
Abstract
Introduction:
Type 2 diabetes and obesity are metabolic diseases that have grown into a global, unstoppable pandemic. Despite strong and well-developed pharmacological treatment methods, their prevalence is still increasing and out of control.
Methods:
With the development of bariatric and metabolic surgery, as a successful method in the treatment of obesity and type 2 diabetes, the term “reversal” or “remission” of a previously irreversible disease began to be mentioned.
Results:
The most successful and performed bariatric and metabolic methods are SG (sleeve gastrectomy), OAGB (one anastomosis gastric bypass), and RYGB (Roux-en-Y gastrectomy). Achieving significant regulation of glycemia, the effect on numerous metabolic processes and the long-term effect of the therapy itself make bariatric and metabolic surgery the most successful method in achieving diabetes remission.
Conclusion:
Numerous studies, results and experience, weighing risks and benefits have placed bariatric and metabolic metabolic surgery in the clinical guidelines for the treatment of type 2 diabetes.
Keywords
Introduction
The world is struggling with two rapidly growing global pandemics—diabetes mellitus and obesity, which are significant public health and socioeconomic problems.1–4 Precisely because of their overlap in pathogenesis, some antidiabetic drugs act on obesity by increasing body weight, while some anti-obesity drugs can be antidiabetic. 5 Numerous clinical studies have shown a significant and powerful effect of drug therapy and a strong emphasis on the prevention of the diseases themselves. But in choosing the right therapeutic option, the importance of bariatric and metabolic surgery, which is effective for both, is being mentioned more and more. Especially, restrictive procedures (e.g., sleeve gastrectomy [SG]) and restrictive/malabsorptive procedures (e.g., Roux-en-Y gastric bypass [RYGB], one anastomosis gastric bypass [OAGB]) have a significant effect on improving glycemia and can lead to diabetes reversal.4,6 Despite the still unknown precise mechanisms that contribute to the resolution of diabetes after bariatric and metabolic surgery, the impact of bariatric and metabolic surgery on diabetes is undeniable.2,4–6 Experience and results, weighing the risks and benefits of bariatric and metabolic surgery over the past 70 years, have led to current clinical practice recommendations that include bariatric and metabolic surgery in the treatment of type 2 diabetes.
Search strategy
For this literature review, controlled vocabulary (MeSH) and keyword terms on PubMed were utilized, keywords being diabetes mellitus, obesity, bariatric metabolic surgery, RYGB, SG, OAGB, reversal, and remission diabetes. We analyzed systematic reviews, meta-analyses, and clinical trials from 2003 onward. In the section “Bariatric and Metabolic Surgery,” glancing at bariatric and metabolic surgery history, we referred to the original procedure articles published from 1967 to 1998.
Overlapping diabetes and obesity
Since 1973, the pathophysiological connection between type 2 diabetes and obesity has been established. Then, due to the increase in the incidence and prevalence of diabetes and the increase in the prevalence of obesity, both have become global, leading pandemics that represent a major public health and socioeconomic problem. 5 According to the latest data from the World Health Organization, about 422 million people have diabetes, and 1.5 million deaths are directly attributed to diabetes each year.7,8 Globally, 813 million adults are obese. 9 About 90% of patients with diabetes type 2 are obese, but only 23% of patients with severe obesity suffer from diabetes type 2.2,5 In its World Obesity Atlas 2023, we can see that the economic impact of overweight and obesity on the world is set to reach $4.32 trillion. 10 Numerous clinical studies have shown a significant and powerful effect of drug therapy and a strong emphasis on the prevention of the diseases themselves. However, 44% of patients with diabetes and treated with medical therapy have uncontrolled diabetes. 5 The situation with the treatment of obesity is similar.
