
Abstract
Background:
Encouraging adolescents to adopt healthy lifestyles can be challenging. The aim of the “Som la Pera” study was to engage adolescents by applying new strategies to increase both their fruit and vegetable consumption and their physical activity (PA), while reducing their sedentary behavior (screen time per day).
Methods:
In disadvantaged neighborhoods of Reus (Spain), two high schools were randomly assigned to the intervention (n = 169 adolescents, 13- to 16-year old) and two were assigned to the control group (n = 223 adolescents, 13- to 16-year old). The intervention, which lasted 12 months and spanned two academic years (2013–2015), used social marketing (SM) to improve healthy choices. The peer-led strategy involved 5 adolescents, who designed and implemented 10 activities as challenges for their 169 school-aged peers. The control group received no intervention. To assess self-reported lifestyles in both groups, the Health Behavior in School-aged Children survey was used at baseline and end of study.
Results:
After 12 months, the weekly PA improved in the intervention group vs. the control one (p = 0.047). When male and female groups were examined separately, the improvement in PA remained with a borderline significance only in the male group (p = 0.050).
Conclusions:
A school-based, peer-led SM intervention designed and implemented by adolescents attending high schools in low-income neighborhoods promoted an increase in PA, particularly in male adolescents 13 to 16 years of age. No effect on fruit or vegetable consumption or screen time was observed.
Clinical Trial Registration number: NCT02157402.
Background
Adolescent obesity is a public health concern. In Europe, one of three 11-year-old children is overweight or obese. 1 In Spain, up to 26% of 13-year-old males and 18% of 13-year-old females were overweight or obese in 2014. 2 This fact needs compelling solutions considering that adolescent obesity is a strong predictor of adult obesity, which has many well-known short- and long-term health and economic consequences, both for the individual and society as a whole. 3
Adolescents are considered vulnerable to their neighborhood environments. Several studies in American populations show that adolescents from high-income countries living in low-income neighborhoods are at a higher risk of obesity. 4 Moreover, obesity persistence is strongly associated with the transition to adulthood across socioeconomic status (SES) categories. 5 Some environmental factors and behaviors may explain this association. For instance, in recent decades, European adolescents categorized with a low SES have shown decreased physical activity (PA), and increased time spent on video gaming, increased unhealthy dietary lifestyles, and decreased breakfast consumption. 6 Understanding youth obesity and its modifiable risk factors is a key point for addressing obesity occurrence, particularly in adolescents living in disadvantaged neighborhoods.
As adolescents grow up, an identity-reshaping process of establishing relationships with friends, family, and society occurs. 7 Due to this, they are less subjected to parental advice and more to peer and media influences, 8 while simultaneously being an influence over their peers' healthy choices and behaviors.9,10 This influence on the peers can be used in peer-led education, which is defined as “a strategy that involves teaching or sharing health information, values, and behaviors among individuals as part of normal communication within similar social groups.” 11 Peer-led strategies applied in interventions have been shown to be effective in preventing tobacco, alcohol, and cannabis use among adolescents. 12
Disparate results have been obtained in healthy lifestyle interventions. The Healthy Buddies study 13 was a 10-month intervention, focused on promoting healthy lifestyles, implemented by older adolescents (4th school grade in the US Education System) to younger (kindergarten) schoolchildren. Results showed an improvement of the health knowledge, attitudes, and behaviors in both populations. 13 The TEENS study 14 was a 2-year intervention implemented by youth on their classroom peers to promote healthy eating. Although the TEENS intervention was widely accepted by the youth involved, no improvement in healthy eating was observed.
