
Abstract
Background:
Adolescents with severe obesity and comorbid mental health issues are the most resistant to traditional weight management approaches and have poor treatment outcomes. Our objective was to implement and evaluate a pilot day hospital treatment program for adolescents with severe obesity, or risk for severe obesity, and significant mental health comorbidities.
Methods:
This was a prospective cohort study of adolescents 12–18 years of age with severe obesity (BMI >99th percentile), or at risk for severe obesity, and comorbid mental health issues. The intervention, focused on healthy lifestyle and mental health support, was implemented within an existing psychiatric day hospital at a pediatric quaternary care hospital. Anthropometric and mental health measures were analyzed pre- and postintervention.
Results:
Thirty-two adolescents with a mean age of 14.9 years [standard deviation (SD) 1.6] participated in the pilot integrative day hospital program for a mean duration of 5.2 months (SD 2.3). Eleven participants had primary severe obesity and comorbid mental health conditions (obesity subgroup) and 21 participants had primary mental illness and were at risk for obesity (psychiatry subgroup). We did not observe a significant difference between BMI pre- and postprogram among adolescents in both subgroups. In other words, adolescents in both subgroups achieved weight maintenance. Fear in losing control of overeating and/or being seen by others when eating decreased significantly in the obesity subgroup [mean difference (MD) 0.99; 95% confidence interval (CI): 0.27 to 1.71]. There was a significant decrease in participant-reported depression symptom severity, both overall and within program subgroups. Quality-of-life scores of study participants improved significantly within the obesity subgroup (MD −12.31; 95% CI: −21.69 to −2.93), but not within the psychiatry subgroup (MD −6.35; 95% CI: −13.37 to 0.67).
Conclusions and Implications:
A day hospital model of care may result in weight maintenance, decreased eating concerns, and improved mental health in adolescents with severe obesity or risk for severe obesity, and significant mental health comorbidities.
Introduction
Nine to 17% of Canadian youth (5–19 years of age) are classified as obese. Worldwide, 158 million youth are estimated to currently meet criteria for obesity and by 2030 this number is expected to rise to 254 million if better prevention and treatment interventions are not identified and implemented. Youth who are overweight or obese are at risk for a number of medical and mental health conditions that can significantly impact quality of life and life span.1–6
Existing obesity treatment programs tend to focus on reduction in weight or BMI as their main outcome, and struggle to show homogeneous and lasting improvements. Multiple complex factors contribute to the condition of obesity, and to the ability of youth and their families to adhere to treatment recommendations.7,8 Most individuals diagnosed as overweight or obese are not identified as having an eating disorder. However, there is a strong correlation between obesity and disordered eating behaviors such as binge eating and very strict dieting/fasting behaviors. 9 It is likely that more varied and targeted approaches are needed for subgroups such as those with severe obesity, disordered eating (binging and/or restriction behaviors), as well as comorbid mental health issues that significantly disrupt daily functioning (severe social anxiety, chronic school refusal, etc.). Past studies have shown such individuals have poorer weight outcomes within treatment programs.10–12
There are few reported interventions specifically designed to concurrently address severe obesity, disordered eating, and significant mental health issues among youth. Traditional outpatient mental health treatment programs often do not have sufficient focus on the complexities of eating and activity, and conversely, traditional weight management programs often do not provide sufficient treatment for moderate-to-severe mental health issues. 4 Most comprehensive healthy lifestyle programs for youth utilize cognitive behavior therapy (CBT) paired with nutrition and physical activity education and instruction, and report modest overall changes in weight with some improvement in general mental health parameters such as quality of life and short-term depression and anxiety symptoms.4,13,14 For individuals with severe obesity and significant comorbid mental health issues, disordered eating behaviors may be so intertwined that outpatient treatment alone is not enough to engender lasting change.