Obesity, in addition to being the strongest risk factor for the development of type 2 diabetes, is also a risk factor for other chronic diseases (cardiovascular diseases, liver, metabolic diseases).2,5 Considering the connection between their pathologies, the main goal in the treatment of obesity and diabetes is weight reduction. 5 Current treatment methods often lead patients into a vicious cycle—the struggle to treat hyperglycemia with the use of some drugs (e.g., sulfonylureas, insulin, thiazolidinediones) often leads to obesity, while the use of glycemic-lowering drugs (glucagon-like peptide 1 [GLP-1]) in the treatment of obesity is often not sufficient for weight reduction and is not a long-term solution.5,11
Therefore, it is extremely important to find the right therapeutic option as soon as possible in order to slow down these two fast-growing pandemics and reduce public health costs. 5 More significantly, high-quality research proves bariatric and metabolic surgery as the superior and most effective method of treating obesity and diabetes.5,7
The latest American Diabetes Association’s guidelines from 2023 recommend bariatric and metabolic surgery as an option to treat type 2 diabetes in screened surgical candidates with body mass index (BMI) ≥40 kg/m2. Metabolic surgery may be considered as an option to treat type 2 diabetes in adults with a BMI of 30.0–34.9 kg/m2 (27.5–32.4 kg/m2 in Asian American individuals) who do not achieve durable weight loss and improvement in comorbidities (including hyperglycemia) with nonsurgical methods. 12
Bariatric and metabolic surgery
The International Federation for Surgery of Obesity and Metabolic Disorders Seventh Global Registry Report records 311,441 bariatric and metabolic surgery procedures performed in either 2020 (United States) or 2021 (rest of the world). This difference is due to differences in reporting cycles. 13 Bariatric and metabolic surgery is nowadays considered as a standard modality of obesity treatment. Weight loss operations have their beginning in the 1950s with the introduction of jejunoileal bypass (JIB). In the late 1960s and early 1970s, JIB was shown to produce permanent weight reduction and became the most performed operation. However, as the patients were long-term observed, many untoward complications became evident. Because of many complications, it was suggested that the JIB is not an appropriate operation for morbidly obese patients, and it was abandoned in the 1980s. 14 Eduard Mason performed the first gastric bypass in 1966, and in 1977, this technique was modified, introducing the RYGB procedure—nowadays considered a golden standard in bariatric and metabolic surgery.15,16 Case series of laparoscopic procedures published in the 1990s led to the wide acceptance of bariatric surgery. In that period, many new procedures of bariatric and metabolic surgery were introduced, with more or less success. SG was also introduced as a component of biliopancreatic diversion with duodenal switch. 17
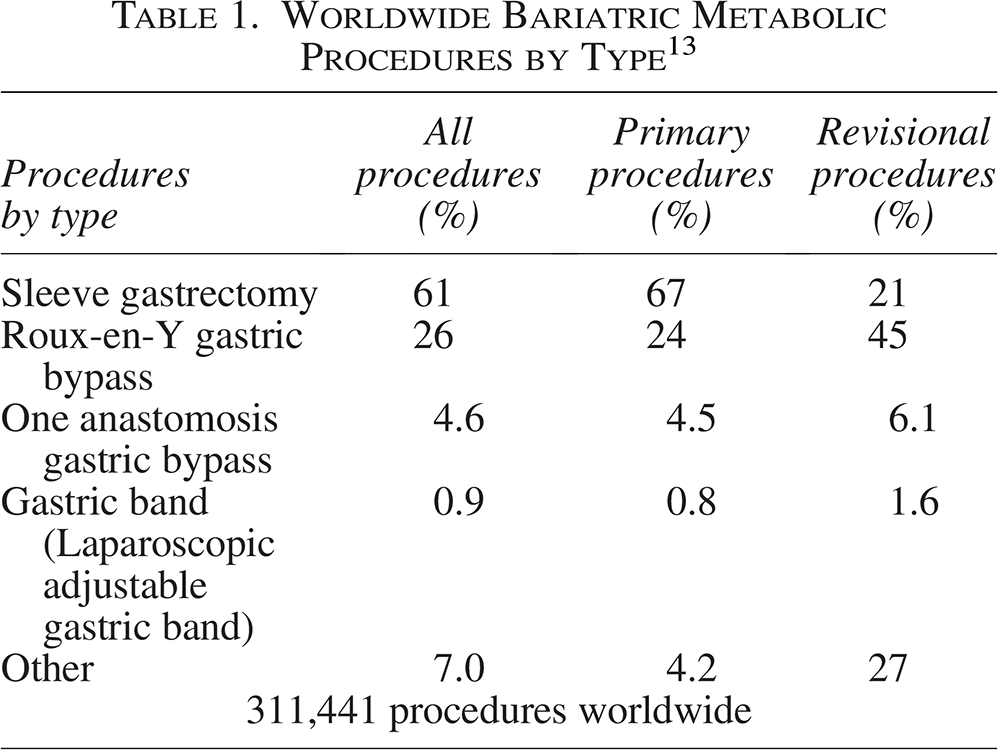
Today, SG and RYGB are mostly performed procedures in bariatric metabolic surgery, SG making 61% of overall procedures, 67% of primary procedures, and 21% of revisional procedures, and RYGB making 26% of overall procedures, 24% of primary procedures, and 45% of revisional procedures. The third most common procedure in the World is OAGB, making 4.6% of overall procedures and 4.5% of revisional procedures. 13 Summary from 6th IFSO Global Registry Report can be seen in Table 1. Both RYGB and SG result in sustained 5-year weight loss control. There is a significantly greater percentage excess weight loss (%EWL) in patients undergoing RYGB compared with SG (65.7% vs. 57.3%). 18