Social marketing (SM) is a change strategy that applies commercial marketing principles in health promotion programs to influence voluntary behavior toward systematically making healthy choices. 15 SM can increase the quality and effectiveness of school-based interventions aimed at improving healthy habits. However, more scientific evidence is needed because few interventions have expressly used SM as a methodological strategy in youth obesity prevention. 16
The European Youth Tackling Obesity (EYTO) project was developed as a multicenter, peer-led SM intervention aimed at improving adolescent lifestyles by encouraging healthy choices, such as making healthy dietary choices and increasing PA. EYTO long-term goal is to prevent obesity in adolescents from socioeconomically disadvantaged neighborhoods in United Kingdom, Spain, Portugal, and the Czech Republic. 17 This project recruited and engaged five adolescents per country to work as adolescent challenge creators (ACCs), who then designed and implemented a peer-led intervention for their classmates using SM benchmark criteria (SMBC) as the methodological basis. The SMBC help strengthen the use of effective SM strategies and include the following 8 domains: customer or participant orientation, behavior, theory, insight, exchange, competition, segmentation, and the methods mix. 17 The teams in each country acted autonomously, and in Spain, the project consisted of a school-based intervention called “Som la Pera” (“We are Cool”).
This work is focused on several potential contributors for obesity development. The main aim is to assess the effectiveness of the “Som la Pera” intervention, a school-based, SM, and peer-led methodology, in promoting an increase in PA and fruit and vegetable consumption, while reducing screen time in adolescents. The secondary aims are to evaluate the change in adolescents' breakfast consumption, to reduce obesity prevalence, and to evaluate the engagement of local organizations and stakeholders in the Project.
Methods
The original protocol has been previously published. 17 The study was approved by the Ethics Committee of the Hospital Universitari Sant Joan de Reus (ref: 14–04– 24/4proj2) and registered at clinicaltrials.gov (NCT02157402). The protocol followed the principles of the Helsinki Declaration and the good clinical practice guidelines of the International Conference on Harmonization (ICH GCP). The study was reported in accordance with the CONSORT 2010 extension to cluster randomized trials 18 (Supplementary Data).
Data from this study were published in Aceves-Martins et al. 19 On March 6, 2020, concerns were raised regarding ignoring clustering and nesting in the statistical analyses. Afterward, a retraction of the article was made, but we were given the opportunity to perform a new version of the article by re-analyzing the data taking in to account clustering and nesting in the statistical analyses.19–22 Thus, this article is a republication of the original (retracted) article addressing concerns raised by Golzarri-Arroyo et al. 20
Study Design
The “Som la Pera” intervention was a parallel-cluster randomized controlled study performed in Reus, Catalonia, Spain. The study focused on promoting healthy lifestyle changes in adolescents. To minimize contamination between research conditions, high schools were the unit of randomization, with an allocation ratio of 1:1. Local authorities identified nine public high schools serving socioeconomically disadvantaged neighborhoods. The randomization code was computer generated, and the high schools were assigned to either the control or the intervention arm using the PROC PLAN in SAS 9.2 (SAS Institute, Inc., Cary, NC) software. As has been previously described, 17 four of these high schools were randomly selected. The participant recruitment process was initiated on May 30th, 2014, and finalized on June 27th, 2014.
Sample Size
Sample size was originally based on individual randomization. We expected an effect size due to the intervention of at least 0.5 servings/day, with a small intracluster correlation coefficient (ICC) (i.e., 0.025). The standard deviation (SD) for the fruit intake among adolescents has been estimated to be 0.96. 23 Based on these premises and using the algorithm proposed by Donner et al., 24 and available online, 25 two clusters in each experimental condition with 100 students in each cluster (N total = 400) are 80% powered to find as statistically significant the aforementioned effect size. This calculation, however, does not account for a binary approach as is referred to in study limitations.
Inclusion Criteria
Adolescents born between 1998 and 2002 (13- to- 16-year old), who attended one of the four selected high schools were invited to participate in the study, and those who provided informed consent (forms signed by their parents/legal guardians and by the adolescent) were included. Accordingly, students in the 2nd and 3rd grades (in the Spanish education system, these grades include adolescents ∼13- to 16-year olds) participated in the study.
Intervention
The intervention included the following: (1) ACC training and (2) design and implementation of 10 activities presented as challenges (hereafter, activities) over 12 months, as showed in Table 1. The study lasted from June 30th, 2014, to May 29th, 2015, spanning two academic years (2013–2014 and 2014–2015).