Only a handful of studies have looked at more intensive weight management treatment options such as inpatient programs, boarding schools, and residential weight loss camps.15–20 These programs were not designed to concurrently treat significant mental health issues. Several of these studies reported significant outcomes of short-term weight loss but questions of psychological impact and eventual weight regain remain. The most intense of these programs, a 10-month inpatient CBT treatment program, reported that 82% of participants maintained at least a 10% weight loss at 14 months. 15 Youth who completed this program also showed improvements in measures of self-perception, internalizing behaviors, and disordered eating behaviors. 15 However, funding for such long-term programs is difficult to secure, they require youth to be away from their home environment for an extended period, and generalization of learned skills outside of such programs can be challenging.
In mental health, an intermediate level of treatment intensity is offered via day treatment programs, which allows youth to remain in their community while receiving intensive treatment during the day. Despite studies demonstrating this model as successful for eating disorders, we found no published studies investigating the effectiveness of a day treatment approach for youth with severe obesity.21,22 This study was designed to address this gap with the development and assessment of a pilot treatment program for youth with both severe obesity or at risk for severe obesity and significant mental health issues within a day hospital model.
Materials and Methods
Study Design
This was a pilot prospective cohort study of adolescents with severe obesity or at risk for severe obesity, and comorbid mental health issues. The intervention was developed by clinicians from several specialty programs at a large pediatric quaternary care hospital in Toronto, Ontario, Canada, including obesity management, eating disorders, and acute care psychiatry. Clinicians collaborated to design, and iteratively refine, a new model of care within an already existing adolescent general psychiatry day hospital program to include healthy lifestyle treatments for youth with comorbid severe obesity (BMI >99%) and youth with lower BMIs but at risk for severe obesity due to use of medicines such as antipsychotics which can cause considerable weight gain. The program was not focused on weight reduction, but used CBT to teach youth how to attain a healthy lifestyle, increase physical activity and healthy eating habits, and develop skills in general mental health.
Participants
Demographic characteristics (e.g., age, socioeconomic status, diagnosed medical and psychological comorbidities) were collected at study entry. Forty-two participants entered the pilot integrative day hospital program between September 2015 and September 2018. Ten of these declined participation in the research study. Participants came from outpatient general psychiatry programs or the multidisciplinary obesity management program within the hospital, a family-based program focused on healthy living for adolescents aged 12–17 years with complex and severe obesity.
At entrance into the program, a member of the research team approached and explained the purpose and details of research within the program. Participants were given the opportunity to ask questions and then asked whether they were willing to participate.
To be eligible for the program, individuals needed to be 12–18 years of age and have a mental health diagnosis with current significant impairment in daily functioning. Those entering from the obesity management program had the same criteria, along with a BMI >99%. The program accepted youth with all diagnoses who could participate in group-based programming, except for those with substance use disorders, anorexia nervosa or bulimia nervosa, as the institution has separate specific day hospital programs to address these disorders. The program had a rolling entry process and the maximum number of patients at any one time was eight, up to three of which were diagnosed with comorbid severe obesity.
Comorbidities such as binge eating disorder were determined using a comprehensive mental health assessment based on Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria conducted by psychologists and eating disorder expert physicians. In addition, the clinical assessment was used to assess patient needs and inform care plans including suitability for the pilot integrative day hospital program.
Treatment
The pilot integrative day hospital program was a CBT-based program that also included dialectical behavior therapy mindfulness/distress tolerance skills. Participants engaged in a combination of group therapy, family sessions/therapy, individualized therapy, and experiential learning opportunities from 9:00 am to 2:30 pm Monday through Friday. Target treatment duration was set at 4–6 months and was dependent on treatment response, as well as patient and family engagement. The groups and social exposures were delivered by two highly experienced child and youth workers under the supervision of a child psychiatrist. Family therapy and individual therapy sessions were provided by either a social worker or psychologist with a target frequency of once a week. Participants also received 2 hours of daily educational support from certified teachers. The goal was to help youth achieve an improvement in functioning and a decrease in mental health symptoms.
