rationale for using gamification or serious games was more common than for a specific game mechanic; 85% of the tools versus 45% of the times. The rationale most frequently given for both implementing game mechanics in general and for the choice of specific game mechanics was to provide young people with an engaging experience,37,38,40,41,44,45,47,49,55,57,59,62–64,67,68,75 which was robustly observed from previous reviews without age restrictions on eHealth interventions for mental health and well-being 18 and chronic disease management and healthy lifestyle. 23 Collectively, for young people, incorporating game mechanics into eHealth self-management interventions seems appropriate because of their natural interest in play, which was reflected by the rationales for serious games. 19
In some studies included in the present review, it was highlighted that involving young people with chronic diseases in codesign when gamifying eHealth tools for self-management may help to identify which game mechanics are the most appealing to the target population.41,50,59,61,65 However, this speculation remains to be corroborated in experimental research. 85 Indeed, a previous review concluded that gamification in mental health apps lacked a clear rationale. 22 We additionally showed that the link between specific game mechanics and self-management theory was not explicitly stated for most of the tools included in the present review. Thus, on behalf of the eHealth Junior Consortium, we recommend that future research reports the rationale for utilizing specific game mechanics in eHealth tools to ensure a proper alignment with evidence-based practice, which is highly valued in healthcare. 80
Efficacy of gamification and serious games (secondary research question)
In this study, we found that experimental designs (i.e., RCT and SCED) were scarce and heterogeneous. This limitation does not seem to be specific to research on eHealth or young people, as it has also been observed in other reviews that do not focus on eHealth and do not have age restrictions.86–89 In general, the limited experimental evidence makes it difficult to quantify the effects of gamification in the self-management of chronic diseases in young people. Only two (25%) of the eight RCTs included in this review showed that eHealth interventions utilizing gamification may improve self-management of chronic diseases. Consistent with previous reviews,86,89,90 the studies that we included had small sample sizes and may have been underpowered. Consequently, it is challenging to draw quantitative conclusions from our review. Thus, future studies should be well-powered. In our risk of bias (quality) assessment, we also identified that future nonexperimental research should adequately control for confounders as is a common limitation in the available literature.
Limitations and strengths
This review has some limitations. First, the small number of RCTs included in this review precluded to conduct meta-analysis to quantify the effects of eHealth interventions using gamification. At least, we provided a qualitative synthesis, which was not conducted by previous reviews on different populations. 24 Second, the inclusion of studies published in English only may limit the generalizability of our results. Third, the rapidly evolving nature of eHealth terminology may have resulted in failing to identify relevant studies despite our carefully designed search term combinations. Fourth, common limitations in the field, such as incomplete descriptions of eHealth tools, may have negatively impacted our findings. Fifth, a deeper level of understanding on how specific game mechanics were used to engage users may be of interest, 91 which would require to conduct qualitative studies in the targeted population. Sixth, we paid scarce attention to how well several game mechanics were integrated in each of the tools and if they aligned with the therapeutic goal(s) of the tools, which might impact the efficacy of game mechanics.80,92
This review also has several strengths. First, the inclusion of heterogeneous samples and interventions, such as somatic and psychiatric diseases, as well as gamified tools and serious games, helped us to provide a comprehensive overview of the current state of the art. Our comprehensive overview may serve as a valuable resource for game developers, health professionals, and researchers offering starting points for further development and evaluation of gamified eHealth interventions. A priority of the eHealth Junior Consortium for further research is to identify both universal/transdiagnostic and individual/personal mechanisms promoting self-management acknowledging the importance of both types of mechanisms. Second, we carefully designed our search strategy, inclusion/exclusion criteria, and time span coverage, searching in four major databases (Embase, Medline, PsycINFO, and Web of Science). In addition, two independent researchers were involved in all the information provided in the main text of this review (e.g., electronic search, selection of studies, and extraction of information for main tables and figures). Third, this work is embedded within the eHealth Junior Consortium, providing a highly multidisciplinary vision from diverse fields including pediatrics, psychiatry, psychology, game design, and eHealth, among others.
Conclusions
This review provides an overview of the use of game mechanics in eHealth tools focusing on improving self-management of chronic diseases in youth. We identified 34 eHealth tools utilizing 55 distinct game mechanics; the most common were rewards, score, creative control, and social interaction. For most of the tools (85%), a general rationale for utilizing gamification was provided, which often was to facilitate engaging experiences. A rationale for using specific game mechanics was less commonly provided (only for 45% of the game mechanics). Thus, future research should report the rationale for utilizing specific game mechanics in eHealth tools. The scarce experimental research available precludes testing the effectiveness of using gamification in the eHealth tools identified in the present review. The general rationale for gamifying and the rationale for using specific game mechanics identified in this review may inform priorities for testing their effectiveness in future experimental research.
Footnotes
Acknowledgments
The protocol of the present systematic review was agreed in an online meeting of the eHealth Junior Consortium on 9/11/2021. Discussions about the findings were carried out in online meetings on 14/07/2022 and 19/01/2023. The authors thank all the participants for their active participation and valuable suggestions.
Authors’ Contributions
M.D.S.: search, study selection, data extraction, writing, visualization, and project administration. L.L.: conceptualization, methodology, search, study selection, data extraction, and writing. M.M.H.: conceptualization, data extraction, and review. J.v’t.V.: conceptualization and review. V.T.V.: conceptualization and review. W.M.B.: conceptualization, methodology, and review. M.H.J.H.: conceptualization, review, and project administration. R.C.V.: conceptualization and review. S.L.N.: conceptualization, review, and project administration. F.E.-L.: conceptualization, methodology, writing, supervision, and project administration. F.E.-L. is the guarantor of the review.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This publication is part of the “Feeling good, despite illness; Accessible eHealth supporting the well-being of chronically ill children.” The eHealth Junior Consortium project (with project number
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.