The percentage of response rate was calculated according to adolescent's participation, face-to-face or social media usage.
ACCs, adolescent challenge creators; PA, physical activity; URV, Universitat Rovira I Virgili.
ACC training: a total of five ACCs from the two intervention high schools were selected by high school teachers on the basis of their knowledge of the students' leadership characteristics and English-language skills (to facilitate communication with EYTO partners). These five ACCs received a 4-hour initial training session on both SM principles and healthy lifestyle theory led by a university specialist in health and communication.
Design and implementation of the activities: the five ACCs designed activities (1.30 hours/week, during 24 weeks, conducted by health promotion and communication specialists) and implemented them to engage their school peers in the intervention. Teachers supported the ACCs by providing adequate space or just being around in case someone needed help during the activities. The themes of the activities were based on the primary and secondary objectives of the study and focused on stimulating the interest of their peers. The activities were designed to be attractive for effectively obtaining peer concern.
The ACCs presented the “Som la Pera” intervention in the 11 participating classrooms at the two intervention high schools. They explained the study, provided social media information, and invited their peers to provide suggestions for the activities. The ACCs disseminated the activities by using social media platforms, as well as direct and indirect (posters and flyers) promotion, at the two intervention high schools. In addition, information, photographs, and videos pertaining to each activity were uploaded to the campaign's social media platforms, including Facebook® (https://www.facebook.com/somlapera), YouTube®, and Instagram® (https://instagram.com/somlapera/), as described in Table 1. Social media use was measured using a Facebook analytics option, and the participating adolescents were asked about their involvement to determine how many had social media accounts.
Outcomes
The primary outcomes of the study were as follows: (1) to consume ≥1 portion/day of fruits and ≥1 portion/day of vegetables; (2) to engage in ≥6 hours/week of moderate to vigorous intensity PA. This threshold was selected and tailored from the international recommendations of a minimum PA of 1 hour of PA/day 26 ; and (3) to have ≤2 hours/day of sedentary behavior (screen time), reported as hours spent watching television, using a computer, or playing video games.
This threshold was selected by following the international recommendations of a maximum of 2 hours of screen time/day (reflecting sedentary behavior). 27 Outcomes were defined as binary variables: OK vs. No-OK (See Statistical Analyses section). Secondary outcomes included the following: (1) to increase breakfast consumption (daily breakfast consisting of more than a glass of milk or juice), (2) to reduce obesity prevalence (based on self-reported data, and (3) to obtain the engagement of local organizations as stakeholders.
All outcomes were assessed using the self-reported Health Behavior in School-aged Children (HBSC) survey from 2009–2010, 28 by an online platform accessed by the adolescents from the computer laboratory at their high schools. Adolescents in both intervention and control groups completed the HBSC survey twice, at baseline (May 2014) and at the end of the intervention (May 2015).
The retention rate was defined by the number of adolescents who answered the four questions regarding the main outcomes, which were as follows: (1) fruit consumption: number of times per week adolescents ate portions of fruits; (2) vegetable consumption: number of times per week adolescents ate portions of vegetables; (3) PA: hours per week adolescents exercised in their free time to the extent that they were out of breath or sweaty; (4) sedentary behavior (in terms of screen time): television, game console, and computer usage in separate items to capture the number of hours per day adolescents spent watching TV, playing video games or using a computer in their free time on weekends and weekdays.
Questions concerning secondary outcomes were not mandatory: (5) breakfast consumption: number of times per week adolescents ate breakfast (more than a glass of milk or juice); (6) self-reported weight and height; and (7) engagement of local organizations and stakeholders. The prevalence of obesity was assessed using self-reported weight and height, which were used to calculate body mass index (BMI) values in accordance with the International Obesity Task Force (IOTF) 29 and World Health Organization (WHO) cutoffs. 30 The classification of BMI by WHO was performed using BMI z-scores analyzed according to the WHO Global InfoBase, 31 which defines children with BMI z-scores >1 SD as overweight and >2 SD as obese.