Worldwide Bariatric Metabolic Procedures by Type 13
Complications from bariatric and metabolic surgery exist even in the most technically gifted hands. Early recognition of complications can be lifesaving. Laparoscopy was introduced to bariatric and metabolic surgery in the 1990s. Laparoscopic procedures improved mean operative times, intraoperative blood loss, intensive care stay length, postoperative pain, in-hospital stay, faster recovery, morbidity, and mortality rates. For laparoscopic RYGB, 30-day mortality rates are 0.2–1.9%, with established risk factors: higher BMI, gender (male), age, and comorbidities. 19 Early complications leading to mortality are anastomotic leak with sepsis and pulmonary embolus. Perioperative morbidity rate is 23.6%, resulting from anastomotic leak, hemorrhage, marginal ulceration, wound infection, deep vein thrombosis, small bowel obstruction or trocar site hernia, internal hernia (e.g., Peterson’s hernia), or anastomotic site intussusception. Late complications include anastomotic dilation or stricture, biliary tract pathology, gastric remnant fistula, weight regain, and metabolic/nutritional complications. 20 Laparoscopic SG has a 30-day mortality rate of 0.1% and relatively few complications. German bariatric registry reports a leak rate of 0.9%. 21
The three most useful methods of bariatric surgery, SG, OAGB, and RYGB, used in the treatment of obesity, have also been shown to be successful in the treatment of type 2 diabetes. Some high-quality trials have proven the superiority of bariatric and metabolic surgery in diabetes remission over conventional drug therapy. Up to 60% of patients achieve remission of type 2 diabetes. 22 Remission is sustained in younger patients with shorter period of illness and less diabetes-related complications. 23 Meta-analysis of SG impact on diabetes mellitus type 1 (T1DM) also showed excellent short-term weight-reducing effects and reduced insulin requirement in obese patients with T1DM. 24 According to some trials, the glycemic control of both methods has been shown to be equally successful, while some describe the better effectiveness of RYGB. However, there are differences in the degree of diabetes remission. The STAMPEDE trial, which examined patients with obesity and uncontrolled type 2 diabetes, showed that patients who underwent RYGB had greater weight loss and needed less medication to achieve glycemic control, while both methods had a similar effect on achieving glucose control. OAGB had statistically significantly better outcomes compared with RYGB and SG regarding diabetes mellitus type (T2DM) remission and %EWL at 5 years, suggesting diabetic patients with cardiovascular risk factors, such as hypercholesterolemia, to receive bypass surgery.7,23,25–34
After bariatric and metabolic surgery, comorbidities also improve or resolve. Hyperlipidemia improves in 70% of patients. Hypertension resolves in 61.7% of patients and disappears or improves in 78.5% of patients. Obstructive sleep apnea disappears in 85.7% of patients and disappears or improves in 83.6% of patients. 35
Impact of bariatric and metabolic surgery on glucose homeostasis
Type 2 diabetes is known to us as a chronic, unstoppable, irreversible metabolic disease. Guidelines and numerous studies indicated the need for good and rapid intensification of well-known pharmacological therapy in order to achieve the desired glycemia.3,27 Despite this, the disease is still progressive, and over 50% of patients become dependent on insulin within 9–10 years. 27 Recent research focused on the new goals of diabetes treatment—achieving remission or reversal.
