
Abstract
Introduction:
Revision rhinoplasty typically requires cartilage grafting to improve both functional and aesthetic results. 1 Septal cartilage, which is preferred in rhinoplasty due to its location, structure, and abundance, may not be an available option in revision surgery. 2 This leaves several viable grafting alternatives including costal and auricular cartilage. Rib cartilage provides a large volume of material but requires a second operative field and exposes the patient to greater morbidity and complications, such as chest wall infection, hematoma, and pneumothorax. 3 Auricular cartilage harvesting is a simple and underutilized technique in nasal reconstruction. 1 Compared with rib cartilage, ear cartilage harvesting has lower morbidity, is faster, and less technically complicated. This technique can preserve normal ear contours, has low complication rates, and is well suited for creating a variety of grafts. 2,4 The goal for this approach is to obtain cartilage with sufficient width and length for rhinoplasty procedures while preserving the natural contours of the ear. In this video, we review the advantages and indications for auricular cartilage harvest and explain a postauricular conchal cartilage harvest technique.
Materials and Methods:
A patient presented to clinic after a prior aggressive reductive rhinoplasty. Examination revealed tip ptosis and severely collapsed lateral crura. There was a deficiency of septal cartilage. Options including reconstruction with auricular cartilage versus rib grafting were discussed. After reviewing the risks and benefits, informed consent for an approach using auricular cartilage was provided.
Results:
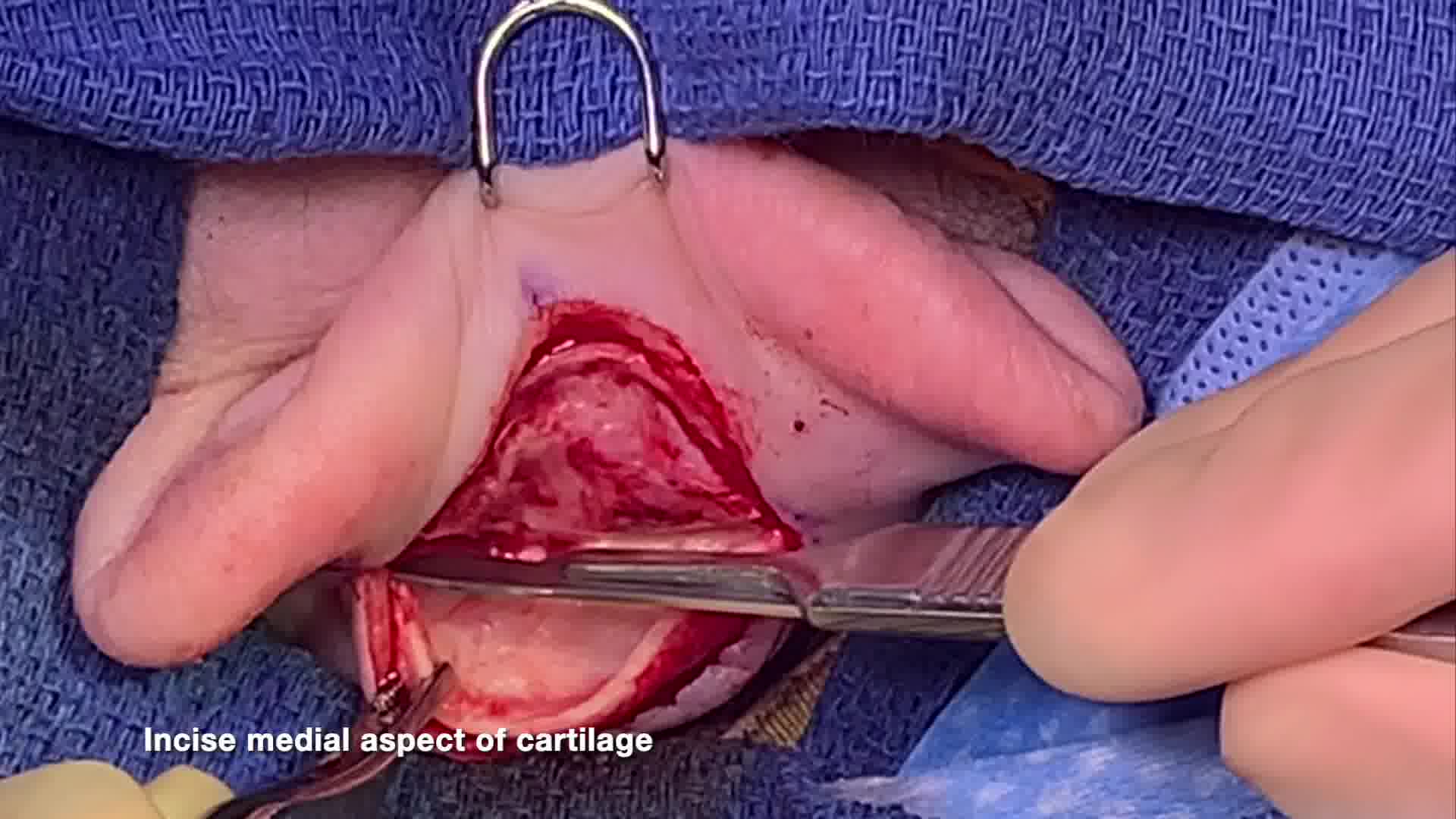
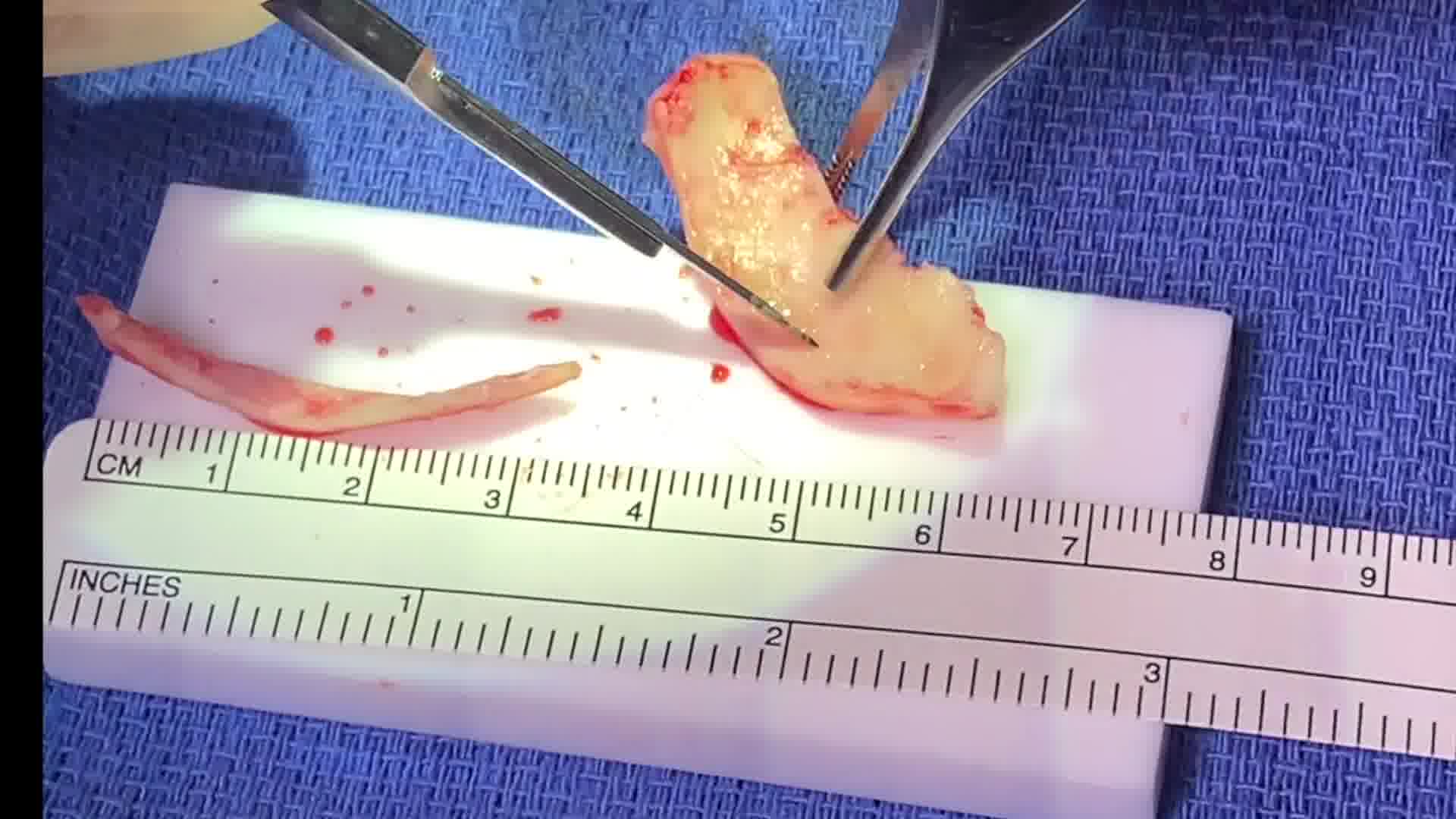
Auricular cartilage was systematically harvested and used to create effective rhinoplasty grafts. After marking the skin to preserve auricular contours, a posterior incision was made by simultaneously incising both skin and cartilage. Tissue was dissected free from the conchal bowl cartilage. Dissection can proceed as far superiorly to the concha cymba, over the helical root, and as far inferiorly along the concha cavum toward the external auditory canal. A medial transcartilaginous incision was made. This is typically created as far medially as necessary