The engagement of local organizations and stakeholders was evaluated qualitatively by their participation in and contributions to each activity. As part of the EYTO project, stakeholders' evaluations by a qualitative analysis were conducted in each of the four participating countries. Such analyses included questions about personal views and understanding of obesity in adolescents; for instance, in the “Som la Pera” intervention, participants were asked about their views on the success and challenges of the intervention; social media usage in this type of intervention, the impact of the intervention on the ACCs, adolescents who received the challenges, and policy makers and practitioners; and the future (changes needed to implement the intervention in the community over the long term).
Although the randomized high schools were located in low-income neighborhoods, individual SES was also assessed to evaluate socioeconomic factors that could affect the results. The Family Affluence Scale II (FAS II), a proxy for SES in youth, was used to measure the participants' familial material wealth. 32 The FAS II scale included questions such as (1) the number of cars that their family owned, (2) whether they had their own bedroom, (3) the number of holidays that their family went on each year, and (4) the number of family-owned computers. Each FAS II question was scored on a scale ranging from zero to nine points, and the mean lead to classify the participants as having low (0–2), middle (3–5), or high (6–9) family affluence.33,34
Statistical Analyses
Continuous variables were expressed as mean ± SD and categorical variables as percentages. The outcome for each variable was improvement at the end of the follow-up. The improvement was classified as follows: (1) Improve (OK): no good lifestyle at the beginning and good lifestyle at the end of the treatments; (2) Still Good (OK): good lifestyle at the beginning and good lifestyle at the end of the treatments; (3) Not Improve (No-OK): no good lifestyle at the beginning and no good lifestyle at the end of the treatments; and (4) Get worse (No-OK): good lifestyle at the beginning and no good lifestyle at the end of the treatments.
Multiple imputation was performed for all variables. For each variable, 100 datasets were generated using the package mice in R software and meta-analyses of these 100 datasets were performed for calculating the corresponding value. Univariate analyses were performed by χ 2 test, both for the four categories defined above and for the dichotomous variable (No-OK vs. OK).
Multivariate analyses were performed for the dichotomous variable. Cluster-randomized data were analyzed as a multilevel model with the GLIMMIX SAS-Procedure by means of the Between-Within method,35,36 which is the correct approach for this type of design, and not the parametric bootstrap, as has been recently shown by Golzarri-Arroyo et al. 37 The ICCs were calculated by means of the covariance parameter estimate provided from the SAS PROC GLIMMIX, according to Ene et al. 38 These analyses are a change concerning the approach referred to in the previous published protocol, 17 considering clustering and nesting, which was not considered previously.
To evaluate the risk of obesity according to the FAS II, multilevel models with the GLIMMIX SAS-Procedure by means of the between-within method were performed with data at baseline, with no distinction between the intervention and control groups. The significance level was set at bilateral 5% and model estimations were also reported as a coefficient and 95% confidence interval.
Results
Enrollment
Figure 1 shows the flow diagram of the adolescents' recruitment in both the intervention and control groups. A total of 521 adolescents were recruited for this study. Overall, the acceptance rate was 75.23% (392/521). The average retention rate was 76.3% (ranging from 63.5% to 88.8%) in the intervention group and 89.2% (ranging from 89.2% to 89.3%) in the control group. Specifically, in the four high schools (two in the intervention group and two in the control group), the retention rates were 88.8% in intervention high school 1 (n = 79/89, responders/recruited), 62.5% in intervention high school 2 (n = 50/80), 89.2% in control high school 1 (n = 107/120), and 89.3% in control high school 2 (n = 92/103).