Bariatric and metabolic surgery can reverse T2DM for 60% of patients. The American Diabetes Association, the Endocrine Society, European Association for the Study of Diabetes, and Diabetes UK have adopted a definition of remission: HbA1c <6.5% (48 mmol/mol) measured at least 3 months after cessation of glucose-lowering pharmacotherapy. As already mentioned, achieving remission is possible with pharmacotherapy, lifestyle changes, and bariatric and metabolic surgery. In this, bariatric and metabolic surgery proved to be the most successful and long-term solution. 36 Remission itself and improvement of glycemia after bariatric and metabolic surgery are achieved through several mechanisms. Because of changes in the intestinal anatomy and physiology, food enters the gastrointestinal tract faster and bypasses the “proximal” bowel, which has endocrine activity and leads to the expression of intestinal genes that are involved in fatty acid, triglyceride, and cholesterol synthesis.2,27 Postoperatively, there is reduced caloric intake, which contributes to further weight loss, lower insulin needs, and improved insulin sensitivity in the liver (reduced gluconeogenesis and improved lipid metabolism), adipose, and skeletal muscle.2,4,27 Postoperatively, reduced need for insulin, reduced glucotoxicity, and reduced peripheral insulin resistance improve the function of β cells and promote their regeneration. 22
Hormonal changes also occur. The level of GLP-1, gastric inhibitory peptide, peptide YY, ghrelin, and bile acids increases postprandially. Together, they contribute to glucose homeostasis.2,3,5,27 The gut hormone secretion increase has been explained through different mediators depending on the type of surgery. For RYGB, bile acids or changes in the gut microbiome have been described as possible mediators—bile acids indirectly regulate glucose through the G-protein-coupled bile acid receptor, Gpbar1 (TGR5) receptor expressed on L-cells, causing release of GLP-1 when binding.35–40 GLP-1 also has specific effects on the pancreas. It prevents beta cell apoptosis, stimulates glucose-induced insulin secretion, and increases the mass of beta cells. 22
Changes in amino acid levels were also observed, which correlate with changes in insulin secretion and insulin sensitivity. 27
After bariatric and metabolic surgery, significant changes were observed in the gut microbiome, which has metabolic, immunological, and neural functions in the body. Recent studies have proven that RYGB improves tight-junction integrity, which improves intestinal permeability. It leads to the reduction of metabolic endotoxemia and systemic inflammation. 22 An increase in the diversity of the microbiota after bariatric and metabolic surgery has been proven through scientific works, but it is still necessary to conduct numerous studies in order to understand its role in the treatment of metabolic diseases.2,27
T2DM reversal is real
Many works indicate the success of achieving reversal and remission of diabetes. Bariatric and metabolic surgery has proven to be the most successful in this through numerous studies. In the Swedish Obesity Study, of 343 patients who underwent bariatric surgery, 72.4% achieved diabetes remission at 2 years, compared with only 16.4% of control patients. Also, a 2019 study showed that 74% of patients who underwent RYGB had diabetes remission at 1 year. 5 Moradi et al. showed in their study that 74.8% of patients had complete remission of type 2 diabetes after 1 year, and remission was extended to 3 years in 79.4% of patients. 7 But after achieving a reversal, it is necessary to invest a lot of knowledge and effort to turn that reversal into a permanent remission. However, after achieving remission, the question of metabolic memory and its role in achieving permanent remission arises. As the effect of bariatric and metabolic surgery on achieving glycemic control is not the same, previous studies have observed the existence of predictive factors. For now, it is known that these include duration of diabetes, degree of medication use, glycemic control, BMI, comorbidities, patient age, C-peptide levels.3,41 Moradi et al. also showed that the best predictor factors for achieving remission are younger patients, higher preoperative BMI, lower HbA1c, shorter duration of diabetes, no insulin therapy, and a negative family history of obesity. 7 These predictive factors will certainly be of great use when choosing a treatment method with the aim of achieving remission.
Along with all the benefits of bariatric surgery, postbariatric hypoglycemia should also be mentioned. It is an extreme drop in glucose levels after surgery. It is most often reported after RYGB, but it occurs with other methods of bariatric surgery. 27 The prevalence of hypoglycemia after bariatric and metabolic surgery depends on the methods of determination. Studies have shown that <1% have severe hypoglycemia requiring hospitalization, and 10–30% have hypoglycemia with self-reported symptoms.42,43
Conclusion
Fighting with two global unstoppable pandemics, which have led to an increase in mortality and morbidity, there has been significant progress in the development of therapeutic methods. Through the evidence of numerous studies, bariatric and metabolic surgery has proven to be the most effective method and a method with a long-term effect. The three most commonly performed methods of bariatric and metabolic surgery, SG, OAGB, and RYGB, have proven their benefits on various metabolic levels, both in glucose homeostasis, weight reduction, regulation of serum lipid levels, blood pressure, renal function, and other metabolic parameters. 2 But despite the significant benefits achieved by bariatric and metabolic surgery, the reversal and remission of diabetes is still not achieved in some patients. Predictive factors play an important role in this. Therefore, it is difficult and not at all simple to choose the best therapeutic option in obese patients with type 2 diabetes, with which we will be able to achieve reversal and remission of the disease. In addition to choosing the most effective therapy, patient compliance is equally important to us. Further studies will be needed to point out the open questions of the benefits and risks of bariatric and metabolic surgery.
Authors’ Contributions
A.P.: Conceptualization, writing, data curation, formal analysis, investigation, and methodology. J.V.Š.: Writing, data curation, formal analysis, investigation, and methodology. M.S.: Data curation, formal analysis, investigation, and methodology. D.Š.: Conceptualization, supervision, and validation.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.