Specialized healthy lifestyle programming was also delivered in group, individual, and family formats. The programming included instruction and practice of normalized eating (3 meals per day and 2–3 snacks per day, 2–3 hours apart) along with active living practices. Eating behaviors that occurred at home (overnight and on weekends) were processed with patients regularly in the program. Dietitians modified the nutrition choices available for breakfast and snacks, which included a late afternoon “snack on-the-go,” to ensure participants continued normalized eating patterns. Dietitians ran regular groups that included traditional nutrition education, cooking classes, and grocery store tours. An exercise therapist was available to work with participants either in a group or individually, as requested, and included trips to the local fitness gym. Groups run by psychologists offered specialized support around obesity-specific issues such as binge eating/loss of control eating, body image, low self-esteem, victimization from bullying, and social isolation/anxiety.
Primary Outcome Measures
We examined weight and BMI pre- and posttreatment program. Weight maintenance was defined as no change in BMI. BMI was calculated using the World Health Organization growth references. 23 Anthropometric data (e.g., height, weight, and BMI) were gathered upon referral and chart review. All participants had height and weight measured at program entry by a registered nurse, who trained and worked with an obesity management program. Single measures of weight were obtained for all participants in the morning before breakfast, with clothing but no shoes, and using a bariatric scale. Weights before program entry were collected using clinically approved equipment and methodology and were used to help determine weight trajectory over time.
Additional anthropometric measurements were obtained at study entry and exit for all patients when possible. Several other measurements occurred at intervals ranging from weekly to monthly depending on individual patient needs and risk factors. Cardiometabolic measures included fasting lipid profile, insulin, glucose, and hemoglobin A1c. In addition, eating behavior was measured through participant report on the Eating Disorder Examination Questionnaire (EDE-Q) and through completion of a 24-hour recall of dietary behaviors.24,25
Secondary Outcome Measures
Upon program entry and exit, patients and their caregivers also completed a set of empirically validated psychological questionnaires to assess depression, anxiety, weight, and health-related quality of life, satisfaction with care, and parenting stress: Children's Depression Inventory 2 (CDI 2), Multidimensional Anxiety Scale for Children 2 (MASC 2), Pediatric Quality of Life Teen Report 4.0 (PEDSQL), Peds QL—Healthcare Satisfaction Questionnaire (Parent PEDSQL), and the Stress Index of Parenting Adolescents (SIPA).26–30
Data Analysis
Demographics were summarized with means and standard deviations (SDs) for continuous variables, and counts and proportions for categorical variables. We examined the effects of time and subgroup with a repeated measure analysis of variance (ANOVA) that included an interaction term between time and subgroup. Differences between pre- and postscores are presented along with confidence intervals (CIs) and p-values for the overall cohort, and for obesity and psychiatry subgroups. To analyze weight trajectories in the obesity subgroup, a mixed effects linear regression model, with a random effect to account for the repeated measurement of each individual over time, was used. The model includes a term for time to account for the baseline trend in BMI change per day and a term for the number of days spent in the program to account for a potential difference in this trend once the program started. The data used in the model are displayed in Figure 1.