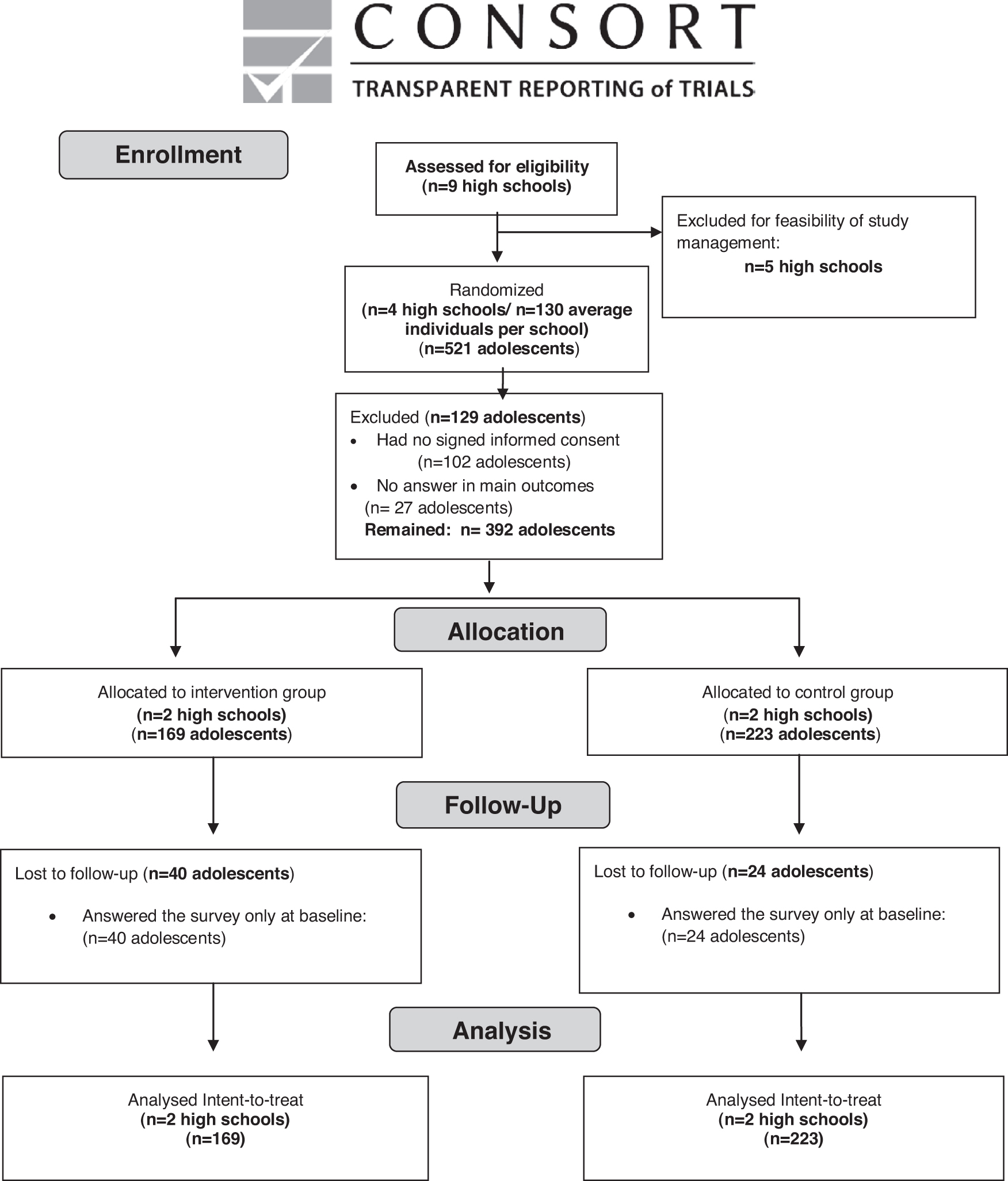
Flow diagram of participants through the “Som la Pera” study.
To increase the retention rate, the researchers returned to the high schools to remind the students to answer the HBSC online survey as well as for informing the high school teachers about which adolescents had not yet answered the HBSC survey.
Table 2 shows the baseline characteristics of participants by cluster levels and according to treatment group. Within-cluster differences, both in intervention and control groups, were observed for age (p < 0.001) and BMI (p < 0.05), and for breakfast consumption daily in the intervention group (p = 0.012). Differences between treatment groups were observed for BMI (p = 0.003) and SES (p = 0.029). When data were analyzed separately by gender (data not shown), marginal differences between intervention and control groups were also for PA in the male population (p = 0.073). The baseline screen ≤2 hours/day at weekdays was higher in the control than in the intervention group for females (p = 0.045).