for the planned cartilage grafts. The posterior incision is closed with running 5-0 chromic sutures. Anterior and posterior compressive bolsters are made from cotton dental rolls. With preservation of the antihelical contours and placement of the incision posteriorly, the ear typically heals with virtually no long-term negative aesthetic consequences. The auricular cartilage was used to create bilateral spreader grafts, bilateral articulated alar rim grafts, bilateral caudal septal extension grafts, and a large shield graft. Careful carving and shaping of the grafts to fit the needs of the reconstruction are performed. By using a cutting technique that utilizes the outer perimeter of the conchal cartilage, a graft of up to 4.5 cm in length can be obtained. The patient healed with an excellent functional and aesthetic result.
Conclusions:
Ear cartilage harvest is simple, efficient, and effective for rhinoplasty and nasal reconstruction. This technique offers a viable alternative to rib cartilage harvesting. We favor a postauricular approach with attention to preserving the anterior auricular contours and an effective bolster dressing. There are minimal long-term functional and aesthetic consequences.
Dr. Ostrander contributed to formal analysis, methodology, project administration, resources, validation, visualization, and writing (original draft, review, and editing). Dr. Watson contributed to conceptualization, data curation, formal analysis, investigation, methodology, project administration, resources, supervision, validation, visualization, and writing (original draft, review and editing). Dr. Watson was responsible for the conceptualization of the surgical technique and she had a major role in the original draft.
The authors have no competing financial or ethical conflicts of interest to disclose. The patient provided informed consent before the procedure, and no identifying information has been included to ensure absolute anonymity. This study was performed in accordance with the Declaration of Helsinki. No experimental or investigational treatments were administered, and the single patient featured received standard of care treatment.
No funding was received for this article.
Runtime of video: 6 mins 46 secs
Get full access to this article
View all access options for this article.