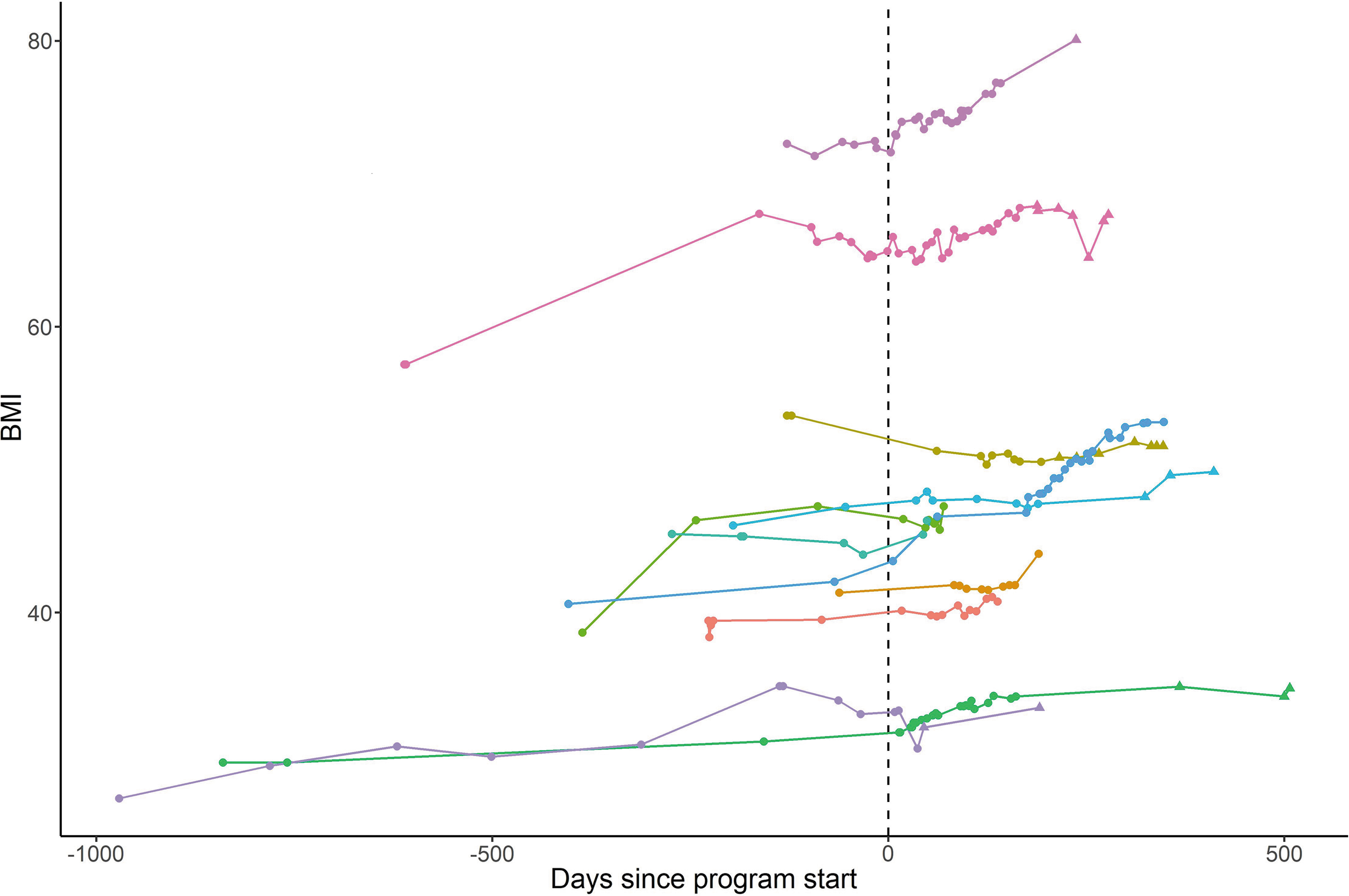
BMI trajectory of adolescents enrolled in the pilot integrative day hospital program for the participants in the obesity subgroup.
Correction for multiple comparisons was restricted to our primary study outcomes, and significance levels were corrected using the Bonferroni adjustment. We chose not to do this for our secondary outcomes as this was a pilot study and these outcomes were meant to be more exploratory and hypothesis generating. Statistical analysis was performed using SAS 9.4.
Institutional Review Board (IRB) Approval Statement and Statement of Patient Consent
Patients and families who agreed to participate were provided with a written informed consent form. This study is approved by the research ethics board at the Hospital for Sick Children (REB approval #1000055259).