BMI and age expressed as mean ± standard deviation. p by χ 2 test. p overall, p for differences between treatment groups.
BMI, body mass index; SES, socioeconomic status.
Lifestyle characteristics
Table 3 shows the changes in primary outcome lifestyle characteristics according to treatment group for the total population. After interventions, no significant difference between intervention and control groups in fruit or vegetable consumption was observed when multivariate analyses were performed. PA increased in the intervention vs. control group (p = 0.047). No difference was observed neither in screen time ≤2 hours/day on weekends, weekdays, or total or in daily breakfast consumption. When male and female groups were examined separately (Table 4), the improvement in PA remained with a borderline significance only in the male group (p = 0.050). No difference was observed in other analyzed variables. Primary outcomes ICCs for total, male, and female populations are depicted in Supplementary Table S1.
Multivariate analyses by Generalized linear mixed model (GLIMMIX procedure)//Between-Within Degrees of Freedom Approximation. Model 1, adjusted for baseline values; Model 2, adjusted by age sex, BMI, and baseline values.
CI, confidence interval; OR, odds ratio.
Multivariate analyses by Generalized Linear Models (GLmmMI package) with Clustered Data: Model 1, adjusted for baseline values; Model 2, adjusted by age sex, BMI, and baseline values.
Overweight and Obesity
For self-reported weight and height measurements, the response rate was 63.9% in the intervention group and 74.9% in the control group. The percentages of overweight and obesity (from self-reported weight and height) in the adolescents were similar across the intervention and control groups at the end of the study based on both the IOTF and WHO classifications, According to the SES of adolescents, which was based on the FAS II evaluation, 204 adolescents (53.7%) were categorized as high FAS, 155 (40.8%) as middle FAS, and 21 (5.5%) as low FAS. No difference in obesity criteria was observed when comparing SES levels (Table 5).
Multivariate analyses by Generalized linear mixed model (GLIMMIX procedure)//Between-Within Degrees of Freedom Approximation adjusted by age and sex.
The prevalence of obesity was obtained using self-reported weight and height from the HBSC survey and BMI classifications from the WHO and IOTF. The FAS II, a proxy for SES in youth, was used to measure the participants' familial material wealth.
FAS II, Family Affluence Scale II; HBSC, Health Behavior in School-aged Children; IOTF, International Obesity Task Force; NA, Non-Answer; WHO, World Health Organization.
Social media usage
The Facebook page created by the ACCs received 496 likes. Of the 169 participants in the intervention group, 113 (66.9%) followed the Facebook page, 39 (23.1%) did not follow the page, and 17 (10.1%) did not have a Facebook account or used a different nickname on their social media account. These numbers indicated only followers of the Facebook page, while several interactions among adolescents who did not follow the page were found throughout the study during the Facebook activities, such as using the information posted to the classroom wall or schoolmates' internal chats. In addition, none of the students in the control group followed the “Som la Pera” Facebook page. However, it could be possible that some of them had consulted the Facebook page without following it because the page was not private.
Stakeholders' engagement
Local organizations, such as the central marketplace, public high schools, city council, and local university, supported the “Som la Pera” intervention as keystone stakeholders by providing fresh food and beverages and hosting specific activities. Moreover, national and international organizations supported the EYTO project by disseminating information in local, national, and international media. The participation of different stakeholders was qualitatively evaluated. The information revealed that (1) relevant and accessible information can be provided using a youth-led approach; (2) accessible choices are required for young people to make healthy choices; and (3) collaborative and holistic approaches are necessary to address obesity in adolescent populations. 39 A final report of the results of the qualitative analysis of the EYTO project was published. 40 For each challenge, the involvement of at least one stakeholder was essential and their participation is showed in Table 1.
Discussion
“Som la Pera,” a school-based peer-led SM intervention, was designed to encourage adolescents from disadvantaged neighborhoods to make healthy lifestyle choices by implementing 10 activities over 12 months. The intervention improved the weekly PA participation in the intervention group vs. the control one, particularly in males. Other lifestyle outcomes were not improved by the “Som la Pera” intervention.
This study provided evidence, through a peer-led intervention, that ACCs may have credibility among young peers. Our results support previous data concerning that adolescents may serve as positive role models, and thus, ACCs could influence their peers' specific health-related lifestyles. 41 Results of adolescent peer-led interventions suggest that they may generate more favorable results than adult-led interventions when targeting adolescents. 42 The “Som la Pera” study, however, is the first study incorporating a peer-led intervention with an SM methodology to encourage a healthy lifestyle in adolescents. According to social cognitive theory, social influence greatly impacts individual thoughts and behaviors.
Other emergence theories support that individual behavior and learning arise from interactions within and between the individual and the environment. 43 Results of the “Som la Pera” intervention are a novel joint approach for the use of SM and peer-led education, as well as the empowerment of young people in the design and implementation of a lifestyle improvement intervention.
The WHO estimates that half of the European population do not consume the recommended daily amount of five portions of fruits and vegetables (400 grams). 44 According to the HELENA Study, European adolescents consume ∼200 grams/day of fruits and vegetables, which is one-half the amount recommended by the WHO. 45 In our study, after 12 months of intervention, there was a 10.4% increase in the number of adolescents who consumed at least one portion of fruit per day, although this percentage did not reach significance in the multivariate analyses. The daily recommended amount of fruits and vegetables has been associated with a lower risk of mortality, particularly from cardiovascular disease. 46
According to the European Heart Network, 47 each piece of fruit or vegetable (106-gram portion) consumed daily decreases cardiovascular risk, the leading cause of mortality worldwide, by a 4%. However, it is not totally established that fruit and vegetable consumption are causally related to obesity. Reviews and analyses of fruit and vegetable intake on long-term weight change or weight loss in men, women, and children reached a range of conclusions from no discernible effects, modest ones, or significant effects.48,49
Regarding PA, the percentage of adolescents who progressed toward the goal of at least 60 minutes of moderate to vigorous PA per day 26 was more than double in the intervention group than in the control one (39.1% vs. 17.9%), this difference reaching statistical significance. The great PA daily practice accounts particularly for the male where a significant 60.5% reached the goal vs. 16.9% of the females. Our data show that adolescents in the “Som la Pera” intervention group exhibited higher PA participation, 16.9% in female and 60.5% in male than the 15-year-old female (12%) and male (28%) Spanish adolescents described in the 2013/2014 HBSC International Report. 2 Adolescents, specifically girls, are at risk of physical inactivity.
Due to this, recently, several peer-led studies have been designed to increase PA in adolescent girls. The G-PACT Project, a three-tier peer-led mentoring model improved PA levels and reduced sedentary time in adolescent girls when an exercise class after-school component was included. 50 The PLAN-A is an on-going study, but preliminary data show its feasibility for increasing PA in adolescent girls. 51 The WISH study, a peer-led walking-in school intervention, shows limited effects on improving PA in adolescent girls in its pilot phase. 52 Gender differences in the results of “Som la Pera” intervention were consistent with the findings of previous studies showing higher levels of PA in males. 6
Our results support the fact that a healthy lifestyle in youth is influenced by gender. In the “Som la Pera” intervention, females showed more interest than males in participating in the activities created by the ACCs when they involved food or cooking activities, whereas males showed more interest than females in the PA-promoting activities. The gender differences in lifestyle improvement may be the result of differences in preferences, attitudes, social desirability, or diet status. 53 In addition, learning strategies could function differently between genders; in this study, females respond more enthusiastically to traditional classroom and theoretical environments, and males may be more involved when experiential learning is used as a strategy to improve lifestyles, as found in other studies. 54
We did not observe improvements in the sedentary behavior, measured as screen time per day, in our Som la Pera intervention. To achieve a greater reduction in sedentary behavior, some previous studies have suggested that the involvement of family members, and the home environment, as a part of the intervention could be a suitable option for addressing the issue. 55 This idea can also be extended to fruit, vegetable, and breakfast consumption since it is easier to manage these dietary behaviors at home.