Results
Participants
Thirty-two adolescents with a mean age of 14.9 years (SD 1.6) participated in the pilot integrative day hospital program for a mean duration of 5.2 months (SD 2.3). Eleven participants had primary severe obesity and comorbid mental health conditions (obesity subgroup) and 21 participants had primary mental illness and were at risk for obesity (psychiatry subgroup). Demographic characteristics of study participants are described in Table 1 (note large amount of missing data). Most participants identified as female (69%) and White/Caucasian (43%). Although not all parents reported on education and income, most reported having completed high school (44%) and having an income of $40,999 or less (58%).
Demographic Characteristics of Adolescents Enrolled in the Integrative Day Hospital Program for the Full Sample (n = 32)
SD, standard deviation.
Clinical characteristics of study participants including baseline anthropometrics and major mental health concerns are described in Table 2. Participants in the obesity subgroup and psychiatry subgroup had a mean BMI of 47.5 kg/m2 (SD 12.6) and 23.3 kg/m2 (SD 6.1), respectively. The most common mental health concerns diagnosed for participants in the obesity subgroup were anxiety disorders (73%), depression/depressive disorders (27%), disordered eating/binge eating disorders (27%), and attention-deficit hyperactivity disorders (27%). Similarly, participants in the psychiatry subgroup were commonly diagnosed with anxiety disorders (71%). However, more participants in the psychiatry subgroup reported depression/depressive disorders (48%) and obsessive-compulsive disorders (24%). The majority of participants (n = 27) had more than one major mental health concern.
Clinical Characteristics of Adolescents Enrolled in the Integrative Day Hospital Program for Program Subgroups (n = 32)
Includes major depressive disorder, dysthymia, and major depressive episode.
Includes substance use disorder, gender dysphoria, oppositional defiant disorder, and bipolar affective disorder.
ADD, attention-deficit disorder; ADHD, attention-deficit hyperactivity disorder; OCD, obsessive-compulsive disorder; PTSD, post-traumatic stress disorder.
Primary Analysis: Anthropometric and Eating Behavior Outcomes
Results on anthropometrics and eating behavior pre- and postprogram are presented in Table 3. The repeated BMI measurements of patients in the obesity subgroup were modeled as a function of time and time since beginning the program using a linear mixed effects model. Patients' BMI increased on average by 0.62 per 100 days (95% CI: 0.47 to 0.77), and once they started the program, their weight changed by an additional 0.30 per 100 days (95% CI: −0.02 to 0.61) (Fig. 1). Cardiometabolic laboratory measures did not demonstrate significant change within program subgroups. Regarding eating behavior measures, EDE-Q subscale scores were decreased for eating concerns [mean difference (MD) 0.99; 95% CI: 0.27 to 1.71] (fear in losing control overeating and/or being seen by others when eating) after treatment only in the obesity subgroup. EDE-Q subscale scores for weight, restraint, shape concerns, and the total global score did not demonstrate significant change within program subgroups.
Results from an ANOVA Examining the Pre- and Postprogram Data on Anthropometrics, Cardiometabolic Measures, Eating Behavior of Adolescents Enrolled in the Integrative Day Hospital Program for the Full Sample and Program Subgroups (n = 32)
Bonferroni adjusted significance is p < 0.007.
Bonferroni adjusted significance is p < 0.01.
ANOVA, analysis of variance; CI, confidence interval; EDE-Q, Eating Disorder Examination Questionnaire; MD, mean difference.
Secondary Analysis: Psychological Outcomes
In Table 4, pre- and postprogram data on secondary research objectives are presented as full sample and within program subgroups. There was a significant decrease in participant-reported depression symptom severity, as measured by pre- and postprogram CDI 2 scores, both overall and within program subgroups. Participant CDI 2 scores in the obesity subgroup decreased from elevated to average or lower (MD 9.36; 95% CI: 1.44 to 17.28), whereas participants in the psychiatry subgroup experienced a similar significant decrease from very elevated to high average (MD 7.00; 95% CI: 1.34 to 12.66). 31 Although not statistically significant, there was a trend toward improvement in anxiety symptoms overall (MD 3.37; 95% CI: −1.21 to 7.95) within the obesity subgroup (MD 2.79; 95% CI: −4.65 to 10.23) and psychiatry subgroup (MD 3.95; 95% CI: −1.39 to 9.30), as demonstrated by decreased MASC 2 participant-reported mean scores postprogram.