However, changes in dietary behaviors at home require the involvement of parents for the intervention to be successful, with the parents adopting the same healthy lifestyle aims as their children. 56 In terms of the secondary outcomes, the “Som la Pera” resulted in no significant improvement in the prevalence of obesity after the intervention. The maintenance of obesity prevalence could be attributed to an insufficient time to detect a change in youth BMI due to the fact that the participants were healthy adolescents, and not overweight or obesity ones.
This study has limitations. First, data are based, as in the most part of surveys, on self-reported information, including body weight and height. This policy was implemented to avoid the difficulties of persuading adolescents to participate in weight measurements. 57 Also, PA was assessed using a questionnaire, whereas PA is more precisely measured using an accelerometer. Regarding the PA findings for males, it cannot be distinguished whether the observed effects are due to the peer-led intervention or to the greater numbers participating in PA, which can influence others (similar to the crowd effect).
A recruitment bias exists due to the fact that subject recruitment was performed after randomization of schools. Also, sample size was calculated on the basis of servings/days and not for a binary response. Although a lack of access to technologies for social media platforms, other than Facebook, was neither reported by participants nor detected by the ACCs or the researchers, a specific question on the issue was not performed. Due to this, some participants from low-income households could have had limited access to technologies that are used to access social media platform. In addition, and related to the HBSC survey, the assessment of sedentary behavior only accounted for screen time and not for sedentary behavior as a whole. 28
Other limitations are that only two clusters per group were evaluated, the retention rate was 1.54% lower than expected, and a higher retention rate in the control group than in the intervention group. These facts could account for the lack of significant results obtained in other outcomes than PA (i.e., fruit consumption). High school 2, one of the intervention high schools, had a lower retention rate due to a lack of encouragement of the adolescents to answer the questionnaires, such as the provision of school time, computer laboratories, and reminders. Finally, in this study, only short-term behavioral changes were measured; the maintenance of these behaviors over longer periods of time not being assessed.
Nevertheless, the main strength of this study was that the “Som la Pera” intervention was created by adolescents for adolescents. The ACCs designed attractive activities with a meaningful message using the SM and peer-led education as the methodological basis, and empowering young people in the design and implementation of the intervention was crucial for the study's success.
The inclusion of teachers, local organizations, and policy makers as stakeholders may have also influenced the positive results of this intervention on PA because these groups actively contributed to the adolescent's environment. In addition, the adolescents in the study were likely motivated by knowing that their peers were participating in similar interventions across Europe, allowing them to share and apply their ideas. The SM and peer-led methodologies ensured relevant content was created for adolescents living or attending high schools in low-income neighborhoods, given that peer leaders and participants were from the same social environment. A pending issue for future work is to investigate the effectiveness of the peer-led SM intervention vs. an adult-led SM intervention.
Conclusions
A school-based, peer-led SM intervention designed and implemented by adolescents attending high schools in low-income neighborhoods effectively improved the PA, particularly in males. This fact points out that a healthy lifestyle in youth could be influenced by gender. Increasing PA activity in adolescents, although at small daily changes, may yield long-lasting health benefits and a significant reduction in chronic diseases in adulthood. No effect on fruit or vegetable consumption or screen time per day was observed.
Footnotes
Acknowledgments
This project benefited from valuable collaborations with the National Children's Bureau (the United Kingdom), Companhia de Ideias (Portugal), and Komunikujeme (Czech Republic). The Spanish research project was supported by the Central Market of Reus, Spain (Mercat Central de Reus), which provided fresh food for the intervention, and the Municipality of Reus, Spain [Ajuntament de Reus, Spain]. We thank the teachers, parents, and students of the Reus high schools for their enthusiastic participation in this study.
Funding Information
This research project was funded by the European Commission (European Directorate General HEALTH-2012 12 19). This funder did not play a role in the Spanish study design, data collection, study management, data analysis, data interpretation, article writing, or decision to submit the report for publication.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.