Results from an ANOVA Examining the Pre- and Postprogram Data on Anxiety, Depression, Patient's Quality of Life, Parental Satisfaction with Care, and Parent–Adolescent Interactions of Adolescents Enrolled in the Integrative Day Hospital Program for the Full Sample and Program Subgroups (n = 32)
Total score that incorporates physical, emotional, social, and school functioning scores.
Total score that incorporates information, inclusion of family, communication, technical skills, emotional needs, and overall satisfaction scores.
CDI, Children's Depression Inventory; MASC, Multidimensional Anxiety Scale for Children; Parent PEDSQL, Peds QL—Health Care Satisfaction Questionnaire; PEDSQL, Pediatric Quality of Life Teen Report 4.0; SIPA, Stress Index of Parenting Adolescents.
Quality-of-life scores of study participants improved significantly within the obesity subgroup (MD −12.31; 95% CI: −21.69 to −2.93) but not within the psychiatry subgroup (MD −6.35; 95% CI: −13.37 to 0.67). Similarly, a statistically significant increase in the total score for health care satisfaction reported by participants' parents was seen only in the obesity subgroup (MD 12.48; 95% CI: 1.29 to 23.66).
In the psychiatry subgroup alone, the SIPA demonstrated a statistically significant decrease in the pre- and postprogram scores for the adolescent domain (MD 8.40; 95% CI: 2.51 to 14.28), which include the following subscales: moodiness/emotional lability, social isolation/withdrawal, delinquency/antisocial, and failure to achieve or persevere. In the adolescent-parent relationship domain, which included themes of affection, openness, communication, and the enjoyment of adolescent parent interactions, no statistically significant changes were seen in the full sample (MD 2.09; 95% CI: −16.19 to 20.38) nor within the obesity subgroup (MD 1.90; 95% CI: −30.24 to 34.04) or psychiatry subgroup (MD 2.28; 95% CI: −15.19 to 19.75).
Discussion
The aim of this study was to develop, implement, and evaluate a pilot integrative day hospital program that provided individualized and intensive treatment to a complex adolescent group with both severe obesity, or risk for severe obesity, and significant mental health comorbidities. Our key findings were that youth in both obesity, and psychiatry subgroups achieved weight and BMI maintenance and experienced a decrease in depressive symptoms. Specifically, within our obesity subgroup, youth had reduced eating concerns, and improved quality of life was observed for both youth and parents. In the psychiatry subgroup, significant improvements were noted in youth emotional lability, social isolation, antisocial behavior, and perseverance.
Much of the current pediatric obesity literature focuses on weight reduction as a primary intervention outcome.13,32 However, treatment-seeking adolescents with severe obesity (BMI >99%) often have an upward trajectory of weight gain before starting specialized treatment. 33 For such individuals, weight maintenance, such as seen in our program, should be considered a marker of success.
Equally noteworthy is the significant reduction in eating concerns and improved quality of life. For some, this is indicative of a drop in the fear of loss of control eating and less fear of eating in front of others that aligns with increased general coping skills, self-acceptance, and ability to follow through with normalized eating, all of which are key developments for healthier living and well-being. The day treatment model provided in vivo practice/exposure opportunities over a consistent period that allowed for the proper development of these skills. Although well established and widely used, clinical cutoff scores for the EDE-Q are not yet well established for youth, especially those with severe obesity. 34 In our study, we found a statistical decrease in the subscale of eating concerns that indicates a reduction in the fear of losing control of eating/overeating and/or being seen by others when eating. A major obstacle to normalized regular eating for youth with severe obesity is eating in front of others as they often feel judged, and the resulting irregular eating patterns can lead to feelings of lack of control once eating begins. Any reduction in this construct is considered highly beneficial for this population.
Patients with restrictive eating disorders have a wide array of treatment options including outpatient, inpatient, day hospital, and residential care depending on level of disease severity. However, there is a lack of appropriate care options for youth with disordered eating disorder and/or severe obesity, which highlights possible inequities in care. 35 Given the increasing prevalence of obesity and mental illness in adolescents, it is critical to create the evidence needed to support these treatment models of care for youth.
Our day treatment program achieved mental health improvements and shifts in healthy lifestyle behaviors in patients for which outpatient treatment had failed. In addition, school-avoidant participants were offered individualized school support, developed skills for future school re-entry, and received guidance to facilitate transition out of the pilot integrative day hospital program. By allowing participants to maintain their regular home environment and involving family in treatment, new strategies discussed in our program could be used, practiced, and supported by youth and their family members to improve coping with life stressors. Although family member involvement was perceived as a benefit of the day hospital program experience by patients, parents/caregivers, and clinicians, their engagement was challenging due to personal life factors related to financial stressors, competing work schedules, and burden of transportation.
The pilot integrative day hospital program, the first of its kind in Canada, featured intensive and holistic programming provided by multidisciplinary health care professionals who provided treatment for both the physical and emotional health needs of this adolescent population with medical and psychiatric complexities, along with their families. The extended program duration of 4–6 months was unique and the group milieu within the program provided a continued safe space for participants to connect with peers, as many experienced school refusal due to bullying. Furthermore, clinicians and program administrations met regularly to evaluate and iterate the treatment design in real time to better address participant and team needs.
Limitations
This was a small pilot study completed in a quaternary care hospital setting with more resources than may be available in smaller or community hospitals, thereby affecting its generalizability. In addition, the small sample size, especially within the two subgroups, may have had inadequate power to detect changes in the outcomes of interest. Additional study limitations included some missing questionnaire data, issues with participant retention, and a lack of a comparison group. Program duration was determined by individual engagement and treatment response. In some cases, transition out of the program proved to be more difficult for patients and families to accept. This may have impacted actual responses to questionnaires as some wanted to appear to be relapsing to stay in the program, and in some cases, they refused to complete follow-up questionnaires. These challenges likely caused, if anything, an underestimation of the positive effects of the program. Parents were difficult to engage in completing questionnaires and required multiple reminders. Future treatment studies may collect end-of-treatment outcomes before the actual discharge phase. The iterative design also made it difficult to discern which specific program component was the most effective in improving the various participant outcomes. As numerous providers and variable intervention strategies were required to deliver the model of care, this likely led to some treatment inconsistencies among program participants.
Conclusions
Preliminary evidence from our pilot integrative day hospital program suggests promise for a much needed collaborative and integrative model of physical and mental health care. Further study is needed to determine what components of a day hospital program are most effective for youth with severe obesity or risk for severe obesity and significant mental health comorbidities to inform new models of care for this population.
Footnotes
Authors' Contributions
All authors meet the definition of authorship, as defined by the International Committee of Medical Journal Editors, and (1) made substantial contributions to the conception or design of the study or the acquisition, analysis, or interpretation of data for the study; (2) drafted the study or revised it critically for important intellectual content; (3) obtained final approval of the version to be published; and (4) agreed to be accountable for all aspects of the study in ensuring that questions related to the accuracy or integrity of any part of the study are appropriately investigated and resolved.
Acknowledgments
The authors thank all the health care providers who provided excellent clinical care and support to the adolescents and families in the day hospital program. We thank Keshini Devakandan, clinical research project coordinator, for her support in preparing this article for submission.
Funding Information
Funding for this project was provided by the Medical Psychiatry Alliance.
Author Disclosure Statement
No competing financial interests exist.